


Abstract
BACKGROUND: Firearm injuries contribute to substantial morbidity and mortality. The immigrant paradox suggests that, despite being more socially disadvantaged, immigrants are less likely than nonimmigrants to have poor outcomes. We tested the association of immigrant characteristics with firearm injuries among children and youth.
METHODS: We conducted a population-based cohort study involving residents of Ontario aged 24 years and younger from 2008–2012 using health and administrative databases. We estimated rate ratios of unintentional and assault-related firearm injuries by immigrant status using Poisson regression models with Generalized Estimating Equations.
RESULTS: We included 15 866 954 nonimmigrant and 4 551 291 immigrant person-years in our analysis. Nonimmigrant males had 1032 unintentional (12.4 per 100 000, 95% confidence interval [CI] 11.7–13.2) and 304 assault-related (3.6 per 100 000, 95% CI 3.2–4.0) firearm injuries. Immigrant males had 148 unintentional (7.2 per 100 000, 95% CI 6.1–8.5) and 113 assault-related (5.5 per 100 000, 95% CI 4.5–6.6) firearm injuries. Compared with nonimmigrants, immigrants had a lower rate of unintentional firearm injury (adjusted rate ratio 0.5, 95% CI 0.4–0.6) but a similar rate of assault-related firearm injury. Among immigrants, refugees had a 43% higher risk of assault-related firearm injury compared with nonrefugees (adjusted rate ratio 1.4, 95% CI 1.0–2.0). Immigrants from Central America and Africa accounted for 68% of immigrants with assault-related firearm injuries.
INTERPRETATION: Compared with nonimmigrants, immigrant children and youth had a lower risk of unintentional firearm injury, although the risk of assault-related firearm injury was higher among refugees and immigrants from Central America and Africa. The results suggest that prevention strategies for firearm safety should target nonimmigrant youth as well as these newly identified high-risk immigrant populations.
Firearm injuries are a substantial cause of morbidity and mortality among children and youth.1,2 They have a high case-fatality rate3 and, among survivors, leave lasting repercussions with associated high direct medical and indirect costs.4 In Canada, an average of 1300 firearm-related deaths occur annually5 and many more firearm injuries lead to hospital admissions or emergency department visits.1,6,7 Several risk factors have been identified for sustaining a firearm injury or being a victim of a homicide. They include young age (< 5 yr) and late adolescence, male sex, low socioeconomic status, Indigenous ethnicity, black race, access to a firearm in the home and involvement in a gang.1,8–12 Canadian emergency physicians and pediatricians have recognized the need to identify at-risk populations to enable targeted strategies to prevent violent injuries.6,9 Such strategies are essential to counter the rising trend of violent crimes involving handguns in major Canadian cities12 and to lessen the burden of preventable unintentional firearm injuries.
One potential at-risk group includes the growing population of immigrant children and youth in Canada. Immigrants now make up 19% of the Canadian population.13 Although studies have reported lower rates of unintentional injury among immigrants than among Canadian-born children and youth,14,15 there was cause-specific variability and no population-based data on assaults were included. The immigrant paradox16 — a theory that, despite facing social disadvantage, new immigrants have better health outcomes than native-born people — has not been consistently observed among children17 nor well studied among victims of violent crime or unintentional firearm injuries. It is unknown whether immigration itself or immigration-related factors such as time since migration, region of origin and refugee status are related to firearm injury. Immigrants may bring their home country’s normative behaviours with them, including perceived need for firearm ownership.18 Firearm ownership varies across the globe, with rates as high as 112 firearms per 100 people in the United States, in contrast to 0.6 firearms per 100 in Japan2 and 26 per 100 in Canada.5 Global cultural norms for use of firearms for self-protection and involvement with gangs also vary. Moreover, circumstances that lead to migration, settlement supports and integration may affect the risk of firearm injuries.
As Canada embraces more immigrants, in particular from areas with civil unrest and economic hardship19 in the context of an increasing spate of firearm injuries,5,20 delineation of firearm risk among immigrants is important. We conducted a study to describe the epidemiology of victims of unintentional and assault-related firearm injuries among immigrant children and youth in Ontario and to test the association of immigration characteristics with firearm injuries.
Methods
We conducted a population-based cohort study using health and other administrative databases available at the Institute for Clinical Evaluative Sciences (ICES).
