


- © 2008 Canadian Medical Association
Cervical cancer affects 1300 Canadians annually and accounts for roughly 400 deaths.1 The staging system used in cervical cancer is clinically based. At present, the size of the primary lesion and clinical stage are the most common determinants that guide management of the disease. Surgery is the preferred treatment for early disease (≤ 1B1), and chemoradiotherapy is preferred for advanced disease (> 1B1). Several randomized trials of the surgical management of cervical cancer have identified adverse prognostic factors for recurrence and survival. These factors include large tumour size (≥ 4 cm), deep stromal invasion (outer third of cervical stroma), vascular space involvement, parametrial tissue invasion, positive surgical margins and lymph node metastasis.2,3 In the presence of these adverse factors, adjuvant postoperative radiotherapy is usually recommended. There is also evidence that, in patients with these high-risk factors, avoiding surgery and treating primarily with chemoradiation is equally effective in reducing morbidity.4
In this issue of CMAJ, Selman and colleagues5 have performed a systematic review and meta-analysis of the literature on the diagnostic accuracy of magnetic resonance imaging, computed tomography, positron emission tomography and sentinel node biopsy in determining lymph node status in patients with cervical cancer. They reviewed 4230 studies and included 72 in their final analysis using strict selection criteria. They concluded that sentinel node biopsy was the most accurate (positive likelihood ratio 40.8) and positron emission tomography the next most accuracte (positive likelihood ratio of 15.3) in determining lymph node involvement. Although magnetic resonance imaging and computed tomography are commonly used for lymph node assessment, the authors found that they were less effective (positive likelihood ratio for magnetic resonance imaging 6.4 and for computed tomography 4.3).
Selman and colleagues have provided valuable information on the accuracy of the 4 tests presented in their paper, but one can not help but wonder why sentinel node biopsy was included in the same category as the 3 imaging tests. The former is clearly a surgical procedure that involves a limited lymphadenectomy. Presumably, it was chosen because of its few purported side effects. The bulk of the literature on sentinel node biopsy focuses on the early stages of disease and exploring the use of sentinel lymph node identification as part of the extirpative surgical procedure, with the goal of minimizing operative and postoperative morbidity from the lymphadenectomy. It is this strategy that has been implemented in the surgical management of melanoma, breast cancer and vulvar cancer. The role of sentinel node biopsy in advanced disease is less clear. The data in this patient population suggest that the false-negative rate increases with the use of sentinel node biopsy.6 Moreover, because the sentinel lymph node in cervical cancer is primarily in the pelvis and standard radiation therapy fields encompass this area of potential spread, there is little clinical role for its use in the management of advanced disease.
Examples comparing the detection of positive lymph nodes using the three imaging methods are shown in Figure 1, Figure 2, Figure 3 and Figure 4. The applicability of a highly accurate imaging method will have different implications for patients in the early and advanced stages of disease. In early disease, the clinical challenge is to identify patients who have microscopic metastatic disease. Such patients stand to benefit most from adjuvant or primary chemoradiotherapy, thus avoiding surgery altogether. However, the low incidence of lymph node metastases in these patients will make it difficult for any imaging method to be useful in the clinical setting. Sentinel node biopsy is well-suited in this situation because it is commonly combined with the resection procedure, and because it has the highest positive likelihood ratio and lowest negative likelihood ratio. In contrast, Selman and colleagues report that positron emission tomography had a positive likelihood ratio of 15.3. Given that most studies of early cervical cancer reported a less than 10% incidence of lymph node metastases,7 the post-test probability for a positive positron emission tomography scan will be about 60%. Will this be sufficient to dictate a change in management of the disease? For patients with advanced cervical cancer, the challenge is to define the precise extent of disease (including para-aortic nodal and distant spread) so that appropriately tailored therapy can be provided. These patients are not likely to have surgery, and the extent and location of lymphatic metastases provides guidance for chemoradiotherapy. As mentioned earlier, in advanced disease the detection of a metastatic lymph node in the pelvis will unlikely help management decisions, and precise imaging methods that identify extrapelvic disease are absolutely required in these patients. With the limited data available, the precise positive likelihood ratio for positron emission tomography to identify para-aortic lymph node metastases is unknown.

Figure 1: Positron emission tomography scan (left) showing a positive supraclavicular lymph node. Computed tomography scan (right) of the same area illustrates the superior ability of positron emission tomography to identify metastatic disease.

Figure 2: Positron emission tomography scan (left) showing no evidence of metastases. The corresponding computed tomography scan is on the right.

