


- © 2004 Canadian Medical Association or its licensors
The public generally considers natural products such as “health foods” and herbal remedies to be safe and beneficial. That these substances are largely unregulated contributes to the misconception that they are innocuous: patients don't feel the need to tell their physicians that they are using them, and physicians don't routinely ask patients if they are taking them. Yet there is a potential for these products to alter the action of certain drugs, sometimes with adverse clinical effects.
Natural products can “interact” with drugs by affecting the biological processes that regulate their metabolism and elimination. The family of enzymes known as the cytochrome P450s (CYPs)1 are heavily involved in the business of drug metabolism. Of its many subtypes, CYP3A4 is one of the most important; we will use it to illustrate how interactions between natural products and medications can occur.
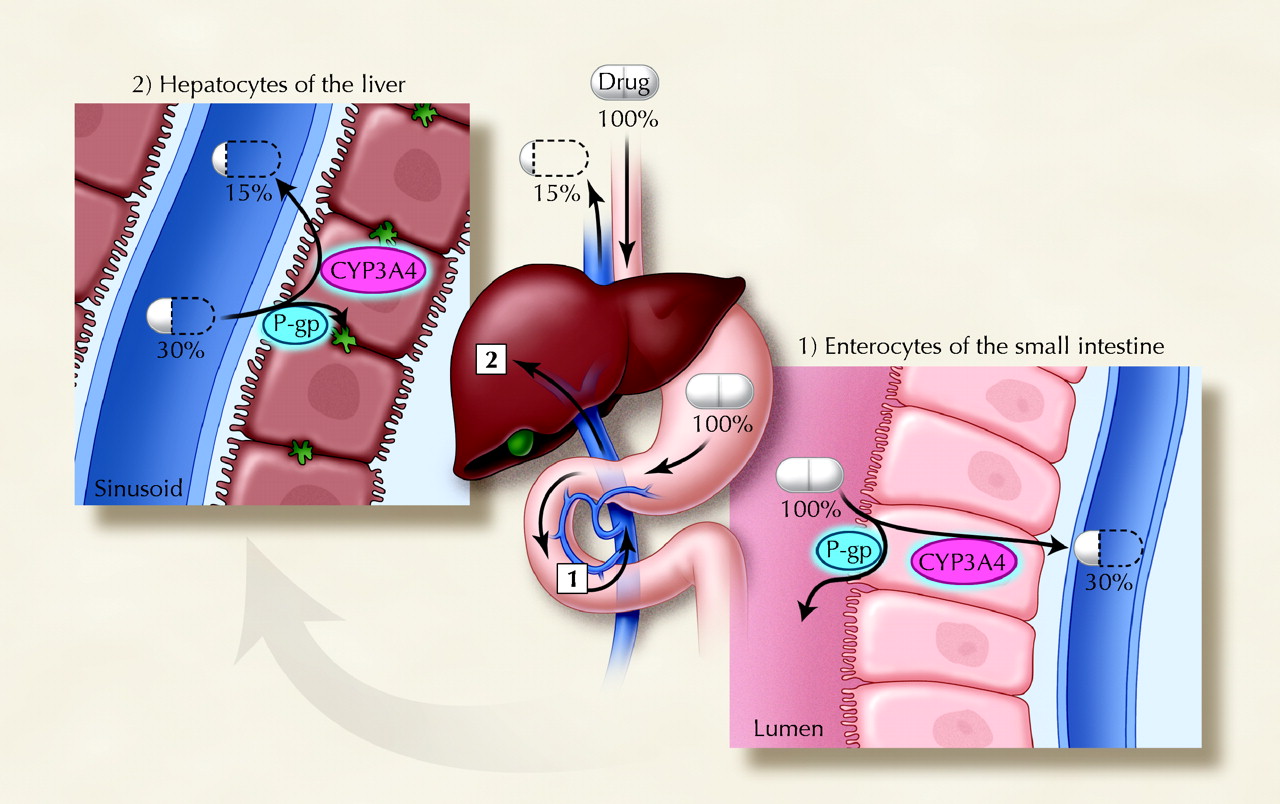
CYP3A4 has been estimated to at last partly oxidize 60% of all drugs to metabolites that are either less active or more readily excreted (or both). Its availability in the small intestine and liver enables it to inactivate orally administered drugs before they enter the systemic circulation (first-pass elimination), thereby reducing the drug's bioavailability (the percentage of an oral dose that reaches the systemic circulation unchanged). If the activity of CYP3A4 is altered, so too is the bioavailability of drugs that are oxidized by this enzyme (see Fig. 1).
