


After an uneventful pregnancy and delivery, a healthy male infant was born at 39 weeks' gestation and circumcised by his family physician on the sixth day of life. In the subsequent 36 hours, the boy continued to wet diapers, but had progressive irritability and lethargy, and was brought back to the family physician for reassessment at the age of 8 days. His lower abdomen and lower limbs were noted to be mottled, cyanosed and edematous, and the boy was referred to a local pediatrician who was concerned about a possible acute inferior vena cava thrombosis.
A full abdominal examination of the unconsolable infant was impossible, however, a very slow but continuous dribble of urine was noted despite a Plastibell circumcision ring that may have been partly obstructing the urethral meatus. A urethral catheterization was attempted, but this could not be achieved because of meatal obstruction.
The infant remained irritable, but his vital signs were stable. His abdominal distension and lower extremity venous congestion and cyanosis were confirmed. Portable abdominal radiographs showed a massive distended bladder with evidence of lumbar scoliosis (Figs. 1 and 2). (Arrowheads denote bladder outline on radiographs.) The boy was thought to have a Plastibell ring urethral meatus obstruction leading to enlargement of the bladder, which blocked the inferior vena cava, resulting in acute venous stasis of the lower abdomen and extremities. Using a 25-gauge butterfly needle, 200 mL of urine was aspirated suprapubically. Subsequently, the infant appeared calmer and the Plastibell ring was successfully removed by cutting the string that held it in place. When trying to cut the string, it was noted that the ring was embedded in the glans penis. The baby proceeded to pass spontaneously over 600 mL of urine in the following 12 hours. Over the next 36 hours he continued to urinate, and his venous engorgement and cyanosis disappeared. His penis appeared normal. The patient had no further problems or complications.
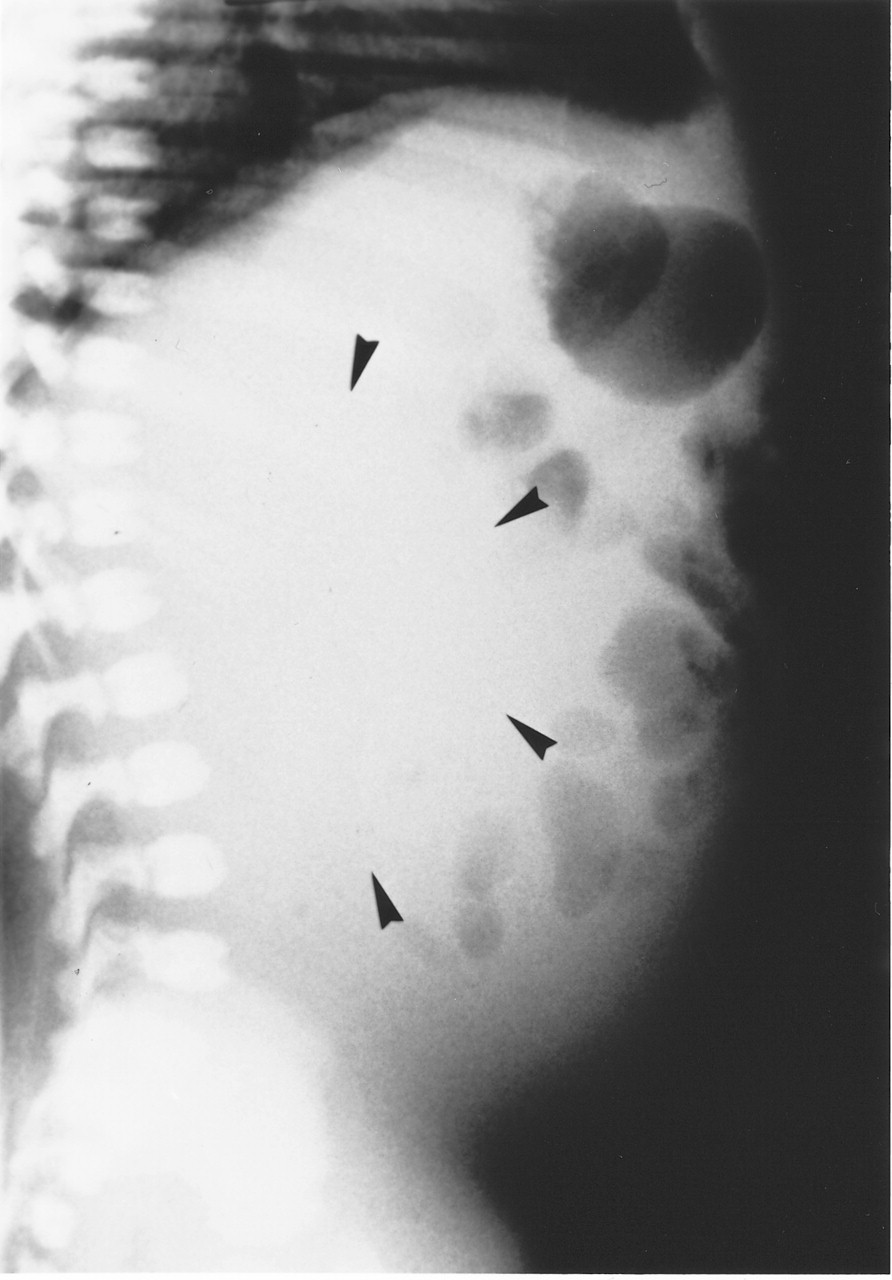
Figure 2. Photo: Images courtesy of the Department of Medical Images, Royal University Hospital

Figure 1. Photo: Images courtesy of the Department of Medical Images, Royal University Hospital
Although circumcision is routinely practised by some groups for religious and cultural reasons, the routine practice of circumcision is not recommended.1 In its latest policy statement in 1999, the Task Force on Circumcision, established by the American Academy of Pediatrics, concluded that the scientific evidence at that time was not sufficient to recommend routine neonatal circumcision.2 This position was also supported by the Canadian Pediatric Society.3 In Saskatchewan circumcision is not an insured service; parents have to pay for it.4
The devices that have been used for medical circumcision include the Plastibell device, the Gomco clamp5 and the Mogen clamp. The Plastibell device is used as follows. After adequate analgesia, a slit is made in the foreskin, the end ring of the Plastibell device is placed over the glans, and the foreskin is pulled over the ring. A ligature is tied tightly around the foreskin, which is then cut off. The bell of the device is removed, and the end ring falls off a few days later.
In a review of the Plastibell device used in about 2000 cases of neonatal circumcision, the incidence of complications was 1.8%, the most frequent being minor infection and hemorrhage. Other complications included a tight Plastibell ring that can cause constriction of the glans penis, irregular skin margin, inadequate skin excision and migration proximally of the Plastibell ring as the glans swells with venous engorgement.6 There have been isolated cases of necrotizing fasciitis,7,8 ruptured bladder,9 retention of urine secondary to glandular prolapse,10,11 and retention of the Plastibell device.12 In the case described here, the difficulty experienced in removing the Plastibell ring was consistent with retention of the device.
In this case, venous stasis is presumed to have occurred post circumcision when the boy's distended bladder caused acute vena caval obstruction. The continuous dribbling of urine led to initial assumptions that there was no urinary retention, and complete examination of the abdomen, which would have allowed the detection of a palpable urinary bladder, was impeded by the child's irritability. The abdominal radiographs that revealed the grossly distended bladder helped significantly in the definitive management of this infant. Children with a similar presentation post circumcision should be evaluated for this uncommon but easily reversible form of venous obstruction.
Linh Ly Koravangattu Sankaran Department of Pediatrics College of Medicine Royal University of Saskatchewan Saskatoon, Sask.
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

