


Abstract
Background: Because of established links between entrenched poverty and risk of HIV infection, there have long been warnings that HIV/AIDS will disproportionately affect Aboriginal people in Canada. We compared HIV incidence rates among Aboriginal and non-Aboriginal injection drug users (IDUs) in Vancouver and studied factors associated with HIV seroconversion among Aboriginal participants.
Methods: This analysis was based on 941 participants (230 Aboriginal people) recruited between May 1996 and December 2000 who were seronegative at enrolment and had completed at least one follow-up visit. Incidence rates were calculated using the Kaplan–Meier method. The Cox proportional hazards regression model was used to identify independent predictors of time to HIV seroconversion among female and male Aboriginal IDUs.
Results: As of May 31, 2001, seroconversion had occurred in 112 (11.9%) of the participants, yielding a cumulative incidence of HIV infection at 42 months of 12.7% (95% confidence interval [CI] 10.3%–15.1%). The cumulative incidence at 42 months was significantly higher among the Aboriginal participants than among the non-Aboriginal participants (21.1% v. 10.7%, p < 0.001). This elevation in risk was present in both female and male Aboriginal IDUs. Among the female Aboriginal IDUs, frequent speedball (combined cocaine and heroin) injection (adjusted relative risk [RR] 3.1; 95% CI 1.4–7.1) and going on binges of injection drug use (adjusted RR 2.3; 95% CI 1.0–5.2) were found to be independent predictors of HIV seroconversion. Among the male Aboriginal IDUs, the independent predictors of seroconversion were frequent speedball injection (adjusted RR 2.9; 95% CI 1.0–8.5) and frequent cocaine injection (adjusted RR 2.5; 95% CI 1.0–6.5).
Interpretation: In Vancouver, Aboriginal IDUs are becoming HIV positive at twice the rate of non-Aboriginal IDUs. Our findings emphasize the urgent need for an appropriate and effective public health strategy — planned and implemented in partnership with Aboriginal AIDS service organizations and the Aboriginal community — to reduce the harms of injection drug use in this population.
Little is known about the extent of the HIV epidemic among Aboriginal people in North America.1,2 The reasons for this include limited HIV/AIDS surveillance data, underreporting, and inconsistent documentation of ethnic status between provinces.2,3 However, because of the established links between entrenched poverty and risk of HIV infection, there have long been warnings that HIV/AIDS will increasingly affect Aboriginal people in Canada.4,5,6 Regrettably, with the few data available, alarming trends have already emerged. In 1990 an estimated 1% of all reported AIDS cases involved Aboriginal people; by 1999 this proportion had increased to 10.8%.2 Despite constituting only about 2.8% of the general population, Aboriginal people accounted for about 9% of all people with newly diagnosed HIV infection in 1999.2 Indeed, from 1996 to 1999 the estimated number of Aboriginal people with HIV infection rose from 1430 to 2740.2
In addition, there are some data to suggest that HIV/ AIDS among Aboriginal people is disproportionately affecting youth and women. In provinces with reported ethnicity data, 33% of Aboriginal people with HIV infection newly diagnosed between 1988 and 2000 were less than 30 years old, as compared with 20% of non-Aboriginal people with newly diagnosed HIV infection; a similar difference was observed in cases involving women (47% v. 20%).2 With the exception of national statistics indicating that injection drug use accounted for the majority (60%) of new infections among Aboriginal people between 1998 and 2000,2 risk factors that explain elevated risk and transmission of HIV among Aboriginal people are not well understood.
We have been following a cohort of more than 1400 injection drug users (IDUs) in Vancouver since 1996, of whom about 25% are Aboriginal people. At enrolment, HIV prevalence rates among Aboriginal IDUs were higher than their non-Aboriginal counterparts (31% v. 18%; p < 0.001). Follow-up of the cohort now allows for an investigation aimed at comparing HIV incidence among Aboriginal and non-aboriginal IDUs and identifying predictors of HIV seroconversion among Aboriginal women and men in the study.