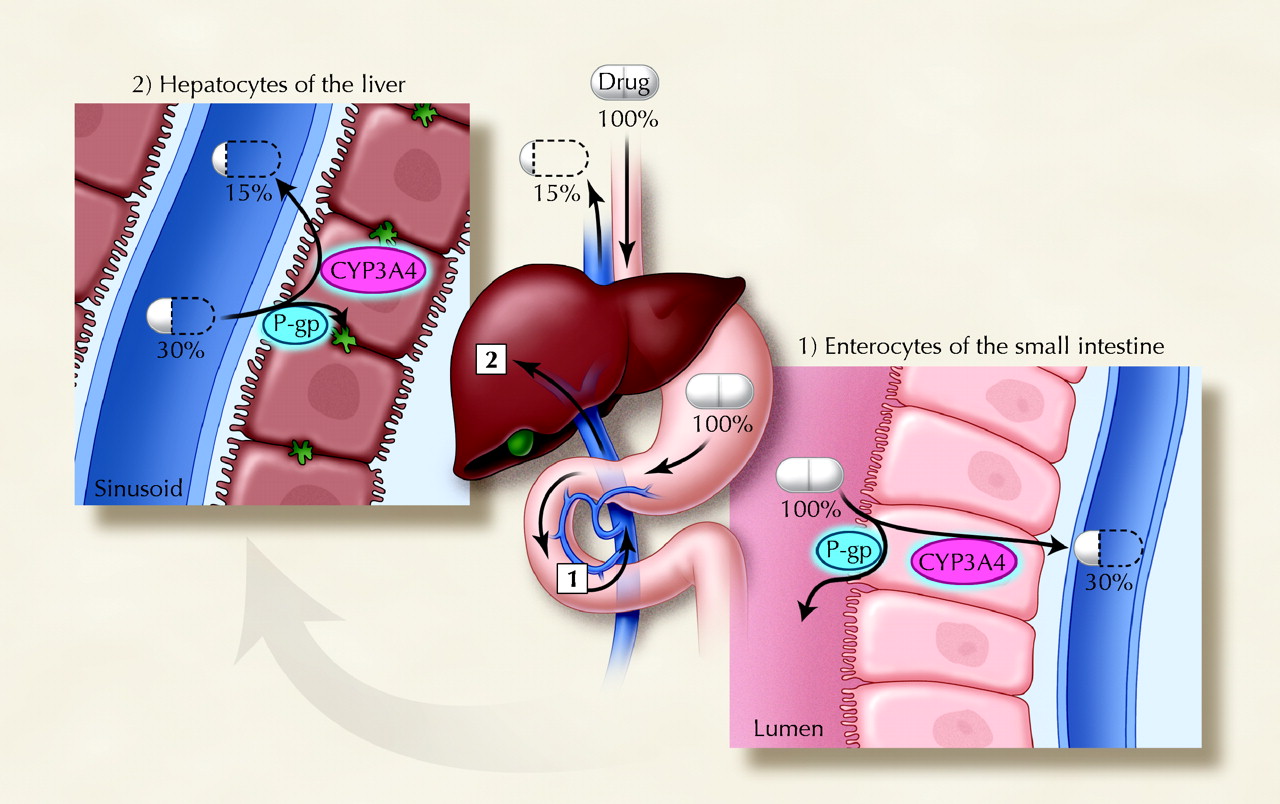
Fig. 1: Sequential first-pass elimination of a theoretical drug through metabolism by CYP3A4 and/or transport by P-glycoprotein (P-gp) in enterocytes of the small intestine and then hepatocytes of the liver. The percentage of the initial drug dose that is available before and after passage through the gut wall and liver is presented. Although the drug is 100% absorbed from the gastrointestinal tract, its bioavailability is only 15% after oral administration. Photo: Christine Kenney
One way that a natural product can alter the action of an enzyme is to inhibit it. Our group made the initial finding that grapefruit can markedly reduce enteric CYP3A4 activity, thus elevating the bioavailability of drugs metabolized by enteric CYP3A4 to potentially toxic levels.2 Grapefruit juice–drug interactions have been succinctly discussed in a recent article in this journal.3
St. John's wort, a herb that has become popular in the treatment of depression, has the opposite effect. It increases the activity of CYP3A4, thereby causing more complete oxidation of drugs; higher metabolism means lower bioavailability and hence diminished clinical response. Moreover, St. John's wort increases the activity of the drug transporter P-glycoprotein. Like CYP3A4, this transporter is expressed in apical enterocytes and hepatocytes. P-glycoprotein acts to pump drugs back into the intestinal lumen directly from the gut wall and indirectly from the liver via bile, thus reducing the bioavailability of orally administered drugs.4 P-glycoprotein is also located in the renal tubules, where it facilitates systemic drug elimination. The combined action of CYP3A4 and P-glycoprotein in the gut and liver can substantially decrease bioavailability and diminish effectiveness. The mechanism by which St. John's wort enhances the activities of CYP3A4 and P-glycoprotein is interesting. It does not involve an actual increase in the activity of individual enzyme and transporter molecules but, rather, induces transcription and translation, resulting in a higher quantity of CYP3A4 and P-glycoprotein. This effect is usually evident within a few days of repeated administration and lasts for approximately a week after discontinuation of St. John's wort.