Data sources
Ontario has a single-payer universal Ontario Health Insurance Plan (OHIP) through which most hospital and physician services are insured. Unique OHIP identification numbers were encoded and linked to data from several health and administrative databases. The Registered Persons Database, Ontario’s health care registry, contains sociodemographic information, including age, sex and postal code, of all OHIP-eligible residents. The Canadian Institute for Health Information’s Discharge Abstract Database and National Ambulatory Care Reporting System collect data on hospital admissions and emergency department visits, respectively. The Ontario Registrar General — Death Files includes all deaths by cause. The Rurality Index of Ontario was used to determine rurality.21 Statistics Canada’s Postal Code Conversion File was used to determine neighbourhood income quintiles at the dissemination area level using Canadian census data (2006). The 2006 census, used also for population denominators, was chosen because the 2011 census was completed voluntarily and may introduce bias. Data from the most recent census (2016) are not yet available.
Immigration information was obtained from Immigration, Refugees and Citizenship Canada’s Permanent Resident Database. Permanent residents (immigrants granted permission to live and work in Canada without limitations on their stay) are eligible for provincially insured health care services, typically within 3 months after arrival. The available portion of this database includes data for all permanent residents to Canada landing in Ontario from 1985 to 2012, including those who eventually become citizens, but not including undocumented or temporary residents (e.g., foreign students). Probabilistic linkage to the Registered Persons Database identifies about 86% of permanent resident immigrants, and data quality and linkage details have been published elsewhere.22,23 The MOMBABY Database at ICES links inpatient admission records from the Discharge Abstract Database for mothers and their newborns delivered in Ontario hospitals.22 This database was used to identify newborns born in Canada to immigrant mothers.
Study population
We included all children and youth aged 24 years and younger living in Ontario from Jan. 1, 2008, to Dec. 31, 2012, who had a valid OHIP number. Individuals with a missing or invalid OHIP number or non-Ontario residents were excluded. Within the study period, we created 5 annual cohorts and assigned sociodemographic data annually with prespecified cut points based on data available as of Dec. 31 of the cohort year.
Outcome measures
The primary outcome measures were unintentional and assault-related firearm injuries. Injuries were defined in terms of emergency department visits, hospital admissions, and in- and out-of-hospital deaths using International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Clinical Modification (ICD-10-CM) codes for external causes of injury (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160850/-/DC1).24 Firearm injuries identified with the ICD-9-CM codes were validated in a study that used state-level administrative data in Washington (sensitivity 92% and positive predictive value 94%).25 Firearm injury intent from computerized discharge records and expert chart abstraction has shown 83% agreement.25 Intent is determined from internationally agreed upon codes used by the World Health Organization.26 We included multiple injury events for the same patient if the injury did not result from the same episode.
Predictor
The main predictor was immigrant status, defined as any child or youth with permanent residency status or born to a mother with permanent residency status, landing in Canada after Jan. 1, 1985. Children born to immigrant mothers before 1985, when immigration data became available, were categorized as nonimmigrants. Children of immigrant mothers were included because risk of injury is associated with maternal immigrant status,27 and maternal immigrant status may reflect a child or youth’s exposure to firearms and firearm-related behaviours in the home environment.
Covariates
Male sex, older adolescence and low socioeconomic status have been associated with firearm injury or homicide risk.1,9,28 Therefore, we included age, sex and neighbourhood income quintile as covariates, as well as rurality of residence. Immigration characteristics used included visa class (refugee v. nonrefugee immigrant), region of origin (based on country of birth using modified Immigration, Refugees and Citizenship Canada world regions (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160850/-/DC1)13 and time since migration to Canada (recent: 0–5 yr, intermediate: 6–10 yr, long term: > 10 yr).
Statistical analysis
We calculated the total number of firearm injuries during the 5 study years and age-sex standardized rates per 100 000 population using 2006 census estimates. We followed the strict privacy guidelines set out by ICES for use of health administrative data for health research without individual consent. Institutional policy requires suppression of cell sizes of less than 6 to ensure nonidentification. We calculated rate ratios with 95% confidence intervals (CIs) of unintentional and assault-related firearm injuries by immigrant status using multivariable Poisson regression models with Generalized Estimating Equations to account for clustering of multiple injury events within victims. Separate regression models were built for each immigration characteristic. All models were adjusted for age, sex, neighbourhood income quintile and rurality. Results are presented as the sum of the 5 annual cohorts, age-and sex-standardized rates, and rate ratios.
We conducted sensitivity analyses in which we excluded children born in Ontario to immigrant mothers and children living in rural areas.