Methods
The Vancouver Injection Drug User Study (VIDUS) is a prospective study involving 1437 people who were recruited through self-referral and street outreach from Vancouver's Downtown Eastside between May 1996 and December 2000. Individuals were eligible if they were 14 years of age or older, had injected illicit drugs at least once during the month before enrolment, resided in the greater Vancouver region and provided written informed consent. Participants were given a stipend (Can$20) at each study visit to compensate them for their time and to facilitate transportation. The study was approved by the University of British Columbia/Providence Healthcare Research Ethics Board.
At enrolment and semi-annually, participants completed an interviewer-administered questionnaire to elicit sociodemographic data and data on injection and non-injection drug use, injection practices and sexual risk behaviours. At each visit venous blood samples were drawn and tested for HIV and hepatitis C virus antibodies. All eligible participants had private interviews and pre- and post-test counselling with trained nurses; referral for HIV/ AIDS care was provided to those found to be HIV positive. Aboriginal status was based on self-report by individuals as Métis, Aboriginal or First Nations.
Variables of interest in this analysis included age, Aboriginal ethnicity, income, incarceration in the 6 months before the visit and stable versus unstable housing. Clients who reported having stable housing were those living in their own house or apartment. Unstable housing was defined as living arrangements that included single room occupancy hotels (SROs), transitional living arrangements (e.g., staying with relatives) and homelessness. Risky injection variables included borrowing and lending syringes that had been used by someone else and overdose experience. Drug use behaviours included frequent injection, type of drug and bingeing behaviour. As we have done previously,7,8 we described clients who reported injecting cocaine, heroin or speedballs (cocaine and heroin) once or more per day as frequent cocaine, heroin and speedball users respectively. Bingeing was defined as periods when drugs were injected more frequently than usual. Methadone maintenance therapy was defined as current use of methadone. Risk factors regarding sexual behaviour included having an HIV-positive sexual partner, having an IDU as a sexual partner, being a man who has sex with men, having an STD diagnosed in the 6 months before the visit and having unsafe sex. Unsafe sex was defined as not always using condoms with regular sexual partners, casual sexual partners or sex trade clients in the 6 months before the visit. Regular sexual partners were defined as those partners with whom the sexual relationship lasted for more than 3 months. Casual sexual partners were defined as those partners with whom the sexual relationship lasted less than 3 months. Sex trade clients were defined as those partners with whom sex was traded for drugs or money.
Data from all participants who were HIV negative at enrolment and completed at least one follow-up visit were eligible for inclusion in the statistical analysis. The event of interest in this study was HIV seroconversion. The date of seroconversion was estimated using the midpoint between the last negative and the first positive antibody test result. The cumulative incidence of HIV infection was calculated using the Kaplan–Meier method. In this analysis, time zero was defined as the date of enrolment. Participants who consistently remained seronegative were considered to be right censored at the time of their most recent test result. The log-rank test was used to compare seroconversion rates between Aboriginal and non-Aboriginal participants. Relative risks and 95% confidence intervals (CIs) were obtained for risk factors of interest. The Cox proportional hazards regression model was used to assess the independent effect of both fixed covariates (e.g., marital status, education level and unstable housing) and time-dependent covariates (e.g., frequency of injection drug use and sexual behaviours) on time to HIV seroconversion among Aboriginal participants. Variables that were found to be either significantly or marginally (p < 0.10) associated with time to seroconversion in the univariate analyses were considered for inclusion in the multivariate Cox regression models. Forward stepwise regression was used to model the effects of selected predictors on time to seroconversion. We explored factors associated with seroconversion in separate multivariate models for men and women. Because the number of observations in some cases was small, we explored factors associated with seroconversion and retained variables that remained marginally (p < 0.10) associated with time to serconversion in adjusted analyses. All p values were 2-sided.
