


Abstract
Background: The benefits of self-monitoring blood glucose levels are unclear in patients with type 2 diabetes mellitus who do not use insulin, but there are considerable costs. We sought to determine the cost effectiveness of self-monitoring for patients with type 2 diabetes not using insulin.
Methods: We performed an incremental cost-effectiveness analysis of the self-monitoring of blood glucose in adults with type 2 diabetes not taking insulin. We used the United Kingdom Prospective Diabetes Study (UKPDS) model to forecast diabetes-related complications, corresponding quality-adjusted life years and costs. Clinical data were obtained from a systematic review comparing self-monitoring with no self-monitoring. Costs and utility decrements were derived from published sources. We performed sensitivity analyses to examine the robustness of the results.
Results: Based on a clinically modest reduction in hemoglobin A1C of 0.25% (95% confidence interval 0.15–0.36) estimated from the systematic review, the UKPDS model predicted that self-monitoring performed 7 or more times per week reduced the lifetime incidence of diabetes-related complications compared with no self-monitoring, albeit at a higher cost (incremental cost per quality-adjusted life year $113 643). The results were largely unchanged in the sensitivity analysis, although the incremental cost per quality-adjusted life year fell within widely cited cost-effectiveness thresholds when testing frequency or the price per test strip was substantially reduced from the current levels.
Interpretation: For most patients with type 2 diabetes not using insulin, use of blood glucose test strips for frequent self-monitoring (≥ 7 times per week) is unlikely to represent efficient use of finite health care resources, although periodic testing (e.g., 1 or 2 times per week) may be cost-effective. Reduced test strip price would likely also improve cost-effectiveness.
See related research article by Gomes and colleagues, page 35
Self-monitoring of blood glucose in patients with diabetes who use insulin may contribute to improved glycemic control and reduced hypoglycemia by allowing for self-adjustments in insulin dose to be made based on meter readings. 1 Self-monitoring may also allow for appropriate changes in diet and physical activity to be made. However, the benefits of self-monitoring of blood glucose for patients not using insulin are less clear. Hypoglycemia is less frequent in this population 2 and is confined mainly to those taking secretagogues. The degree to which patients can adjust the dose of oral antidiabetes drugs in response to readings is limited.
Nevertheless, self-monitoring of blood glucose is routinely recommended for patients who are not using insulin. 1 This results in major investments in this technology by patients and payers. 3 In 2006, $250 million was spent on blood glucose test strips in 8 publicly funded drugs plans in Newfoundland and Labrador, Nova Scotia, Quebec, Ontario, Manitoba, Saskatchewan and British Columbia, while over $120 million was spent in privately funded drug plans in Canada. 4 In some publicly funded drug plans in Canada, blood glucose test strips are among the top 5 classes in terms of total expenditure, 5 with costs exceeding those for all oral antidiabetes drugs combined. 4,6 It is estimated that more than 50% of the total expenditure on blood glucose test strips is for patients with type 2 diabetes who are not using insulin. 3 Costs related to test strips are expected to rise steadily 5,7 because of the increasing prevalence of type 2 diabetes. 8
Decisions about the prescribing and reimbursement of blood glucose test strips require consideration of information about the costs and clinical benefits. 9,10 As part of a larger initiative to determine the optimal use of this technology, we sought to determine the cost-effectiveness of self-monitoring of blood glucose for patients with type 2 diabetes who do not use insulin, based on data from our systematic review 11 of the available clinical evidence.
