


Abstract
BACKGROUND: Sedentary behaviours are associated with adverse health outcomes in middle-aged and older adults, even among those who exercise. We examined whether the degree of frailty affects the association between sedentary behaviours and higher risk of mortality.
METHODS: In this prospective cohort study, we used data from 3141 community-dwelling adults 50 years of age or older from the 2003/04 and 2005/06 cohorts of the US National Health and Nutrition Examination Survey. Time engaged in sedentary behaviours was measured using uniaxial accelerometers, and frailty was based on a 46-item frailty index. Mortality data were linked up to 2011. We used Cox proportional hazard models to estimate the hazard ratio (HR) of sedentary behaviour.
RESULTS: We found that for people with low levels of frailty (frailty index score ≤ 0.1), sedentary time was not predictive of mortality, regardless of physical activity level (adjusted HR 0.90, 95% confidence interval [CI] 0.70–1.15). Among people who were vulnerable (0.1 < frailty index score ≤ 0.2) or frail (frailty index score > 0.2), sedentary time was associated with higher mortality only among those who were physically inactive (not meeting the criterion for moderate physical activity) (HR 1.16, 95% CI 1.02–1.33 for the group defined by 0.1 < frailty index score ≤ 0.2; HR 1.27, 95% CI 1.11–1.46 for the group defined by 0.2 < frailty index score ≤ 0.3; HR 1.34, 95% CI 1.19–1.50 for frailty index score > 0.3).
INTERPRETATION: The effect of sedentary behaviours on mortality varied by level of frailty. Adults with the highest frailty level experienced the greatest adverse impact. Low frailty levels (frailty index score ≤ 0.1) seemed to eliminate the increased risk of mortality associated with prolonged sitting, even among people who did not meet recommended physical activity guidelines.
Sedentary behaviours are increasingly recognized as conferring health risks, independent of physical activity. The health benefits of physical activity are well established, and meeting minimum guidelines for physical activity is associated with reduced risk of many chronic conditions, functional decline, development of psychologic disorders and mortality.1–9 However, even among people who engage in periods of purposeful exercise, sedentary behaviours can increase the risk of adverse outcomes, such as metabolic risk factors, functional limitations, and all-cause and cardiovascular disease mortality.10–16 Even so, a recent meta-analysis showed that engaging in moderate physical activity, such as exercise, for at least 1 hour/day could eliminate the detrimental effects of prolonged sitting.17
Although most of the research on sedentary behaviours has focused on children and younger adults, middle-aged and older adults are the most sedentary group. A study using data from the Canadian Health Measures Survey showed that Canadians over the age of 40 are highly sedentary, spending about 9.5–10 of their waking hours in sedentary behaviours (age 40–59 yr, 9.5 h for men and 9.8 h for women; age 60–79 yr, 9.9 h for men, 10 h for women).18 Only 14.6% of the Canadian population aged 40–59 years and 13.1% of those aged 60–79 years met the recommended 2.5 hours/week of moderate-to-vigorous physical activity.18 Another study using data from the US National Health and Nutrition Examination Survey (NHANES) showed that participants over the age of 50 years spent on average 8.5 of their waking hours in sedentary behaviours.19 Only 7.1% of the population met the recommended 2.5 hours/week of moderate-to-vigorous physical activity.19
Reducing sedentary behaviours could improve health outcomes in middle-aged and older adults. Replacing 30 minutes of sedentary time with an equal amount of light activity or moderate-to-vigorous activity was associated with 14% and 50% reductions in risk of mortality, respectively.20,21 Even so, studies have shown a strong relation between sedentary behaviours and frailty, independent of moderate-to-vigorous activity.22,23 In addition, levels of sedentary behaviours closely corresponded to levels of frailty, with nonfrail individuals being sedentary for an average of 8.2 hours/day, whereas most frail individuals were sedentary for 9.6 hours/day.19 Yet no studies have examined whether the effect of sedentary behaviours on adverse health outcomes differs across levels of frailty. Such an understanding is vital if we are to systematically address sedentary behaviour among older people as a risk factor for adverse outcomes. We undertook this study to examine whether frailty level affects the association of sedentary behaviours with higher risk of mortality.
Methods
Sample
We used data from the 2003/04 and 2005/06 cohorts of the NHANES. The NHANES is a series of cross-sectional surveys of a community-based sample. The NHANES investigators selected participants using a complex algorithm to ensure that the sample was nationally representative of the United States.24 For the current study, we included only participants 50 years of age or older who had a valid frailty index score, as well as accelerometer and mortality data. The NHANES investigators linked the NHANES data with death certificate data from the National Death Index to estimate mortality status.25 We calculated person-years of follow-up from the examination date until the date of death or censoring on Dec. 31, 2011.