Results
A total of 1437 participants were recruited and completed the enrolment questionnaire between May 1996 and December 2000. Of these, 941 were found to be HIV negative at enrolment and completed at least one follow-up visit during the observation period. Of the 941 participants, 230 (24.4%) were Aboriginal and 711 (75.6%) non-Aboriginal. Among the Aboriginal participants 101 (43.9%) reported being Aboriginal, 97 (42.2%) First Nations and 32 (13.9%) Métis. The proportion of participants who enrolled in 1996/97 was similar in the Aboriginal and non-Aboriginal groups (80% and 82% respectively; p = 0.87). Also similar was the mean duration of follow-up (37 and 38 months respectively; p = 0.77). The proportion of participants who completed 6 or more follow-up visits during the observation period was slightly higher in the Aboriginal group than in the non-Aboriginal group (70% v. 63%; p = 0.031). Table 1 shows the baseline sociodemographic and behavioural characteristics of the participants.
Table 1.
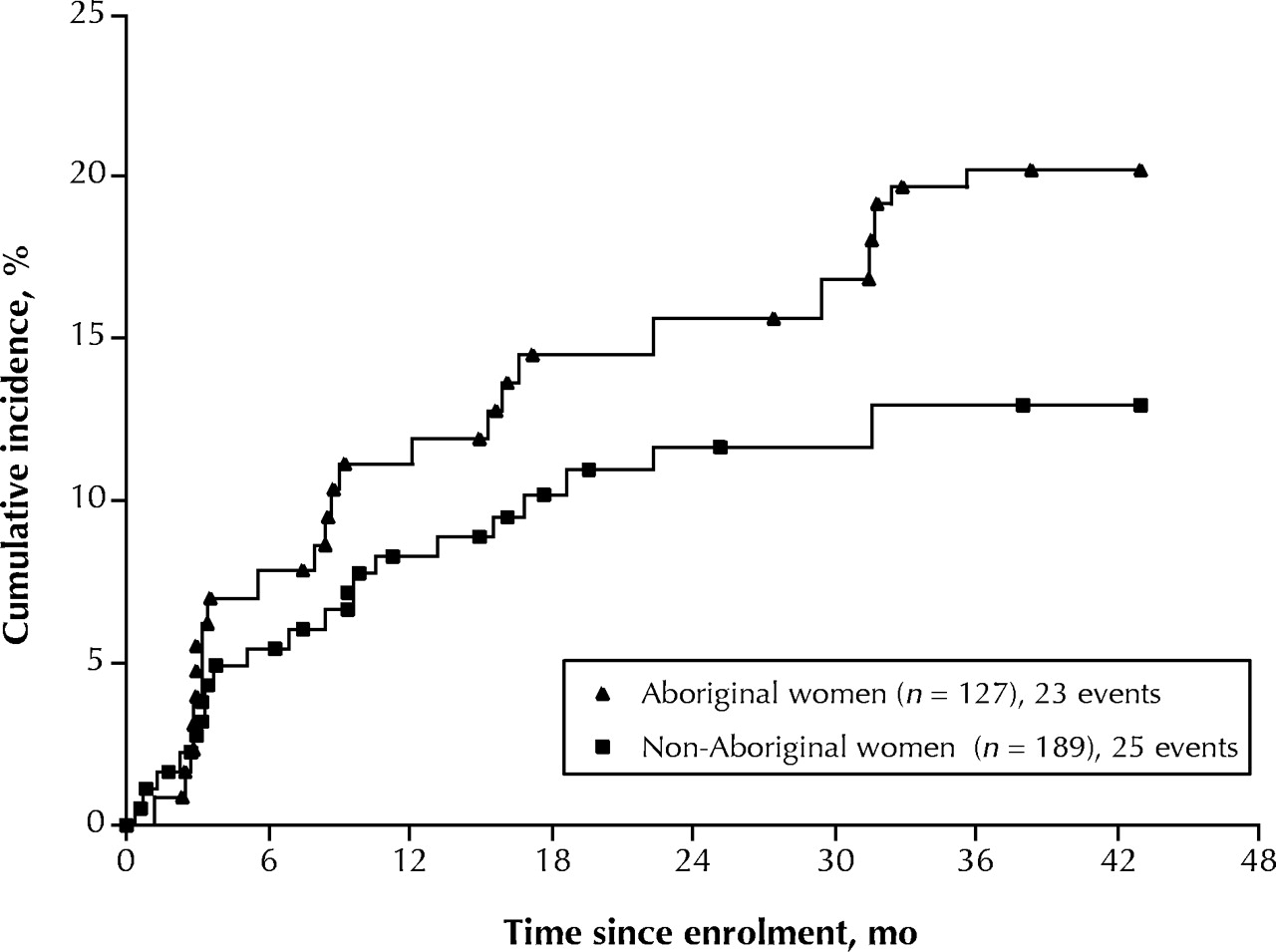
As of May 31, 2001, HIV seroconversion had occurred in 112 (11.9%) of the 941 participants, yielding a cumulative incidence of HIV infection at 42 months of 12.7% (95% CI 10.3%–15.1%). As seen in Fig. 1, the cumulative HIV incidence at 42 months in the Aboriginal group was about twice as high as in the non-Aboriginal group (21.1% v. 10.7%; p < 0.001). This elevation in risk was present in both Aboriginal men and women (Fig. 2). The cumulative incidence of HIV infection among the Aboriginal and non-Aboriginal women was 20.2% and 12.9% respectively; the latter difference did not attain statistical significance owing to the small sample (p = 0.12). The cumulative HIV incidence among the Aboriginal and non-Aboriginal men was 19.4% and 9.6% respectively (p = 0.007).

