


- © 2004 Canadian Medical Association or its licensors
Readers of CMAJ were first alerted to the rising incidence of ciprofloxacin-resistant Neisseria gonorrhoeae infection in Canada last year.1 On the basis of this trend, the recommended treatment for gonorrhea in some areas of Canada and for some infected patients has changed.
The reported rate of gonorrhea in Canada reached its lowest point in 1997, but since that year, following more than 2 decades of decline, the rate has increased by over 60% to 24.3 per 100 000 (7363 cases) in 2003 (preliminary unpublished data from the Sexual Health and STI Section, Public Health Agency of Canada).
Gonorrhea is caused by N. gonorrhoeae infection, and common clinical manifestations include urethritis and cervicitis. Uncomplicated cases of gonorrhea can be treated with single-dose antimicrobial therapy, which helps to ensure compliance. However, emerging and prevalent antibiotic-resistant strains of N. gonorrhoeae limit therapeutic choices. Penicillin- and tetracycline-resistant strains of N. gonorrhoeae are well documented around the world, and therefore penicillin and tetracycline are not recommended for the treatment of gonorrhea. Fluoroquinolone (FQ) resistance was first identified in 1992. FQ resistance is currently most prevalent in the Far East, but it has been documented in many parts of the world, including the UK, the United States and Canada.2
Once resistance rates to an antibiotic reach 3%–5%, the antibiotic can no longer be recommended. Box 1 lists the areas and populations for which FQs are not recommended for treatment of gonorrhea.

Preliminary national FQ resistance rates in Canada have been reported to be 2.1% in 2002 and 2.0% in 2003 (unpublished data, National Microbiology Laboratory). These rates are calculated using the number of N. gonorrhoeae isolates that test resistant to ciprofloxacin (minimum inhibitory concentration ≥1.0 mg/L) as the numerator with the total number of N. gonorrhoeae isolates tested each year as the denominator. Before 1997 the number of isolates tested by the NML was close to the total number of national gonorrhea cases reported; however, this is no longer the case. In 2003, the number of isolates submitted for antibiotic resistance testing nationally was 4726, and the preliminary number of gonorrhea cases reported nationally was 7363. The drop in national resistance testing can be explained at least in part by the growing use of diagnostic methods other than culture, such as nucleic acid amplification testing (e.g., polymerase chain reaction and ligase chain reaction), which preclude antimicrobial resistance testing.
Although the national rate remained under 3% in 2003, data on FQ resistance from individual provinces and territories indicate that the rate of resistance is actually much higher in some jurisdictions. Some provincial laboratories are reporting FQ resistance rates of at least 10% for those isolates submitted for testing.
There are 4 recommended treatments in Canada for uncomplicated urethral, endocervical, rectal and pharyngeal infections (Box 2). Ciprofloxacin and ofloxacin should not be used in cases where the risk of FQ resistance is significant (Box 1). It is important to note that regions within Canada and the US are included in this list. Physicians in Canada who are treating gonorrhea are advised to seek information, if available, from local public health authorities about the level of FQ resistance in their area. If the risk of FQ resistance is significant, the recommended treatments are limited to cefixime or ceftriaxone.