Frailty index
Using the deficit accumulation approach, we used a 46-item frailty index that was constructed and validated in the NHANES population.19,26 We have previously published a complete list of deficits and coding.27 We calculated individual frailty index scores by dividing the number of deficits present in an individual by the total number of deficits considered; for example, an individual with 23 out of a possible 46 deficits would have a score of 0.5 (23/46). As noted above, we excluded from the analysis individuals with missing frailty data, defined as those with data missing on more than 20% of deficits. We categorized frailty index scores into 0.1-point increments to create 4 groups (≤ 0.1, 0.1 < frailty index score ≤ 0.2, 0.2 < frailty index score ≤ 0.3, and > 0.3). These cut points are widely used in the literature.28,29 In our previous study using NHANES data,19 the first 2 categories were very similar but the third category was 0.2–0.45 and the fourth category was greater than 0.45. Although this categorization isolated people with severe frailty into 1 category (> 0.45), the group was very small (n = 122), with only 3 people meeting the guidelines of 2.5 hours/week of moderate-to-vigorous physical activity and only 2 reporting vigorous activity.19 Therefore, for the current study, we used 0.3 as the cut point for the fourth group, which identified people with moderate-to-severe frailty.
Physical activity and measures of sedentary behaviour
Each participant wore a uniaxial AM-7164 accelerometer (Acti-Graph, LLC) on an elastic waist belt for a 7-day period. NHANES investigators instructed participants to wear the accelerometer during all waking hours and to remove it during bathing or swimming activities. We excluded all data marked as nonreliable or not in calibration; only the data of those who wore the accelerometer for a minimum of 10 hours on 4 separate days were included in the analysis.18,30 Using validated NHANES cut points,19,30 we defined sedentary behaviour as 0–100 counts/minute and moderate-tovigorous physical activity as greater than 2020 counts/minute. We analyzed sedentary behaviour as both a continuous and a categorical variable, where low sedentary behaviour was less than 7 hours/day, intermediate sedentary behaviour was 7 to 10 hours/day, and high sedentary behaviour was more than 10 hours/day. We also dichotomized physical activity as meeting or not meeting the recommendations of both the Canadian Society for Exercise Physiology4 and the American College of Sports Medicine31,32 (2.5 h/wk of moderate-to-vigorous physical activity). Participants self-reported vigorous activity by stating whether they had done any activity that caused heavy sweating or large increases in breathing or heart rate for a period of at least 10 minutes over the past 30 days.
Statistical analysis
We conducted all statistical analyses using SPSS software, version 21 (IBM). We calculated mortality rates for all participants after stratifying by frailty index level, by sedentary time and by accelerometer-measured and self-reported physical activity. We used the Pearson χ2 test to examine associations between mortality and frailty group, sedentary time and physical activity. We used Cox proportional hazard models to estimate the hazard ratio of sedentary behaviour. To control for the fact that participants entered the study at different ages, we used residual proportional hazards regression.33 In the first stage, time-varying covariables (i.e., frailty, moderate-to-vigorous physical activity and self-reported exercise) were individually regressed on age, and the residuals from each of these regressions were saved. In the second stage, we ran Cox regressions with age and the saved residuals replacing their corresponding covariables. Because we were interested in adults 50 years of age or older, we used age as the time scale, with age 50 years as the time origin. The basic model examined the risk of death associated with sedentary behaviour controlling for significant covariables; additional models adjusted for both objectively and subjectively measured physical activity. We then stratified the analyses by objectively measured physical activity (≥ 2.5 h/wk or < 2.5 h/wk of moderate-to-vigorous physical activity) and self-reported vigorous physical activity in the last 30 days (yes or no) and then further stratified by frailty index level. We stratified Kaplan–Meier survival curves, using time from assessment as the time scale, by both frailty index group and physical activity. We used statistical weights for demographic characteristics and mortality rates to ensure that the sample was representative of the US population.
We included in the regression models the following covariables, which have been shown to be related to sedentary time and frailty: age (yr), sex (male, female), education (less than high school, high school, some college or associate degree, college graduate or more), race/ethnicity (Mexican American or other Hispanic, non-Hispanic white, non-Hispanic black, other), marital status (married, widowed, divorced or separated, never married), smoking status (never, past, current), body mass index (< 18.5, 18.5–24.9, 25–29.9, ≥ 30), employment status (working full-time, not working full-time), accelerometer wear time (h) and study cohort (2003/04, 2005/06). We considered annual household income and alcohol use as potential covariables but did not include them because of missing data.