Fig. 2: Cumulative incidence of HIV infection among female (left) and male (right) Aboriginal and non-Aboriginal participants who were HIV negative at study enrolment (log-rank p value = 0.12 and 0.007 respectively).

{kind=link}
{kind=link}
Fig. 1: Cumulative incidence of HIV infection among Aboriginal and non-Aboriginal participants in the Vancouver Injection Drug User Study who were HIV negative at study enrolment (log-rank p value < 0.001).
Table 2 presents the univariate results of the Cox regression analysis of sociodemographic and behavioural variables and their association with time to HIV seroconversion. Among the female Aboriginal participants, frequent speedball injection (relative risk [RR] 3.5; 95% CI 1.5–7.8), frequent cocaine injection (RR 2.8; 95% CI 1.2–6.4) and going on binges of injection drug use (RR 2.6; 95% CI 1.2–5.9) were identified as significant predictors of seroconversion. Risk factors that did not attain conventional significance were frequent heroin injection (RR 2.1; 95% CI 0.9–4.6), requiring help injecting (RR 2.1; 95% CI 0.9–4.6) and incarceration in the 6 months before the visit (RR 2.0; 95% CI 0.9–4.5). A reduction in risk of marginal significance was noted among Aboriginal women who reported using condoms with their regular sexual partners (RR 0.2; 95% CI 0.02–1.29). No significant associations with time to HIV seroconversion were observed for the remaining sociodemographic and behavioural characteristics.
Table 2.
Among the male Aboriginal participants, significant predictors of HIV seroconversion in the univariate analyses were frequent speedball injection (RR 3.8; 95% CI 1.3–10.5), frequent cocaine injection (RR 3.0; 95% CI 1.2–7.6) and frequent heroin use (RR 2.5; 95% CI 1.0–6.2). Risk factors that did not attain conventional significance were unstable housing (RR 2.4; 95% CI 0.9–6.4) and frequent crack cocaine use (RR 2.6; 95% CI 0.8–7.8). No significant associations were observed for the remaining sociodemographic and behavioural characteristics.