We performed all statistical modelling using SAS Enterprise Guide, version 6.1 (SAS Institute).
Ethics approval
Research ethics board approval was obtained from Sunnybrook Health Sciences Centre and The Hospital for Children, Toronto, Ontario.
Results
We included almost 16 million nonimmigrant and 4.5 million immigrant person-years in our analyses (Table 1). Immigrants were younger and had larger proportions living in lower income neighbourhoods. Among the immigrants, most (98.8%) lived in urban areas, 15.6% were refugees, and 24.2% had recently immigrated. Almost half (49.0%) were from South and East Asia.
Characteristics of immigrant and nonimmigrant children and youth in Ontario, 2008–2012
In the 5-year study period, male nonimmigrants had 1032 unintentional (12.4 per 100 000, 95% CI 11.7–13.2) and 304 assault-related (3.6 injuries per 100 000, 95% CI 3.2–4.0) firearm injuries. In contrast, male immigrants had 148 unintentional (7.2 per 100 000, 95% CI 6.1–8.5) and 113 assault-related (5.5 per 100 000, 95% CI 4.5–6.6) firearm injuries. Female nonimmigrants had 137 unintentional (1.7 per 100 000, 95% CI 1.4–2.0) and 31 assault-related (0.4 per 100 000, 95% CI 0.3–0.5) firearm injuries. Female immigrants had 12 unintentional and less than 6 assault-related firearm injuries (Table 2). Most (68%) of the assault-related injuries and a large proportion (43%) of unintentional firearm injuries were in immigrants from Africa and Central America (Table 2).
Frequency and age- and sex-standardized rates of firearm injury by immigration status and sociodemographic characteristics, 2008–2012
The risk of unintentional firearm injury was lower among immigrant children and youth (adjusted rate ratio 0.5, 95% CI 0.4–0.6), whereas the risk of assault-related firearm injury was not associated with immigrant status (Table 3). The results of the sensitivity analysis excluding children born in Canada to immigrant mothers and children living in rural areas did not change the direction of these associations. Predictors of firearm injuries included older age (15–24 yr), male sex and low income quintile. The strength of these associations was greater with assault-related than with unintentional firearm injuries, as well as within the immigrant group compared with the nonimmigrant group in the stratified models. Rural residence was predictive of unintentional firearm injury, and urban residence was positively associated with risk of assault from a firearm.
Adjusted rate ratios of unintentional and assault-related firearm injuries by immigrant status and sociodemographic characteristics
Figure 1 shows the adjusted rate ratios for firearm injury by immigration characteristics. Compared with nonimmigrants, refugees had a 43% higher risk of an assault-related firearm injury (adjusted rate ratio 1.4, 95% CI 1.0–2.0) but they did not differ in risk of unintentional firearm injury. Nonrefugee immigrants had a 55% lower risk of unintentional firearm injury compared with nonimmigrants. With increasing duration of residence in Canada, risk of both unintentional and assault-related firearm injuries increased. The risk of unintentional firearm injury was lower among immigrants than among nonimmigrants regardless of duration of residence. The risk of assault-related firearm injury was 1.3 times higher among long-term immigrants (in Canada longer than 10 yr) compared with nonimmigrants (adjusted rate ratio 1.35, 95% CI 1.10–1.66), and it was higher among immigrants from Africa and Central America (Africa: adjusted rate ratio 2.8, 95% CI 2.0–4.1; Central America: adjusted rate ratio 4.1, 95% CI 3.0–5.6).