The clinical consequences of diminished drug efficacy can be as devastating as those of enhanced drug toxicity. For example, St. John's wort was been shown to decrease plasma concentrations of cyclosporine and indinivir sufficiently to cause, respectively, organ rejection and increased HIV viral load.5,6 Although plasma concentrations of cyclosporine are routinely monitored, the basis for an observed loss of benefit during indinivir therapy may go unrecognized, possibly leading to the inappropriate discontinuation of an effective medication or the unnecessary addition of other drugs. Moreover, a broad range of medications appears to be affected. The list includes highly prescribed medications that are substrates for CYP3A43 or P-glycoprotein (digoxin, HIV protease inhibitors) and others that have been implicated in case reports (amitriptyline, theophylline, ethinylestradiol + desogestrel, warfarin).
Physicians should be wary that abrupt and unexplained changes or variability in the clinical status of a patient may be the result of a natural product–drug interaction; it is easy for substances such as grapefruit or herbal remedies to be overlooked as an underlying cause. Also, most herbal products have not been assessed for their potential to cause drug interactions. As a general rule, we recommend discouraging the use of those products for which there is no information. However, many patients will continue to use grapefruit and herbal medications regardless. Rather than immediately altering medication regimens in response to a change in a patient's clinical condition, taking a careful dietary and herbal history may be a more effective initial approach. Although the Compendium of Pharmaceuticals and Specialties (Clin-Info Section, Product Monographs) may be the most popular source of drug information among clinicians, software programs (e.g., Epocrates) and Internet sites (e.g., www.drug-interactions.com) can also be useful.
David G. Bailey Lawson Health Research Institute, London Health Sciences Centre Departments of Medicine and Physiology & Pharmacology George K. Dresser Lawson Health Research Institute, London Health Sciences Centre Department of Medicine University of Western Ontario London, Ont.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