Ethics approval
The NHANES survey protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention. All patients provided written informed consent.
Results
Of the 20 470 participants from the 2003/04 and 2005/06 NHANES cohorts, 4874 individuals were aged 50 years or older. After exclusion of participants with missing accelerometer data (n = 1421), frailty index data (n = 307) and mortality data (n = 5), the final sample size was 3141 (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.161034/-/DC1). Those excluded were slightly older than those included in the analysis (mean age ± standard deviation 65.9 ± 12.0 v. 63.3 ± 10.1 yr), with slightly higher levels of disability based on activities of daily living (for women, 54.3% of those excluded v. 53.7% of those included had disability; for men, 19.8% of those excluded v. 17.0% of those included had disability). On average, accelerometer data were available for 6.24 ± 0.94 days and 14.2 ± 1.7 daily hours for each participant. The mean duration of follow-up from the date of baseline assessment until the date of death or censoring was 6.5 ± 1.6 years.
All of the characteristics of this sample except smoking differed by frailty index (Table 1). The weighted mortality rate was 12.0% (550/3141) or 18.7 deaths per 1000 person-years (Table 2). Mortality rate increased with higher frailty index levels, both in the overall sample (p < 0.001) and when stratified by sedentary time or physical activity (p < 0.001).
Characteristics of participants by frailty level
Mortality rate stratified by frailty level, sedentary time and physical activity
Cox regression models showed significant interaction between frailty and sedentary behaviour, even when objectively measured and self-reported physical activity were added to the model (Table 3). When the analysis was stratified by physical activity, we found that for those who met the moderate-to-vigorous physical activity requirements and for those who reported vigorous physical activity, there was no significant interaction between frailty and sedentary behaviour, and sedentary time was not associated with mortality (Table 3). When the analysis was stratified by frailty level, we found that sedentary behaviour remained associated with mortality in the 3 highest