


An 85-year-old woman presented with a 2-month history of generalized weakness, malaise, nausea, decreased appetite and 9-kg weight loss, as well as generalized pruritus of 2 weeks' duration. She described no abdominal pain, vomiting or abnormal bowel movements, though she had noted that her urine was somewhat darker than usual. She complained of having had mild, intermittent mid-back pain for a few months. The patient said that she had no history of blood transfusions, jaundice or hepatitis and was not using any medications, cigarettes or alcohol. On examination she was emaciated with mild jaundice, and had flat, brittle nails but no clubbing. The patient's abdomen was soft and scaphoid. A firm liver edge was palpable 3 cm below the right subcostal margin, as was a soft, nontender, tennis ball–sized lump in her right upper quadrant. The patient had no lymphadenopathy, no skin rash, no peripheral edema and no focal neurological findings.
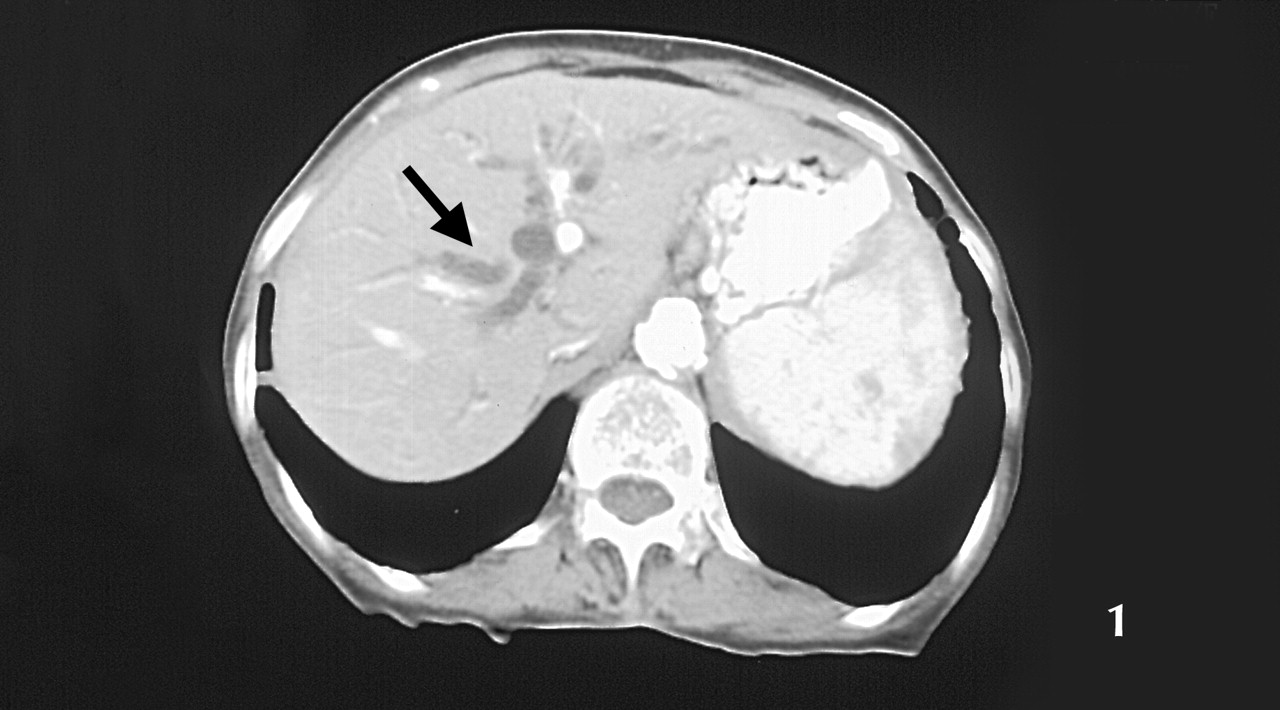
Although the patient's complete blood count, creatinine and electrolytes were normal, her erythrocyte sedimentation rate was slightly elevated at 39 mm/h, as were her serum bilirubin (32 μmol/L), AST (103 U/L), ALT (65 U/L), ALP (456 U/L) and GGT (367 U/L). An abdominal ultrasound scan showed dilated intrahepatic ducts and an enlarged gallbladder, but the patient's pancreas was not well visualized. A CT scan of the abdomen with contrast was performed: Fig. 1 shows a fatty liver and dilated intrahepatic ducts (black arrow); Fig. 2 shows the dilated pancreatic duct (white arrowhead), dilated common bile duct (white arrow) and enlarged gallbladder (black arrow); Fig. 3 shows an enlarged gallbladder (black arrow) and an inhomogeneous head of pancreas with a small soft-tissue density (white arrow). A chest radiograph showed numerous noncalcified nodules less than 1 cm in size in both lungs consistent with metastases. A clinical diagnosis of likely metastatic carcinoma of the head of pancreas or periampullary carcinoma was considered and endoscopic retrograde cholangiopancreatography was recommended to further establish the diagnosis, but the patient declined further investigations and died a month later. The family declined an autopsy.

Figure 3. Photo: Images courtesy of Dr. Malvinder S. Parmar

Figure 2. Photo: Images courtesy of Dr. Malvinder S. Parmar

{kind=link}
{kind=link}
{kind=link}
Figure 1. Photo: Images courtesy of Dr. Malvinder S. Parmar
In 1890, Ludwig Courvoisier described his observation that patients with painless jaundice and a palpable gallbladder often have a malignant obstruction of the common bile duct; this is known as “Courvoisier's law.”1 Painless jaundice and a palpable gallbladder are present in 50%–70% of patients with periampullary cancer or carcinoma of the head of pancreas.2
Gallbladder distension has been thought to occur because the distal malignant obstruction leads to chronically elevated intraductal pressures. This contrasts with obstructions caused by stones, which are associated with chronic cholecystitis and fibrosis of the gallbladder wall, which precludes distension. In addition, stones may cause only partial obstructions (related to a “ball-valve” action of the stone) leading to less consistent intraductal pressure elevations, and less gallbladder dilatation.3 The identification of some patients with stones, chronic cholecystitis and a Courvoisier's gallbladder has forced a realization that sometimes exceptions to Courvoisier's law do exist.
Nevertheless, this case underscores that for elderly patients presenting with jaundice and an enlarged, palpable gallbladder the possibility of a neoplastic process involving the head of pancreas or the ampulla of Vater should be strongly considered.
Malvinder S. Parmar Medical Director (Internal Medicine) Timmins and District Hospital Timmins, Ont.
In this issue
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Practice
Similar Articles
Collections