Methods
Model and data sources
We performed an incremental cost-utility analysis of self-monitoring of blood glucose using the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model. This computer simulation model forecasts long-term health outcomes and cost consequences in patients with type 2 diabetes (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090765/DC112) The model estimates the risks of 7 diabetes-related complications based on data obtained from 3642 patients with type 2 diabetes who were enrolled in UKPDS. Projections from this model have been validated using published clinical and epidemiological studies. 13
Relevant clinical outcomes associated with self-monitoring of blood glucose in adults with type 2 diabetes not using insulin were derived from our systematic review 11 of randomized controlled trials and observational studies comparing self-monitoring with no self-monitoring. We assessed a number of outcomes, including hemoglobin A1C (HbA1C), hypoglycemia, quality of life, long-term complications of diabetes and mortality. The methodology and results of the review have been reported in full. 11
The UKPDS model simulates the occurrence of clinical events over the expected remaining lifetime of a patient with type 2 diabetes (maximum 40 years). Simulated patients were characteristic of those enrolled in randomized controlled trials included in the systematic review. 11 The ages and baseline risk factors for diabetes-related complications of the simulated patients (e.g., baseline HbA1C level, systolic blood pressure, cholesterol level) have been reported. 14 Data on the history of 7 major diabetes-related complications captured in the UKPDS Outcomes Model (Appendix 1) were not reported in the randomized controlled trials included in the systematic review. Therefore, we assumed that patients in the hypothetical cohort in the base-case analysis did not have a history of these complications. We made this assumption because most randomized controlled trials excluded patients with impending diabetes-related complications or a history of serious disease, and because less than 1% of patients in Canada with type 2 diabetes aged 45–65 years have a history of stroke, blindness, amputation or renal disease. 14–16
We performed this analysis from the perspective of a Canadian ministry of health. 17 We obtained the unit costs for blood glucose test strips ($0.73/strip) and dispensing fees ($7.00 per 100 strips) from the Ontario Public Drug Program. 18,19 We did not incorporate the costs for glucometers and lancets, because they are often made available to patients at no charge by manufacturers 20 and they are usually not covered by public drug plans. We assumed an average daily consumption of 1.29 blood glucose test strips per patient on the basis of the weighted average of actual (where reported) or per-protocol testing frequencies across randomized controlled trials included in the systematic review. This estimate closely coincided with the results of a recent utilization study of Ontario Public Drug Program beneficiaries. 3
Resource utilization and costs (Table 1) associated with managing diabetes-related complications were obtained from the Ontario Ministry of Health and Long-term Care. 23 Inpatient, outpatient and emergency department visits, prescription drug claims, long-term care and home care costs for managing diabetes-related complications were included in the model. 23 The costs were inflated to 2008 Canadian dollars using the Health Component of the Canadian Consumer Price Index. 26
Table 1: Modelled management costs and utility decrements
Both costs and quality-adjusted life-years were discounted at a rate of 5%, as recommended by the guidelines of the Canadian Agency for Drugs and Technologies in Health. 17
Outcomes
The primary outcome measure in the current analysis was quality-adjusted life-years, which capture both quantity and quality of life. We obtained quality weights for included health states from a US catalogue of EuroQol 5-dimension (EQ-5D) scores. 21,22 Patients with noninsulin-treated type 2 diabetes without a history of diabetes-related complications were assumed to have an EQ-5D score of 0.753. 21,22 Disutilities associated with diabetes-related complications are reported in Table 1. 21–24
Statistical analysis
We performed 1-, 2- and multi-way sensitivity analyses to examine the robustness of the results to changes in the parameters and model assumptions. A number of randomized controlled trials included in the systematic review included patients who were taking either oral antidiabetes agents or made lifestyle interventions. We therefore assessed the effect of HbA1C inputs derived from pooling across the subset of randomized controlled trials in which all patients received oral antidiabetic agents or those in which all patients received non-pharmacological interventions. We tested the effect of varying the cost of the test strips, testing frequency, baseline HbA1C levels and patient characteristics. We also tested including a utility decrement for symptomatic hypoglycemia. The detailed results from additional sensitivity analyses are reported elsewhere. 27 We generated cost-effectiveness acceptability curves for the reference case, as well as for alternative testing frequencies and test strip prices, to illustrate the probability that the self-monitoring of blood glucose is cost-effective across a range of decision-makers’ willingness-to-pay thresholds. 28
Results
Our systematic review 11 identified 7 randomized controlled trials, 29–35 enrolling a total of 2270 patients with type 2 diabetes managed with oral antidiabetes agents or lifestyle measures alone. These trials compared self-monitoring of blood glucose with no self-monitoring. The pooled difference in HbA1C was statistically significant in favour of self-monitoring (weighted mean difference −0.25%, 95% confidence intervals [CI] −0.36% to −0.15%). The results were similar in a number of subgroup analyses, including the intensity of education about the interpretation and application of the test results, testing frequency, diabetes duration and baseline HbA1C level. Based on limited evidence, self-monitoring has failed to show consistent benefits in terms of quality of life, patient satisfaction, hypoglycemia, long-term complications of diabetes and mortality. These outcomes were therefore not included in the cost-effectiveness analysis of the reference case.