frailty index groups in a fully adjusted model (frailty index score > 0.1) but not in the group with low frailty (frailty index score ≤ 0.1) (Table 4). There was no association between sedentary behaviour and mortality among those who met the requirements for moderate-to-vigorous physical activity or self-reported vigorous physical activity in the last month (Table 4).
Relation between sedentary time and time to death, stratified by physical activity
Relation between sedentary time and time to death, stratified by frailty index
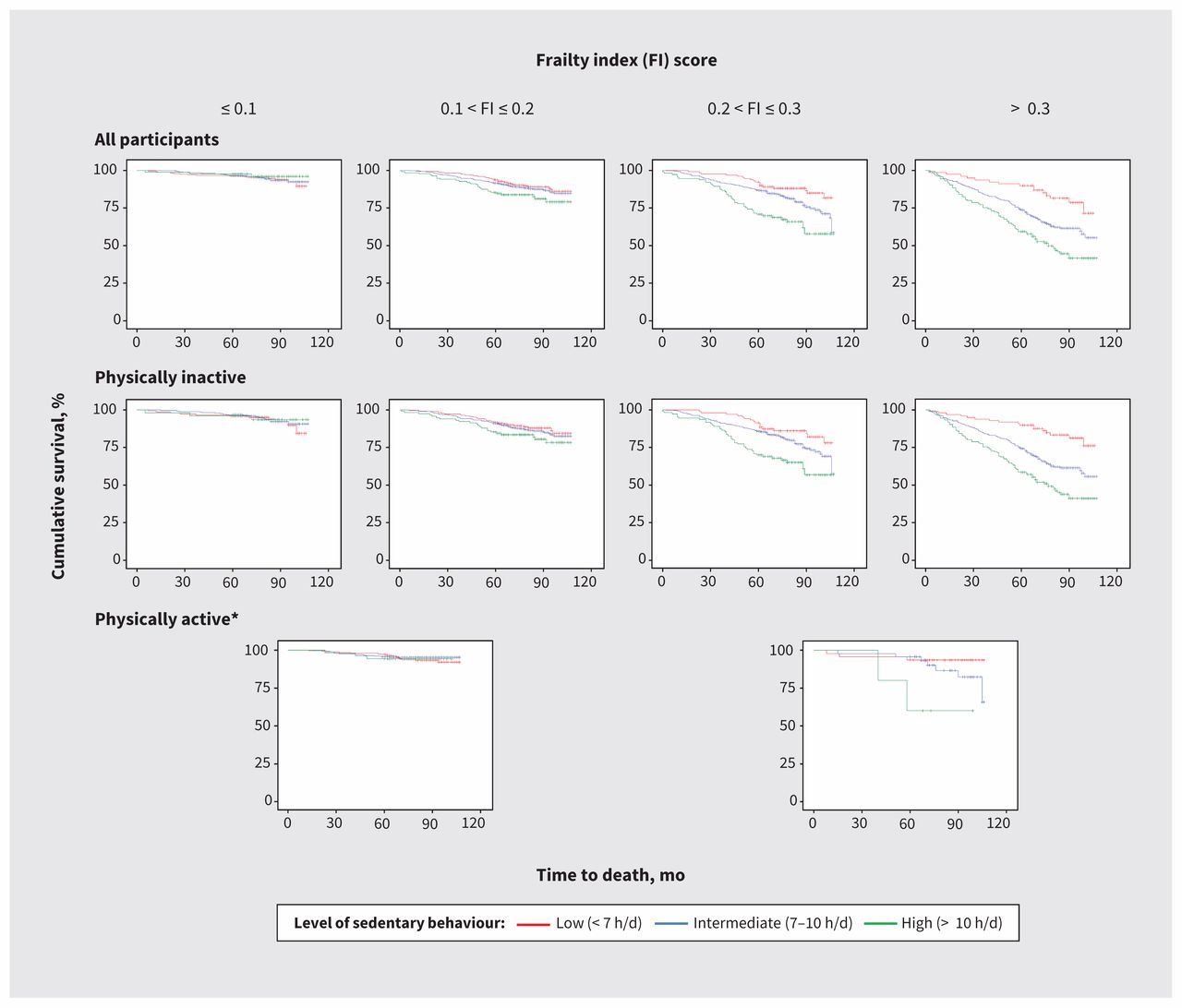
Kaplan–Meier curves showed a significant separation among low, intermediate and high levels of sedentary behaviour. This pattern held true for the 3 highest frailty index groups of the overall sample (p < 0.05) and for those who were physically inactive by objective measurement (p < 0.05; Figure 1) or did not report vigorous physical activity in the past month (p < 0.05).

Kaplan–Meier Curves stratified by frailty index score and whether participants were physically active or inactive (as determined by objective measurement). *For the physically active participants, the groups with frailty index score ≤ 0.1 and 0.1 < frailty index score ≤ 0.2 were merged, as were the groups with 0.2 < frailty index score ≤ 0.3 and frailty index score > 0.3, because of small sample sizes.
Interpretation
This large, nationally representative study of the US population showed the degree to which the accumulation of age-related health deficits affects the association between sedentary behaviours and higher risk of mortality. We found that for people who had low levels of frailty (frailty index score ≤ 0.1), sedentary time was not predictive of mortality, regardless of physical activity level. For those who were vulnerable (0.1 < frailty index score ≤ 0.2) or frail (frailty index score > 0.2), sedentary time was associated with higher mortality only among those who were physically inactive (not meeting the requirement for moderate physical activity or not reporting participation in vigorous activity). Thus, among people who are inactive and vulnerable or frail, sitting time increases mortality risk, but among those who are nonfrail or active, sitting time does not affect the risk of mortality.
