


Abstract
Background: Interdisciplinary health research is a priority of many funding agencies. We surveyed clinician and biomedical scientists about their views on the value and funding of interdisciplinary health research.
Methods: We conducted semistructured interviews with 31 biomedical and 30 clinician scientists. The scientists were selected from the 2000–2006 membership lists of peer-review committees of the Canadian Institutes of Health Research. We investigated respondents’ perspectives on the assumption that collaboration across disciplines adds value to health research. We also investigated their perspectives on funding agencies’ growing support of interdisciplinary research.
Results: The 61 respondents expressed a wide variety of perspectives on the value of interdisciplinary health research, ranging from full agreement (22) to complete disagreement (11) that it adds value; many presented qualified viewpoints (28). More than one-quarter viewed funding agencies’ growing support of interdisciplinary research as appropriate. Most (44) felt that the level of support was unwarranted. Arguments included the belief that current support leads to the creation of artificial teams and that a top-down process of imposing interdisciplinary structures on teams constrains scientists’ freedom. On both issues we found contrasting trends between the clinician and the biomedical scientists.
Interpretation: Despite having some positive views about the value of interdisciplinary research, scientists, especially biomedical scientists, expressed reservations about the growing support of interdisciplinary research.
Collaboration between health disciplines is a new priority of research institutions and funding agencies. Many of these agencies have undergone restructuring and have developed programs specifically to intensify interdisciplinary research. In 2007, the US National Institutes of Health created 9 interdisciplinary research consortia “as a means of integrating aspects of different disciplines to address health challenges that have been resistant to traditional research approaches.” 1 In 2000, the Canadian Institutes of Health Research (CIHR) was established with an express mandate “to forge a health research agenda across disciplines, sectors, and regions that embraces scientific opportunity and reflects the emerging health needs of Canadians, the evolution of the health care system and the information needs of health policy decision-makers.” 2
This change in priority has been attributed to 3 main factors: the need to answer complex health problems, the need to explore questions that are not confined to a single discipline and the need to provide effective solutions to societal problems. 3,4 Although the arguments advocating for interdisciplinary health research have evoked many kinds of promises, scientists undertaking collaborative research can also face many challenges. The past 10 years have seen a growing body of literature examining the impediments and facilitators to interdisciplinary collaboration. 3,5–14
Despite this growing interest, little is known about scientists’ opinions on the prevalent assumption that working across disciplines adds value to health research. Moreover, little consideration has been given to how scientists perceive the growing support of interdisciplinary research by funding agencies. In a survey commissioned by the CIHR, 36% of funded researchers indicated that their collaboration across disciplines had increased as a result of the agency’s establishment. 15 Whether this shift reflects researchers’ scientific interests or their attempts to secure funding by appealing to the agency’s policy of promoting interdisciplinary research is unknown.
As part of a broad research program investigating the integration of social science in health research, 16 we conducted this study to examine to what extent, and why, biomedical and clinician scientists are for or against the promotion of interdisciplinary research. We targeted these types of scientists because they were predominantly affected by the move toward interdisciplinary research that occurred after the creation of the CIHR.
Methods
Study design and participants
We used a study design of descriptive qualitative content analysis based on semistructured interviews. This approach is appropriate for exploring a multidimensional, social and sensitive issue. It allows for an in-depth understanding of the variety of reasons that may ground a more or less favourable perspective concerning a critical question. Approval for the study design was received from the research ethics boards of the University Health Network and the Université de Montréal.
We recruited biomedical and clinician scientists who sit, or have sat, on CIHR peer-review committees. Biomedical scientists included laboratory and basic scientists, such as geneticists, biochemists and molecular biologists. Clinician scientists included physicians who carry out predominantly clinical research such as randomized controlled trials and clinical epidemiology. We sought participants with experience on peer-review committees because (a) they have evaluated various types of research projects in the health domain, and (b) they are in a position to exert influence on scientific activities.
We selected participants through purposeful sampling 17 to include a variety of research areas, CIHR committees and university affiliations. We drew the sample from membership lists of CIHR peer-review committees, from the agency’s inception in 2000 through to 2006. We determined the number of participants to be interviewed using the saturation approach: new participants were added to our sample until no new themes were emerging. 18 A preliminary analysis was thus conducted after each interview. The main characteristics of the sample are summarized in Table 1.