The results of the multivariate analyses are shown in Table 3. Among the female Aboriginal participants, frequent speedball injection (adjusted RR 3.1; 95% CI 1.4–7.1), going on binges of injection drug use (adjusted RR 2.3; 95% CI 1.0–5.2) and using condoms with regular sexual partners (adjusted RR 0.2; 95% CI 0.02–1.2) were independent predictors of HIV infection, although the last risk factor was of marginal statistical significance. Among the male Aboriginal participants, frequent speedball injection (adjusted RR 2.9; 95% CI 1.0–8.5) and frequent cocaine injection (adjusted RR 2.5; 95% CI 1.0–6.5) were independent predictors of seroconversion.
Table 3.
Interpretation
Our findings show that the incidence of HIV infection among Aboriginal IDUs in Vancouver's Downtown Eastside is twice as high as the incidence among non-Aboriginal IDUs. This elevated risk was present in equal measure among both the male and female Aboriginal participants. The divergence between Aboriginal and non-Aboriginal IDUs suggests that this problem is continuing and perhaps worsening. Aboriginal people accounted for about 25% of the study group; however, they represent only 4%–5% of the total population in British Columbia,9 which suggests an overrepresentation of Aboriginal people among IDUs. As several Aboriginal AIDS service providers have suggested, injection drug use is considered to be one way Aboriginal people cope with the complex effects of discrimination, poverty and social dislocation, including the multigenerational effects of the residential school system.5,10,11 These data combine to underscore the grave potential for further spread of HIV infection among Aboriginal people.
Aboriginal women constituted about 40% of all the female participants and half of the women who became HIV positive. Results of recent studies in Baltimore,12 San Francisco13 and Vancouver7 have shown that the sex-related and drug-related vulnerabilities faced by female IDUs may be markedly different than those faced by their male counterparts and have acknowledged the more prominent role that sexual transmission may play in this particularly vulnerable subpopulation. Our observations are consistent with these earlier findings, since a reduction in risk was noted among female Aboriginal IDUs who reported using condoms with their regular sexual partners. However, most sexual health promotion programs targeting women focus solely on consensual sexual circumstances and often ignore the psychological effects of early sexual abuse and relationship violence on women's sexual decision-making.14 Given these complexities,15 prevention efforts aimed solely at the promotion of condom use will not suffice to deter the sexual transmission of HIV among Aboriginal women. In addition, binge use of injection drugs emerged as a strong risk factor among the Aboriginal women in our study. Combined, these data suggest that patterns of drug use may enhance sexual vulnerability among Aboriginal women. Policy-makers should initiate evidence-based programs that accommodate increased sex-related and drug-related vulnerabilities associated with bingeing.8,16
The strong association between frequent speedball injection and HIV infection among both the Aboriginal men and women appears to be a new finding and is of grave concern. In addition, speedball injection places users at high risk of overdose death.17,18 Interventions such as needle-exchange programs, particularly those that are restrictive in their distribution policies, may not suffice to address these problems, and more comprehensive injection safety programs are urgently required.8,19,20
Methadone maintenance therapy has been a primary treatment method for opiate addiction in Canada21 and has been shown to be effective at preventing HIV infection in people participating in methadone treatment programs.22 Although methadone maintenance therapy was not statistically significantly associated with a reduction in risk of seroconversion in our study, it is disconcerting that, at baseline, none of the Aboriginal men and few of the Aboriginal women were enrolled in a methadone treatment program despite significant proportions who reported frequent use of opiates. There have been recent expansions in the availability of methadone maintenance therapy in British Columbia (BC Ministry of Health Services: unpublished data). Whether these expansions have overcome the historical deficit in treatment provided to Aboriginal people should be the subject of further study. Also, increased efforts should be made to determine the barriers to receiving such therapy among Aboriginal people and to explore alternative therapies for opiate addiction.20
Several limitations of this study should be acknowledged. First, as was previously described,7,8 the study population was not a random sample of all IDUs and the analyses was based on self-reported behaviours. We have previously stated that we do not consider these factors to introduce significant distortions into our estimates.7,23 In the past, serosurveillance studies involving Aboriginal peoples have been externally driven and rarely developed in full collaboration with Aboriginal organizations and communities, which resulted in limited participation in HIV research.3,4,24 In our study, however, the follow-up rate among the Aboriginal participants was high, probably because VIDUS includes Aboriginal representation on its Community Advisory Board. We must acknowledge that the complex nature of risk in vulnerable subpopulations such as Aboriginal IDUs may not be adequately measured with our current instruments. Although the overrepresentation of Aboriginal people in the study group may appear to be due to sampling bias, we believe the VIDUS cohort is representative of IDUs in the Downtown Eastside community.7,23 Moreover, census data confirm that Aboriginal people are highly overrepresented in the neighborhood.25 Owing to the exploratory nature of our analysis, further studies will be required to confirm the risk factors associated with HIV seroconversion that were identified in our study. Furthermore, qualitative studies will be valuable in providing a better understanding of the HIV-related vulnerabilities that may be unique to Aboriginal people.