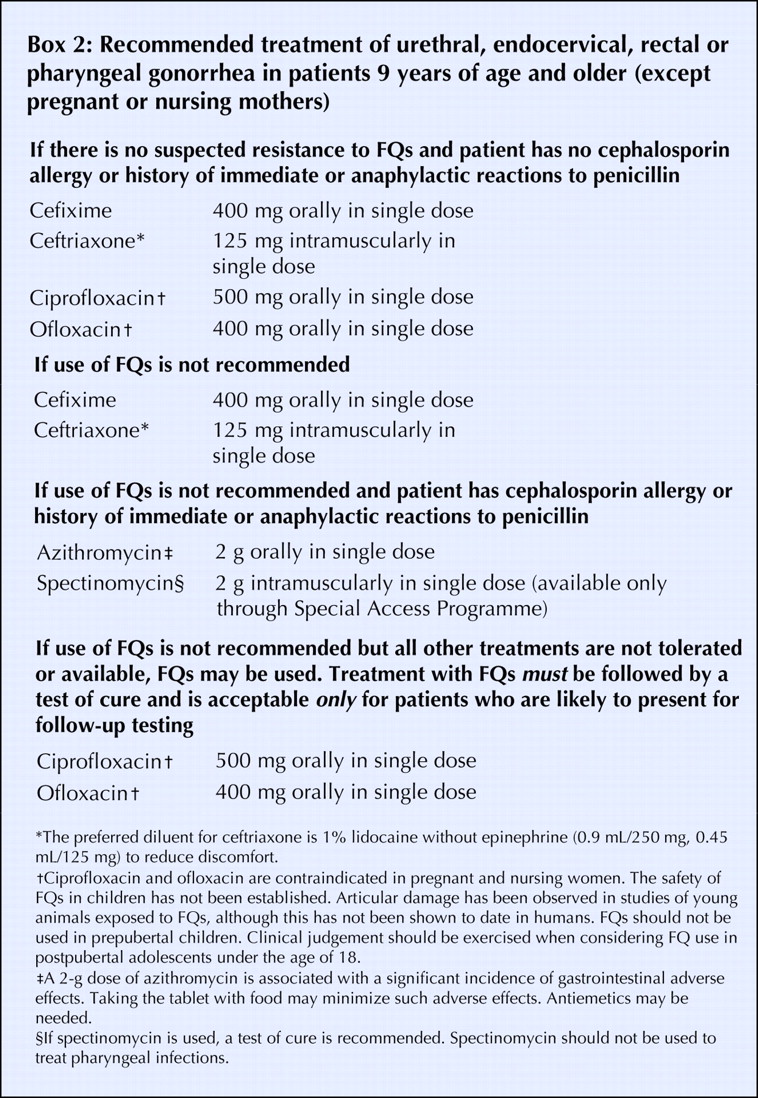
If allergy precludes the use of ceph a losporins, treatment recommendations include azithromycin or spectinomycin. A 2-g dose of azithromycin is associated with a significant incidence of gastrointestinal adverse effects. Taking the tablet with food may minimize such adverse effects. Antiemetics may be needed. In Canada, spectinomycin is available only through the Special Access Programme, Health Canada.
If because of tolerance or access issues azithromycin and spectinomycin cannot be used, and the case occurs in an area of significant FQ resistance, ciprofloxacin or ofloxacin may be considered for patients with allergies to cephalosporins. However, FQs may be used in this situation only if treatment is followed by a test of cure, and they are acceptable only for patients who are likely to return for follow-up testing.
The recommended treatments for pregnant or nursing women and for children under the age of 9 remain unchanged. Physicians are referred to the 1998 Canadian STD Guidelines, available online at www.hc-sc.gc.ca/pphb-dgspsp/publicat/std-mts98/index.html.
Antibiotic-resistant strains of N. gonorrhoeae continue to challenge the treatment, prevention and control of this infection. Because of the availability and use of alternative testing methods that do not allow resistance testing, ongoing monitoring and reporting of antimicrobial resistance remains vital. As well, enhanced patient information beyond age and sex (e.g., whether the infection was derived from homosexual or heterosexual contact) would enable better targeting of health promotion strategies and public education campaigns. As such, a national sentinel surveillance system for the ongoing monitoring of resistance of N. gonorrhoeae to various antimicrobials, such as those in place in the UK and US, may need to be introduced in Canada.
For further updates on FQ-resistant N. gonorrhoeae in Canada, you may access the Sexual Health and STI Section Web site on the Public Health Agency of Canada Web site at: www.hc-sc.gc.ca/pphb-dgspsp/std-mts/.
Janice Mann Rhonda Kropp Tom Wong Sexual Health and STI Section Community Acquired Infections Division Centre for Infectious Disease Prevention and Control Public Health Agency of Canada Ottawa, Ont. Sylvie Venne Services des maladies infectieuses Direction générale de la santé publique Ministère de la Santé et des Services sociaux, Québec Montréal, Qué. Barbara Romanowski Division of Infectious Diseases Faculty of Medicine and Dentistry University of Alberta Edmonton, Alta.
Footnotes
-
To ensure the effective and appropriate treatment of gonorrhea in Canada, an Interim Statement on the Treatment of Gonorrhea in Canada has been produced and will be available on the Public Health Agency of Canada Web site at www.phac-aspc.gc.ca. The revised version of the Canadian STD Guidelines is targeted for release in autumn 2005 and will reflect the changes that have occurred in FQ resistance of N. gonorrhoeae since the 1998 edition.
Acknowledgements: The treatment recommendations in this article were made in conjunction with the Expert Working Group for the Canadian STI Guidelines and the provincial and territorial STI Directors. We thank Lai King Ng and Mei Ling Lam from the National Microbiology Laboratory.
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