Table 1: Characteristics of 61 scientists who responded to a qualitative survey about interdisciplinary health research
Data collection
We conducted interviews with 31 biomedical scientists and 30 clinician scientists. Because the participants were affiliated with universities across Canada, more than two-thirds were interviewed by telephone; the remainder were interviewed in person. Interviews were carried out by 2 team members (S.L. and M.A.). They lasted between 90 and 120 minutes and were audiorecorded with the participants’ consent. These recordings were transcribed verbatim; NVivo 7 qualitative software was used to organize the data. 19
The interview guide for our broad research program included more than 30 semistructured questions. We analyzed 2 themes in detail for this study: opinions concerning the assumed added value attributed to interdisciplinary research; and perceptions of the increasing support of interdisciplinary research by funding agencies. We did not prescribe a definition of interdisciplinary research because we were interested in how the participants would define it.
Data analysis
We used thematic content analysis to examine the data. 20 First, preliminary coding categories were generated that reflected the various viewpoints expressed by the respondents. Second, we analyzed and coded the transcriptions of each interview based on these categories, which were refined when necessary. Third, we compared the categories (and subcategories) between the 2 groups of respondents. Two investigators (S.L. and M.A.) independently read and coded all of the interview transcriptions. Any differences in interpretation were discussed until a consensus was reached.
Results
Participants expressed a wide variety of perspectives on interdisciplinary research and its promotion by funding agencies. Opinions ranged from full agreement that interdisciplinary collaboration adds value to research (described below as an “affirmative viewpoint”) to complete disagreement (“opposed viewpoint”). Many of the participants presented intermediate viewpoints, offering qualified perspectives on the assumed added value of interdisciplinary research. We divided respondents’ perspectives on funding agencies’ growing support for interdisciplinary research into 2 categories: one in which the level of support was seen as unwarranted, and one in which it was seen as appropriate. On both issues we found contrasting trends between the clinician and the biomedical scientists.
Perspectives on the added value of interdisciplinary research
Affirmative viewpoint
About one-third of the participants, most of whom were clinician scientists, felt that interdisciplinary research offers greater potential for understanding complex health problems (Table 2). When participants were asked to justify their favourable opinion, 3 themes emerged (Box 1). First, several participants said that interdisciplinary research offers greater understanding and broadens the application of scientific research. Many cited their personal experience in interdisciplinary research as a stimulating one: participants recalled how the integration of different perspectives brought new insights and enhanced the quality of their studies. Second, participants noted that interdisciplinary research strengthens the rationale for studies and allows basic scientists to appreciate how their highly specialized research is related to broader clinical or socio-economic issues. The third theme, predominant among the biomedical scientists, referred to methodologic and instrumental collaboration. Respondents described examples in which knowledge from one discipline was used instrumentally to carry out research in their own discipline. Drawing on their personal experience, they underscored the advances in knowledge enabled by collaborative work with experts outside of the health domain, such as engineers, physicists and bio- informatics/ genomics specialists.
Table 2: Respondents’ viewpoints on interdisciplinary research and its promotion by funding agencies

Box 1: Sample quotes illustrating respondents’ viewpoints on the prevalent assumption that interdisciplinary collaboration adds value to health research
Qualified viewpoint
Most participants, and a large proportion of biomedical scientists (Table 2), expressed qualified support for the added value of interdisciplinary research. This viewpoint was supported by a number of different arguments (Box 1). Above all, most respondents stressed that disciplinary research is just as valuable as interdisciplinary research: these modes of inquiry are seen as complementary, with disciplinary research providing indispensable depth and interdisciplinary research providing necessary breadth.
Participants also emphasized that the added value of interdisciplinary research is contingent upon a number of characteristics of the project, including the nature of the research problem, the disciplines involved, the level of integration among the disciplines and the overall quality of the research practice (Box 1). For example, participants felt that interdisciplinary research would be more relevant for addressing complex health problems in the population, whereas a disciplinary approach would be more efficient for understanding disease mechanisms. The epistemological or methodologic distance of the disciplines involved was another frequently mentioned issue. For instance, some commented that a joint venture involving basic and social sciences would be less fertile than one involving diverse basic sciences. Some participants were skeptical that a genuine integration of various disciplines is really achieved in many interdisciplinary teams; poor integration reduces the scientific power of interdisciplinary research. Finally, some respondents were dubious about the scientific quality of this new mode of inquiry. Although they recognized the value of interdisciplinary research, they believed that the combination of multiple approaches can be detrimental to scientific quality. The quality of research, rather than its interdisciplinary nature, would be the best guarantee of advancing knowledge.