The HbA1C benefit of self-monitoring from the systematic review, 11 when analyzed using the UKPDS Outcomes Model, translated into small differences (ranging from 0.08% to 0.40%, depending on the outcome) in cumulative incidence rates of diabetes-related complications (Table 2). The numbers of patients who would need to perform self-monitoring to avert 1 diabetes-related complication over a 40-year period ranged from 228 to 1299 (Table 2). Self-monitoring of blood glucose was associated with an additional 0.024 quality-adjusted life-years and increased lifetime costs of $2711, resulting in an incremental cost-utility ratio of $113 643 per quality-adjusted life-year gained (Table 3). Cost-effectiveness acceptability curves (Figure 1 and Figure 2) revealed a probability of less than 10% that self-monitoring would be cost-effective at a willingness-to-pay threshold of $50 000 per quality-adjusted life-year, and a 40% probability of cost-effectiveness at a threshold of $100 000 per quality-adjusted life-year. 10
Table 2: Cumulative incidence of diabetes-related complications over a 40-year period among patients with type 2 diabetes who do not use insulin who self-monitor their blood glucose levels and those who do not self-monitor
Table 3: Benefits, costs and incremental cost utility ratios for self-monitoring blood glucose levels among patients with type 2 diabetes not using insulin*

Figure 1: Cost-effectiveness acceptability curves for different prices per blood glucose test strip. These curves show the probability that performing self-monitoring of blood glucose (SMBG) is cost-effective relative to not performing self-monitoring in patients with type 2 diabetes who are not using insulin, across a range of decision-makers’ willingness to pay-thresholds.
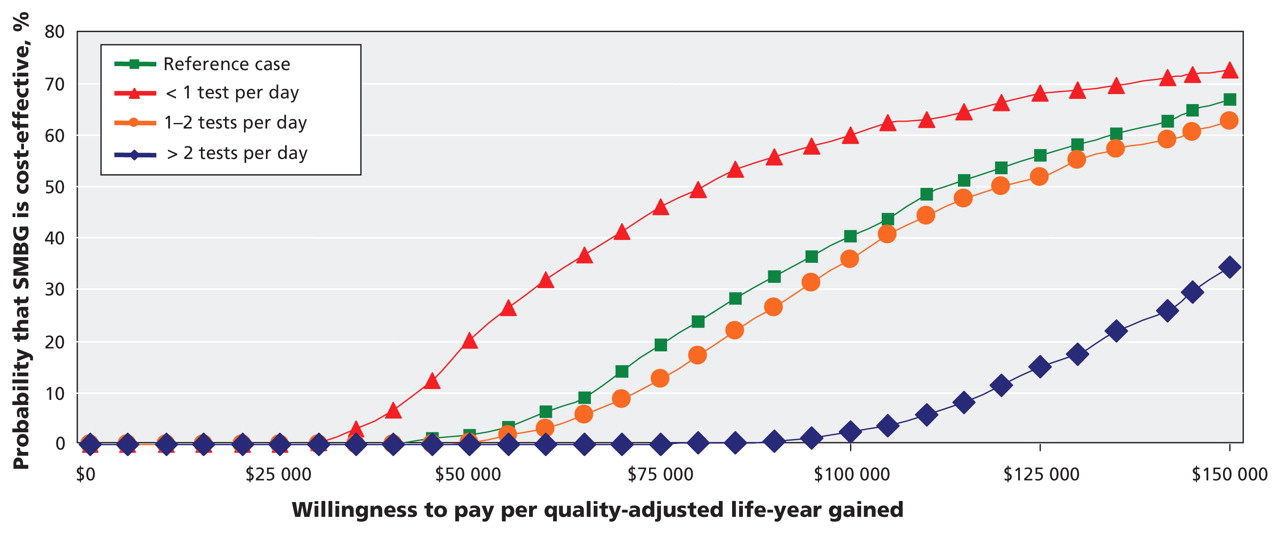
Figure 2: Cost-effectiveness acceptability curves for 2-way sensitivity analyses, in which HbA1C estimates of effect and self-monitoring of blood glucose (SMBG) testing frequencies were both varied.