Figure 3: Magnetic resonance imaging scan showing 2 prominent positive lymph nodes (arrows) abutting the right iliac vessels.
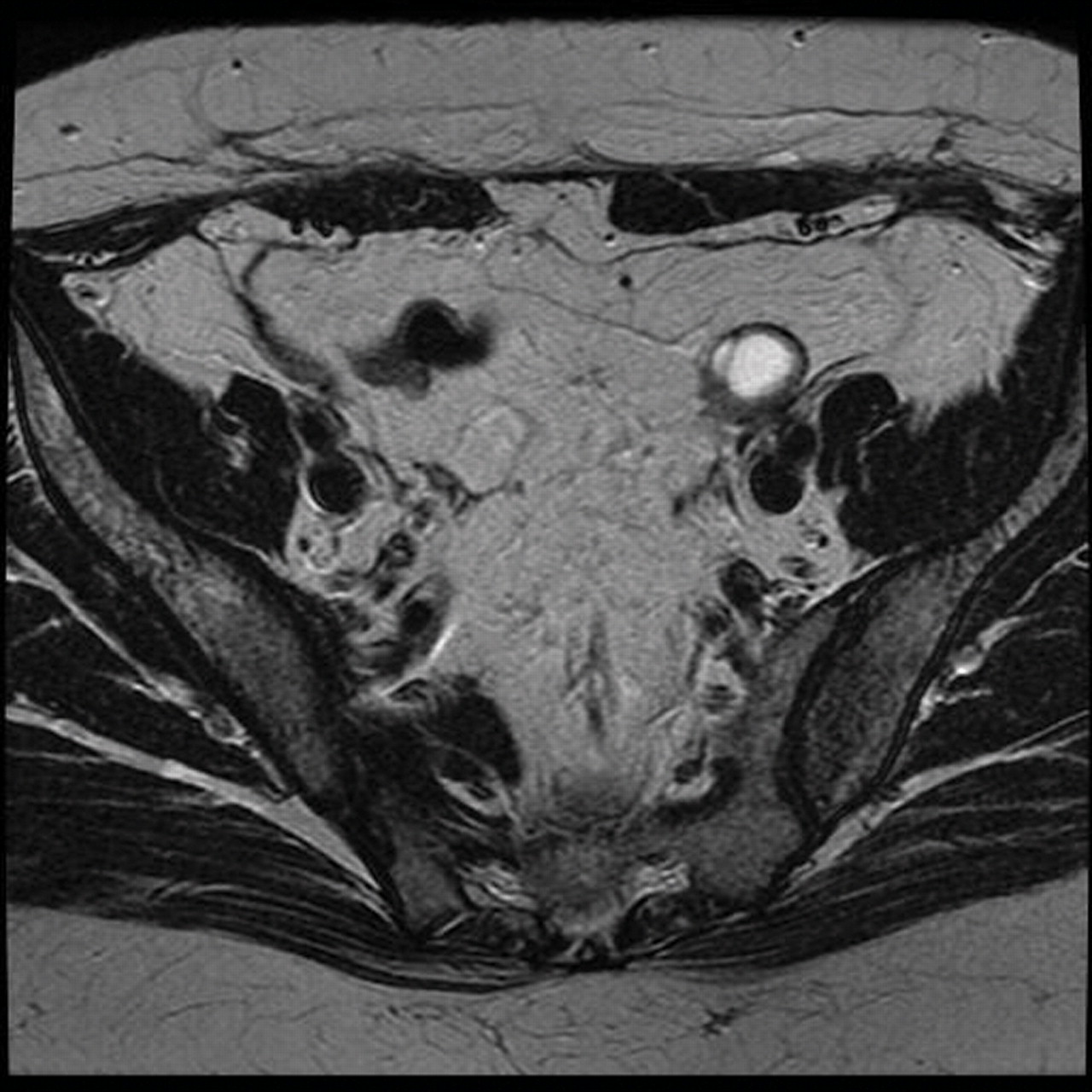
Figure 4: Magnetic resonance imaging scan showing no evidence of metastatic spread. The structure overlying the left iliac vessels represents a cystic ovary.
Fiscal responsibility and cost–benefit analysis are becoming important issues to consider with rising health care costs. Currently, most cervical cancer patients in developed countries are assessed with the use of magnetic resonance imaging. The review by Selman and colleagues5 has confirmed the inadequacy of magnetic resonance imaging in the detection of lymph node metastases; however, it remains a common imaging method for determining the extent of local disease and helping to guide the delivery of chemoradiotherapy. If positron emission tomography is more accurate in its determination of lymphatic spread, should all patients with cervical cancer undergo both magnetic resonance imaging and positron emission tomography? Given that modern positron emission tomography scanning involves a concomitant computed tomography scan, should patients undergo all 3 tests? The currently limited number of and access to positron emission tomography scanners presents important obstacles that provincial ministries of health need to address.
Studies to identify more accurate imaging methods are being performed. The Gynecologic Oncology Group and American College of Radiology Imaging Network are conducting a study comparing positron emission tomography using fludeoxyglucose F 18, computed tomography and magnetic resonance imaging using ferumoxtran-10 for the detection of lymph node metastases in advanced cervical cancer. If the last method is shown to be as accurate as positron emission tomography in detecting distant disease, it may provide a single modality than can be used in the complete assessment of cervical cancer, both locally and distally. Once the favoured imaging method is identified, the next step should be a randomized controled trial comparing it against standard management, with survival as the primary outcome. Given the current accuracy, availability and cost of imaging methods and number of patients, such a study may not be feasible.
The imaging and sentinel node biopsy studies examined in the review by Selman and colleages incorporate all stages of cervical cancer and define a positive result as the identification of any metastatic lymph node, irrespective of location. This represents a major weakness in the literature and inhibits meaningful evaluation of imaging methods. Despite this, Selman and colleagues have confirmed the role of sentinel node biopsy in the management of early cervical cancer. They have also shown that there is promise in the use of positron emission tomography and that we should continue to explore superior methods of identifying metastatic disease in cervical cancer. The issues identified in this commentary, including site of nodal disease, cost and resource availability, remain a challenge.
@ See related article page 855
Key points of the article
• The literature addressing imaging of lymph node metastases in patients with cervical cancer tends to encompass all stages of the disease.
• The applicability of any imaging method will require very high positive likelihood ratios in early cervical cancer and very high negative likelihood ratios in advanced cervical cancer to change clinical management.
• Sentinel node biopsy differs from magnetic resonance imaging, computed tomography and positron emission tomography in that it is a surgical procedure.
• Studies are ongoing to address the role of imaging in advanced cervical cancer with the intent of identifying the full extent of disease.
Footnotes
-
Contributors: Both of the authors contributed to the conception and design of the manuscript, drafted and revised the article, and approved the final version for publication.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