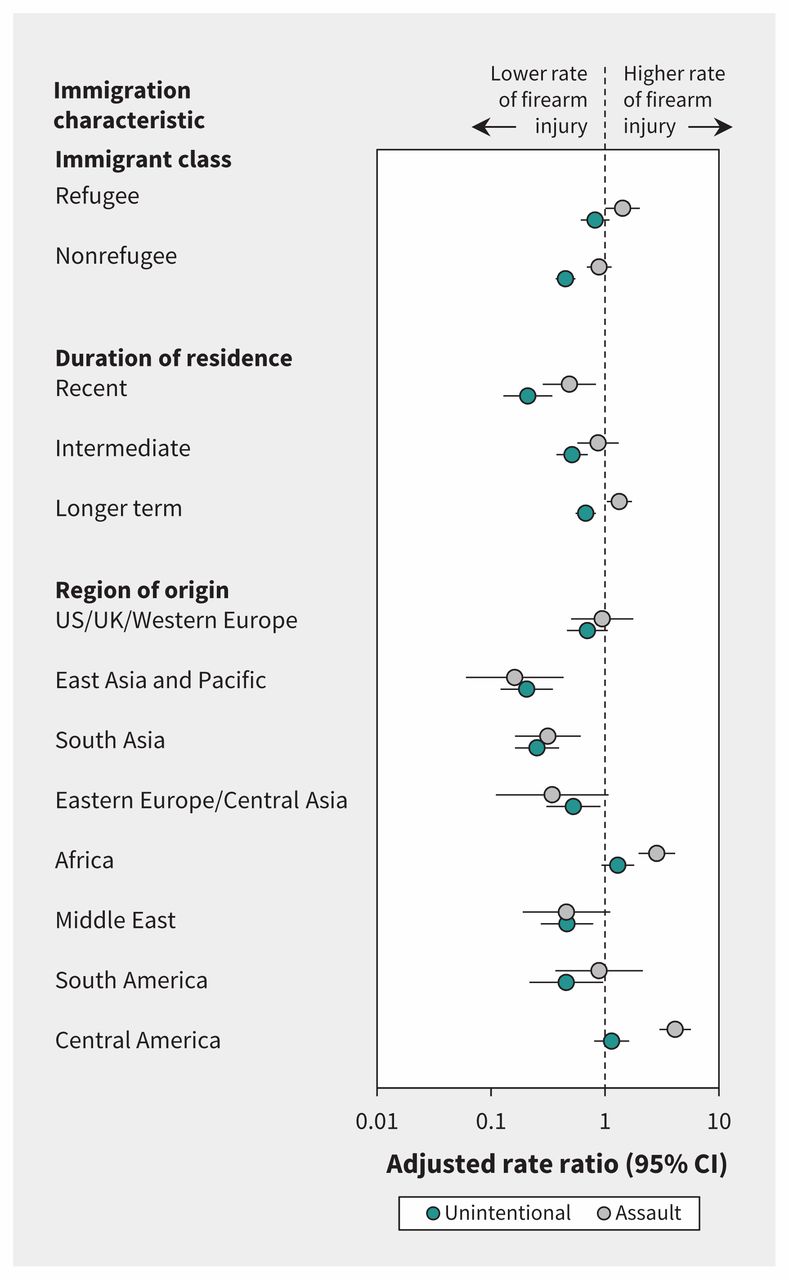
Adjusted rate ratios for firearm injuries (unintentional and assault-related) by immigration characteristics. Each immigration characteristic was modelled separately and adjusted for age, sex, income quintile and rurality. Values greater than 1 indicate a higher rate of firearm injury compared with the reference group (nonimmigrants). CI = confidence interval.
Interpretation
Results from this large, population-based study suggest that immigration is protective and mitigates the risk of unintentional firearm injuries but increases the risk of a firearm assault in certain subgroups. Among immigrants, refugees were at particularly high risk of firearm injuries regardless of intent, as were immigrants with a longer duration of residence in Canada. There was wide variation in the risk of firearm injury by region of origin, with considerably high rates among immigrants from Africa and Central America.
Canada has relatively few firearm injuries, although many countries, predominantly in South and East Asia, have even lower rates than observed in the current study.29 Nonetheless, rates of unintentional firearm injury among nonimmigrant Canadian children and youth are concerning and warrant further attention. The predictors of firearm injury in our study were comparable to those in other studies that reported males, low socioeconomic status, and late adolescence and young adulthood were associated with firearm injury.1,9,28 Low rates of unintentional firearm injury among immigrants, despite a relatively large proportion living in low-income neighbourhoods, supports the immigrant paradox. Few studies have evaluated the association between immigration and risk of firearm injuries. A Swedish population-based study reported that foreign-born adults did not differ from native-born Swedes in the odds of nonfatal unintentional firearm injuries but were at higher risk of being a victim of attempted murder with a firearm.30 Similarly, homicides were 40% lower among Italians than among immigrant males in Italy, although firearm-specific rates were not reported.31 In California, foreign-born people were over-represented in homicides of people 15 to 34 years old.32 Immigration-specific factors such as visa class and duration of residence and their relation to firearm injuries were not explored in these studies.