Opposed viewpoint
Although they were a minority, some participants, predominantly biomedical scientists (Table 2), clearly opposed the assumption that interdisciplinary research is valuable. Three main points were raised by these participants (Box 1). First, invoking a scientific rationale, some claimed that the burden of proof should lie with interdisciplinary research to provide evidence that its results are valuable. Participants noted that they have never seen a rigorous scientific study comparing interdisciplinary and disciplinary research outcomes. Second, looking at the emerging teams currently burgeoning in the health domain, some believed that the combination of highly disparate disciplines represents a high risk, especially because most scientists have very specialized backgrounds and they have not been trained to work according to an interdisciplinary approach. Third, some participants felt that the added value of interdisciplinary research relates more to marketing and the public image of science than to the advancement of knowledge per se.
Perception of funding agencies’ growing support of interdisciplinary research
Level of support is appropriate
Some participants felt that the current level of support of interdisciplinary research is appropriate (Box 2). These participants noted that increased funding offers a warranted “catch up” for a previously underfunded type of research. Hence, it allows for a more adequate balance between disciplinary and interdisciplinary research. Some participants felt that, although the funding agencies’ promotion of interdisciplinary research represents a challenge for them, they see it as an opportunity to experience new ways of doing research or to foster an open-mindedness among health scientists. Contrary to other participants, these respondents believed the benefits of interdisciplinary research exceed the risks.
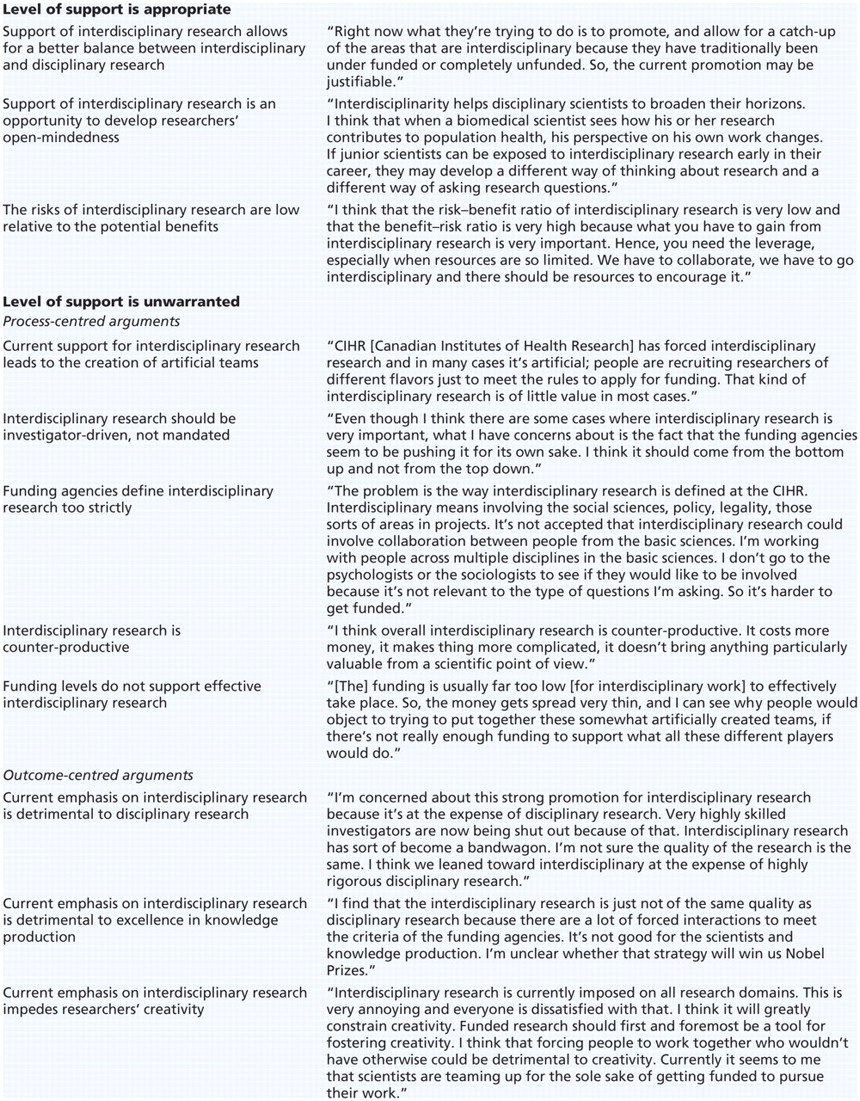
Box 2: Sample quotes illustrating respondents’ perceptions on funding agencies’ growing support of interdisciplinary research
Level of support is unwarranted
The vast majority of participants (44 of 61) felt that the funding agencies’ increasing level of support of interdisciplinary research was in some way unwarranted (Table 2). This unfavourable perception was predominant in both groups —more so among the biomedical scientists.