NHANES is a cross-sectional survey, and mortality data were provided through linkage to death certificate data. Although this approach increases the accuracy of the data, it did not allow us to examine whether changes in sitting time affect the risk of death. NHANES collected accelerometer data only from the 2003/04 and 2005/06 cohorts; therefore, more recent data for objectively measured physical activity levels were not available to us through this survey. We expect that if we had been able to use more recent data in our study, we could have shown a slightly higher level of physical activity among participants; however, we do not expect that the relation between sedentary behaviours and mortality would have been different. A previous study using the NHANES self-reported physical activity data showed that more participants in the 2011/12 cycle than the 2007/08 cycle met the physical activity guidelines (21.7% v. 27.2%); however, the proportion of people reporting no leisure time physical activity remained stable between the 2 cohorts.34
Multiple studies have shown that sedentary behaviours are associated with mortality in middle-aged and older adults.20,21,35,36 Wijndaele and colleagues35 showed that time spent watching television was associated with all-cause mortality in a population-based cohort (the European Prospective Investigation into Cancer and Nutrition study) of about 13 000 people (62 ± 9 yr), even after stratification by age, sex, education, body mass index and energy expenditure for total physical activity. Similarly, Matthews and colleagues36 showed that time spent watching television was associated with all-cause mortality in 240 819 adults (50–71 yr) from the Diet and Health Study of the National Institutes of Health and the American Association of Retired Persons, even after stratification by age, sex, education, race, body mass index, smoking, chronic conditions and diet quality. Fishman and colleagues21 showed that replacing objectively measured sedentary time with light activity was associated with a reduction in mortality risk in NHANES, and the sex-stratified findings were similar to the findings for men and women combined. The current study showed that stratification by frailty level had an impact on the effect of sedentary behaviours on mortality. Differences from these previous studies may be related to levels of frailty representing the overall health state of an individual and the frailty index being a more sensitive measure for change in health than other measures. Similar to our study, a recent meta-analysis including data from more than 1 million individuals showed that among people who were physically active (> 35.5 metabolic equivalent of task-hours per week or about 60–75 min/d), sedentary time was not predictive of all-cause mortality.17
Limitations
Our study had some limitations, and our findings should be interpreted with caution. As is typical for studies using physical activity monitors, almost one-third of participants in our study were missing accelerometer data, and these participants seemed to have higher levels of frailty. Thus, our sample size was substantially reduced, especially among the group with the highest level of frailty, which made it necessary to merge frailty groups for some analyses and prevented us from isolating those with severe frailty (frailty index score > 0.45) into 1 category. Future studies will need to examine the effect of sedentary behaviours on people with higher levels of frailty using other data sets. Furthermore, we could not include income and alcohol as covariables because of missing data. Another limitation relates to the accelerometer cut points used in this study to assess the time spent in sedentary behaviours and moderate-to-vigorous physical activity; although widely used, these cut points are based on studies involving healthier older adults and we may therefore have overestimated sedentary time in the participants with higher frailty levels. Even so, accelerometers are reliable measures of sedentary behaviours, have been validated in older adults with and without impaired function37–42 and can also be used for people with cognitive problems who cannot complete questionnaires about their daily levels of physical activity.43,44 Finally, although the HRs per hour of sedentary behaviour were relatively high for most models, the lower limit of some confidence intervals was close to 1.00.
Conclusion
This study has shown that the effect of sedentary behaviours on mortality differs across levels of frailty among people who are physically inactive, with people who are most frail experiencing the greatest impact. For these individuals, it appears that all hours of the day have an effect on health, not just those spent in physical activity of moderate-to-vigorous intensity. Similar to the situation for tobacco control, where doctors do not emphasize the benefits of nonsmoking, but rather the harms of smoking, we should also emphasize the harms of sedentary behaviours rather than just the benefits of physical activity.5 This is an important public health message that should be part of a larger promotion of the importance of healthy lifestyle behaviours.45 The first Canadian 24-hour movement guideline for children and youth, released in June 2016, suggested that sitting for extended periods should be limited and that recreational screen time should not exceed 2 hours a day. Similar guidelines are needed for middle-aged and older adults.46 Future studies should also examine whether the degree of frailty affects the association of sedentary behaviours with other adverse outcomes, such as functional and cognitive decline, and whether interventions to reduce sitting time should be modified on the basis of frailty level of participants. A randomized clinical trial should examine whether reducing sedentary behaviours can prevent or delay frailty.
Footnotes
CMAJ Podcasts: author interview at https://soundcloud.com/cmajpodcasts/161034-res
Competing interests: Kenneth Rockwood is a founder and director of DGI Clinical Inc., attended a Roche advisory board meeting concerning outcome measurement for Alzheimer disease and has received speaker’s fees from Nutricia. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Olga Theou contributed to the conception and design of the study and to the analysis and interpretation of data. Joanna Blodgett contributed to the design and to acquisition, analysis and interpretation of data. Judith Godin contributed to the analysis and interpretation of data. Kenneth Rockwood contributed to the conception and design. All of the authors drafted the manuscript, revised it critically for important intellectual content, approved the version to be published and agreed to act as guarantors of the work.
Funding: Kenneth Rockwood receives funding from the Dalhousie Medical Research Foundation as Kathryn Allen Weldon Professor of Alzheimer Research.
- Accepted April 11, 2017.
References
In this issue

Article tools



{kind=link}
Jump to section
Related Articles
Cited By...
- How race and socioeconomic status moderate the association between moderate-to-vigorous physical activity and depressive symptoms: a cross-sectional study with compositional data
- A Digitally Enabled, Pharmacist service to detecT medicine harms in residential aged care (nursing home) (ADEPT): protocol for a feasibility study
- Moving beyond Sedentarism in CKD
- Frailty, inequality and resilience
More in this TOC Section
Similar Articles


Podcast