In summary, our findings show that the incidence of HIV infection among both male and female Aboriginal IDUs is twice that among non-Aboriginal IDUs and that risk factors among Aboriginal IDUs may vary by sex. Currently, British Columbia is developing a new AIDS strategy encompassing recommendations made by the BC Aboriginal AIDS Task Force.11 Our study highlights the urgent need for the rapid implementation of evidence-based prevention interventions that are planned and delivered in partnership with Aboriginal AIDS service organizations and the Aboriginal community.
Footnotes
-
Fast-tracked article
This article has been peer reviewed.
Contributors: Mr. Craib was responsible for the design of the analysis. Dr. Spittal was responsible for the interpretation of the findings, the literature review and the writing of the manuscript. Mr. Craib and Ms. Li conducted the analyses, contributed to the writing of the methods and results sections, was involved in revising the paper, and approved the final version. Ms. Laliberte was responsible for coordinating the collection of the data, including the follow-up of the subjects and the interviews, and was involved in revising the manuscript. Drs. Keath, Tyndall, Hogg and O'Shaughnessy were involved in the interpretation of the findings and in revising the final mauscript. Mr. Wood and Dr. Schechter were involved in the data analysis and interpetation of findings and contributed substantively to the final manuscript.
Acknowledgements: We are indebted to the study participants for their continued participation in VIDUS. We are also indebted to our research team for their conviction and continued commitment (Bonnie Devlin, Robin Brooks, John Charette, Suzy Coulter, Steve Kain, Guillermo Fernanadez, Caitlin Johnston, Will Small) and to Cari Miller and Arn Schilder for helpful discussions.
This study was supported by a grant (R01-DA11951) from the National Institute on Drug Abuse. Evan Wood is the recipient of fellowships from the BC Health Research Foundation and the Canadian Institutes of Health Research. Katherine Heath is the recipient of a postdoctoral fellowship from the Michael Smith Foundation for Health Research. Dr. Schechter holds a Canada Research Chair in HIV/AIDS and Urban Population Health.
Competing interests: None declared.
References
In this issue
Article tools



Jump to section
Related Articles
Cited By...
- Mortality in a large community-based cohort of inner-city residents in Vancouver, Canada
- The Cedar Project: risk factors for transition to injection drug use among young, urban Aboriginal people
- HIV prevention and psychoactive drug use: a research agenda
- Rate of methadone use among Aboriginal opioid injection drug users
- Factors associated with sex trade involvement among male participants in a prospective study of injection drug users
- Displacement of Canada's largest public illicit drug market in response to a police crackdown
- Potential use of safer injecting facilities among injection drug users in Vancouver's Downtown Eastside
- Adherence and plasma HIV RNA responses to highly active antiretroviral therapy among HIV-1 infected injection drug users
- Vide VIDUS
- Vide VIDUS
- OTHER ARTICLES NOTED (24 Jan 03 to 18 Apr 03)
- Reporting HIV infection
More in this TOC Section
Similar Articles
Collections