The reduction in HbA1C associated with self-monitoring in the only randomized trial that reported results for patients not using pharmacotherapy for diabetes 30 was smaller than in the overall analysis (weighted mean difference −0.05%, 95% CI −0.23 to 0.33), resulting in a cost per quality-adjusted life- year gained of $292 144. The cost per quality-adjusted life- year based on the pooled HbA1C difference in the subset of randomized controlled trials 30,31,35 in which all patients used oral antidiabetes agents was $91 724 per quality-adjusted life-year gained. The results were highly sensitive to the price of the test strips and, to a lesser extent, testing frequency (Table 4;Figure 1 and Figure 2), 1,2,7, 14–16,23,29–42 but the results were largely unchanged if we varied most other parameters and assumptions.
Table 4: Incremental cost-utility ratios for the comparison of self-monitoring of blood glucose with no self-monitoring in patients with type 2 diabetes not using insulin
Interpretation
Our cost-effectiveness analysis was based on a systematic review of the available clinical evidence, 11 which showed a clinically modest 43 benefit in HbA1C levels among patients with type 2 diabetes who self-monitored their blood glucose levels. This result translated into a small reduction in diabetes-related complications in the economic model. We found that self-monitoring at a frequency of about 9 tests per week was associated with an incremental cost of $113 643 per quality-adjusted life-year gained, relative to no self-monitoring. Thus, the clinical benefits of self-monitoring and the associated cost-savings do not offset the cost of the blood glucose test strips.
In our sensitivity analyses, we explored conditions under which cost-effectiveness estimates may vary. The results did not change substantially with changes in the assumed HbA1C benefit of self-monitoring, higher baseline HbA1C levels, or when the cohort was modified to reflect patient characteristics (e.g., diabetes-related complications, duration of diabetes) observed in the Canadian setting (Table 4). Cost-effectiveness estimates, however, were highly sensitive to changes in the price per test strip and testing frequency. Cost-effectiveness acceptability curves showed that a greater than 50% reduction in the price per test strip would result in a substantial increase in the probability that self-testing is cost-effective. Results from 1- and 2-way sensitivity analyses also suggested that lower testing frequencies (e.g., 1–2 tests per week) would be the most likely to yield favourable cost-effectiveness estimates. This is not surprising because the incremental HbA1C benefit of each subsequent test per day is likely to be progressively smaller, while the cost of test strips increases linearly with the number used. Further well-designed randomized controlled trials are needed to assess the role of self-monitoring at lower testing frequencies in patients with type 2 diabetes who are not using insulin.
Our results differ from those reported in earlier incremental cost-utility analyses. 36,44,45 Two of the previous studies 36,44 found more favourable cost-effectiveness estimates, likely because of the use of data from an observational study, 37 which found larger HbA1C differences in favour of self-monitoring than our systematic review. Conversely, the other economic study 45 reported results less favourable to self-monitoring primarily because the HbA1C results were from a single clinical trial. Differences in utility decrements may also explain some of the differences in the results between these studies. Health-related quality-of-life scores in 2 earlier analyses 36,44 were based on data from patients with type 2 diabetes 24 and the authors did not control for nondiabetes-related complications and other confounding variables such as income, education, ethnicity and number of comorbidities, all of which affect health-related quality of life. In contrast, we obtained utility decrements from a community-based EQ-5D catalogue in the United States, 21,22 which was adjusted for determinants of health (e.g., age, sex, income, education) and chronic conditions other than diabetes.