A wide range of arguments were raised in critique of funding agencies’ strong promotion of interdisciplinary research, and some participants mentioned more than one argument. We classified these arguments into 2 broad categories: process-centred and outcome-centred arguments (Box 2).
Process-centred arguments:
Two interrelated process- centred arguments were most recurrent. One was that funding agencies’ emphasis on supporting interdisciplinary research leads to the creation of artificial teams. The other was that a top-down process of imposing interdisciplinary structures on teams constrains scientists’ freedom and therefore threatens the quality of their work. The limited resources available for research encourage investigators to orient their project to meet explicit funding criteria. The establishment of a substantial number of granting programs dedicated to interdisciplinary research thus creates a pressure on scientists to recruit people of various disciplines on their team, even if they do not work together in a genuinely integrative manner. Participants spoke at length about this concern and claimed that interdisciplinary research should not be mandated by the funding agencies but should rather be investigator-driven. It should evolve naturally according to the issues the investigator considers to be critical for the advancement of knowledge. The research could involve scientists of different fields, with these scientists being recruited essentially to better grasp the complexity of the problem under study.
Participants’ comments also included 3 other process-centred arguments (Box 2). Some pointed to the “too strict” CIHR definition of interdisciplinary research, which encourages research teams to include collaboration across 4 “pillars” of health research (biomedical sciences; clinical sciences; health systems and services; and social, cultural, environmental and population health). This was judged to be too constraining and difficult to achieve in many contexts. Other participants felt that interdisciplinary research is counterproductive because it requires considerable human and financial resources and is more difficult to manage, such that the knowledge generated is not proportional to the investment. Finally, the funding level granted to interdisciplinary research teams was judged to be too low given the number of investigators involved. Hence participants saw the funding agencies’ promotion of interdisciplinary research as inappropriate given current budget constraints.
Outcome-centred arguments:
Three main themes relating to outcomes emerged from the participants’ unfavourable comments (Box 2). One referred to the prejudicial impact on disciplinary research. Participants felt that highly skilled investigators not involved in interdisciplinary teams are deprived of grants because of the funding agencies’ emphasis on interdisciplinary research. Hence, advancements of knowledge in disciplinary research were thought to be jeopardized.
A second argument offered by some respondents was that interdisciplinary research is not of the same scientific quality as disciplinary research, in part because of the often artificial nature of the teams.
The third argument was that the emphasis on interdisciplinary research impedes the creativity of scientists. Some participants believed that funding agencies’ influence on the research agenda becomes detrimental to free and innovative thinking.
Relation between perceived value of interdisciplinary research and funding agencies’ support
Logically, one might assume that participants who agreed that interdisciplinary collaboration adds value to health research would also consider funding agencies’ initiatives to encourage interdisciplinary research appropriate. Surprisingly, we found that half of the respondents who agreed that interdisciplinary research adds value also perceived the growing support by funding agencies to be unwarranted (Table 3). Hence, a positive attitude toward interdisciplinary research did not necessarily imply endorsement of funding agencies’ research agenda. Moreover, a vast majority (22 of 28) of the participants who provided a qualified viewpoint on the value of interdisciplinary research considered the current level of support by funding agencies to be excessive. Not surprisingly, all of the respondents who felt that interdisciplinary research does not add value to health research also perceived the growing support by funding agencies to be unwarranted.