Possible contributing factors to the increased risk of assault-related firearm injuries in immigrant subgroups may relate to higher rates of poverty, lack of access to resources, and more bullying and peer aggression among first-generation immigrant adolescents.33 The finding that, overall, immigration was not associated with assault-related firearm injuries is consistent with the finding of Chavez and colleagues,34 who reported no association of neighbourhood-level immigration with changes in homicide rates. In our study, the observed variation in firearm injury by region of origin may have been related to higher participation in Canadian gangs by Indo-Asian, Caribbean and African immigrants than by those from other regions, and it highlights the need to ensure a healthy transition to Canada for these particular at-risk groups.35
Household gun ownership increases the risk of unintentional firearm injuries.36 The lower rates of unintentional firearm injuries observed among nonrefugee immigrants may relate to low rates of firearm ownership by immigrants, residence in urban areas and selection policies for immigrants to Canada who are highly educated. 13,37 The increasing risk of firearm injury with longer time spent in Canada highlights one area for possible public health education and consumer regulation around gun safety and storage. It also brings to light a need to improve longer-term settlement and integration services for immigrants to maintain healthy behaviours with increasing duration of residence in Canada.
Although the observed rates of firearm injuries in our study were substantially lower than those in many other countries,1,2 they nonetheless represent injuries that are often catastrophic and entirely preventable. A number of interventions have been associated with reductions in firearm injury rates, including firearm legislation restricting gun ownership, registration and access,38,39 and recommendations around safe firearm storage.40 For reducing assault-related firearm injuries specifically, neighbourhood-level community engagement strategies,41 conflict resolution programs,42 emergency department and hospital interventions with brief motivational interviewing and cognitive skills training,43 and community-based programs to develop social skills44 have shown promising results. Although such interventions have contributed to reductions in firearm injuries, there is room for continued improvement, especially targeted toward reducing the number of unintentional firearm injuries among nonimmigrant children and youth and assault-related firearm injuries in subgroups of immigrant youth.
Strengths and limitations
Major strengths of this study include the large sampling frame, with almost complete provincial coverage of children and youth in Ontario, and detailed immigration data which allowed for contextualization of contributing immigration factors. We reported on all firearm injuries, including those involving children and youth presenting to the emergency department and admitted to hospital, rather than more commonly reported mortality data, which allowed better ascertainment of the burden of this public health problem.
There are some important limitations. The immigration data available to us did not include information on undocumented or temporary immigrants. Paternal immigration, parental education level or employment status, and secondary migration data were not available and may be associated with risk of firearm injury. In some instances, small numbers made more detailed risk stratification impossible.
Conclusion
We counted almost 1800 firearm injuries among children and youth in Ontario over a 5-year period, which represents almost 1 injury per day. Nonimmigrant youth had the highest rates of unintentional firearm injury. Immigrant children and youth were at lower risk of unintentional firearm injury overall, but the risk of assault-related firearm injury was higher among refugees and among immigrants from Africa and Central America compared with nonimmigrants. Understanding why the immigrant paradox was not observed in these subgroups needs further study and intervention. Prevention strategies for firearm safety should target nonimmigrant youth as well as these newly identified high-risk immigrant populations.
Footnotes
CMAJ Podcasts: author interview at https://soundcloud.com/cmajpodcasts/160850-res
Visual abstract available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160850/-/DC2
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Natasha Saunders, Alison Macpherson and Astrid Guttmann conceptualized and designed the study. Natasha Saunders, Hannah Lee, Alison Macpherson and Astrid Guttmann interpreted the results. Jun Guan analyzed the data. Natasha Saunders and Hannah Lee drafted the initial manuscript. All of the authors revised the manuscript for important intellectual content, approved the final version to be published and agreed to act as guarantors of the work.
Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI) and Immigration, Refugees and Citizenship Canada (IRCC). The analyses, conclusions, opinions and statements expressed in this paper are those of the authors and not necessarily those of CIHI and IRCC.
Funding: Astrid Guttmann and Alison Macpherson are funded through Applied Chairs in Child Health Services and Policy Research from the Canadian Institutes for Health Research. All data analyses were funded through Astrid Guttmann’s research chair.
Disclaimers: This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
- Accepted December 5, 2016.
References
In this issue

Article tools






{kind=link}
Jump to section
Related Articles
Cited By...
- Death and long-term disability after gun injury: a cohort analysis
- Mortality in a cohort of 3.1 million children, adolescents and young adults
- The authors respond to: "Questions on analysis of firearm injuries study"
- Questions on analysis of firearm injuries study
- More on firearm injuries among children and youth
More in this TOC Section
Similar Articles


Podcast