The choice of economic model may also contribute to differences between our analysis and previous studies. We used the UKPDS Outcomes Model, 12 while 2 previous studies 36,44 used the Center for Outcomes Research (CORE) Diabetes Model. 46 The UKPDS Outcomes Model uses updated regression equations derived from UKPDS68, 12 while the CORE Diabetes Model 46 uses regression equations derived from the older UKPDS56 Risk Engine. 47 Thus, the UKPDS Outcomes Model 12 provides a more accurate estimate of events examined in UKPDS because it uses a wider variety of inputs, including knowledge of previous events, and incorporates updated risk factor data over time. 36
Limitations
Our study had several limitations. First, cost-effectiveness results are limited by available clinical evidence. 11 Second, the model used HbA1C, a surrogate outcome, to project the occurrence of long-term consequences related to diabetes. The validity of this outcome continues to be debated in the literature, particularly for cardiovascular outcomes in patients with type 2 diabetes. 48,49 Thus, the benefits of self-monitoring blood glucose in terms of reduced rates of complications may be overstated. Third, the UKPDS model 36 does not explicitly incorporate a number of morbidities (e.g., peripheral neuropathy, ulceration) related to diabetes. As well, some complications are represented as a single outcome (e.g., blindness, end-stage renal disease) in the model rather than intermediate states such as (e.g., retinopathy, nephropathy) that may themselves be associated with reduced health-related quality of life. Since a reduced incidence of these outcomes because of self-monitoring and the resulting benefits in terms of health-related quality of life and reduced treatment costs may not be captured, the use of the UKPDS model may result in a slight overestimation of the incremental cost-effectiveness ratios. 12 Long-term follow-up data from UKPDS may provide additional data for these states, at which time a reassessment of the cost-effectiveness of self-monitoring in patients with type 2 diabetes may be warranted.
Finally, the analysis of the reference case did not incorporate hypoglycemic episodes, including severe hypoglycemia. Episodes of hypoglycemia, however, are infrequent 2 in patients with type 2 diabetes not using insulin, with the exception of those using insulin secretagogues (i.e., sulfonyureas, meglinatides). Additionally, there is little evidence that use of self-monitoring alters the risk of hypoglycemia, even in patients using sulfonylureas. 35 If future studies reveal that self-monitoring of blood glucose is associated with a reduced risk of hypoglycemia, especially severe hypoglycemia, this analysis should be revisited given the potential impact of this complication on clinical outcomes and resource utilization.
Conclusion
We found that self-monitoring of blood glucose was associated with a modest reduction in HbA1C in patients with type 2 diabetes not treated with insulin. Within the limitations of modelling and the available clinical data, frequent use of self-monitoring in this population is associated with unfavourable cost-effectiveness estimates and is unlikely to represent an efficient use of finite health care resources. This result did not change substantially with changes to a number of inputs, including the type of antidiabetes therapy, degree of glycemic control at baseline and history of diabetes-related complications. However, reduced frequency (e.g., 1 or 2 times per week) or a reduction in the price of test strips would likely improve the cost-effectiveness of routine self-monitoring in this population.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: Scott Klarenbach and Ehud Ur have received honoraria for participation in the COMPUS Expert Review Committee. None declared for Chris Cameron and Doug Coyle.
Contributors: All of the authors contributed to the conception and design of the study. Chris Cameron conducted the analysis, and all authors assisted in the interpretation of the results. Chris Cameron, with the help of Scott Klarenbach, Doug Coyle and Ehud Ur, drafted the manuscript. All of the authors critically reviewed the manuscript for important intellectual content and approved the final version submitted for publication.
Funding: This cost-effectiveness was conducted by researchers at the Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH is an independent, not-for-profit agency funded by Canadian federal, provincial and territorial governments to provide credible, impartial advice and evidence-based information about the effectiveness of drugs and other health technologies to Canadian health care decision-makers. For more information, visit www.cadth.ca.
Acknowledgements: The authors thank Melissa Severn for developing and implementing the literature search strategies, Heather Bennett for her input into study design and Sumeet Singh and Denis Belanger for their critical review of the manuscript. Scott Klarenbach is supported by Population Health Investigator Award from Alberta Heritage Foundation for Medical Research.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Cost-effectiveness of Interventions to Manage Diabetes: Has the Evidence Changed Since 2008?
- Reduction in self-monitoring of blood glucose in type 2 diabetes: an observational controlled study in east London
- Approach to economic evaluation in primary care: Review of a useful tool for primary care reform
- Self-Monitoring of Blood Glucose in Noninsulin-Using Type 2 Diabetic Patients: It is time to face the evidence
- Routine self-monitoring of blood glucose
- Daily self-monitoring unlikely to be cost-effective in adults with type 2 diabetes not using insulin in Canada
- The author responds:
- Missing the boat
More in this TOC Section
Similar Articles