Table 3: Perspective on whether interdisciplinary collaboration adds value to research, according to perspective on funding agencies’ growing support of interdisciplinary research
Interpretation
We found a wide range of views among health scientists concerning the prevalent assumption that collaboration across disciplines adds value to health research. Favourable views echoed the arguments put forward by promoters of interdisciplinary research. 1–3,8,21–23 For example, participants affirmed the belief that interdisciplinary research facilitates better understanding of complex health problems, adds social or ethical relevance to basic research and enables scientific progress through methodologic and instrumental collaboration.
Those expressing a qualified viewpoint emphasized that interdisciplinary research was valuable in addition to, but not in place of, disciplinary research. They also cautioned that the value of research lies in its scientific quality, independent of its disciplinary or interdisciplinary mode of inquiry. Various factors that can affect the value of interdisciplinary research were addressed. Some echoed factors identified in previous studies, such as the relevance of the disciplinary perspectives to the topic of investigation, 4,7,12,24 the epistemological distance between the disciplines involved, 16,25,26 and the integration of the research team. 5,11–13,25,27–29
Although they were a minority, some participants (mostly biomedical scientists) challenged the presumption that interdisciplinary research is a valuable approach. They claimed that evidence is required to support this conclusion and that interdisciplinary work represents a higher risk of failure. Some of their skepticism was rooted in the confusion about “what interdisciplinarity is.” This bewilderment confirms findings of previous studies showing that the distinction between “pluri-,” “trans-,” “multi-” and “cross-”disciplinarity is blurred for most scientists. 3,4,7,30,31
Our study offers 4 main contributions to the literature on interdisciplinary research. First, we have documented health scientists’ negative attitudes toward funding agencies’ growing support of interdisciplinary research, even among participants who agreed that collaboration across disciplines adds value to health research. Second, we have identified key sources of the negative attitudes: the creation of artificial teams because of funding agencies’ emphasis on supporting interdisciplinary research; and the top-down process considered to be detrimental to scientists’ freedom. The latter echoes some debate about scientists’ freedom and the tensions with granting institutions. 32–36 To what extent should interdisciplinary research be policy-driven or investigator-driven? This question needs to be explicitly addressed by all stakeholders involved in health research.
A third contribution of our study is the observation that disincentives to undertake interdisciplinary research not only relate to the practicalities or quality of the relationships between team members, as highlighted by numerous studies, 5–7,9–14,27–29 but also to skepticism regarding its outcomes and scientific quality. Although the potential of interdisciplinary research may be considerable, we cannot ignore that integrating different epistemologies, methodologies and paradigms is challenging and may be irrelevant for answering some research questions.
A fourth contribution of this study is that it highlights different trends in viewpoints between biomedical and clinician scientists. The latter group was more inclined than the former to value interdisciplinary research and view its promotion by funding agencies as justified. This can be linked to the different kind of problems, professional environments and stakes facing these 2 groups of scientists. This reiterates the question: Is interdisciplinary research equally appropriate to the diverse questions addressed by health researchers?
Limitations
Our study has some limitations. We included only 2 types of scientists. Also, we limited participants to members of CIHR peer-review committees. Hence, the transferability of findings may be limited. Further investigation on the views of health services scientists and social scientists is needed because their research practice is different.
Conclusion
Despite having some positive views about the value of interdisciplinary research, scientists, especially biomedical scientists, expressed reservations about funding agencies’ level of support of such research. Our findings suggest that, if the support is to be maintained or increased, efforts should be made to provide convincing evidence of its added value for tackling complex health problems. The valuation of interdisciplinary research should be sensitive to the unique context of each research problem. Furthermore, measures should be taken to avoid the undesired effects of funder-driven interdisciplinary research, such as the creation of artificial teams.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared.
Contributors: All of the authors contributed to the conception and design of the study. Mathieu Albert and Suzanne Laberge collected the data, and all of the authors contributed to the analysis and interpretation of the data. Suzanne Laberge drafted the article. Brian Hodges and Mathieu Albert revised it critically. All of the authors approved the final version submitted for publication.
Funding: This study was supported by the Canadian Institutes of Health Research (CIHR) grant no. KTE-72140. The CIHR played no role in the analysis or interpretation of the data or in the decision to submit the manuscript for publication.
Acknowledgement: The authors thank the biomedical and clinician scientists who participated in the study for giving their time for the interview.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

