


PSA screening remains a topic of considerable controversy for family physicians. The practice-based small group format, in which a group of physicians meet periodically to discuss clinical problems, is an excellent forum for the discussion of difficult issues.1 Our group of 9 family physicians has been meeting for practice-based small group discussions since 1996; one of us was initially trained by the Foundation for Medical Practice Education as a facilitator. We meet monthly for 1.5 hours. We decide which topics to discuss, which ensures that the sessions will be relevant to our local practices. Modules containing pertinent cases, commentaries and a summary of available evidence on various medical subjects are provided by the foundation. We review these prior to the study session and bring charts from our own practices. Despite our range in age and varied backgrounds we work extremely well together; the different viewpoints each physician brings to our meetings have been an asset to our group.
In our discussions of cases we apply the relevant evidence and focus on our communication skills in an attempt to improve the way we practise; we have found that our ability to problem solve and rely on our own resources as family physicians has been enhanced in the process. In a recent group meeting we decided to review CMAJs series of articles on prostate cancer[2–14] (see http://www.cma.ca/cmaj/series/prostate.htm), particularly the articles on screening with the prostate-specific antigen (PSA) test,[3, 5, 6] and discuss how the recommendations might be applied in our family practices.
Reflecting the discord in the literature,15 we could not arrive at a consensus about the use of PSA tests for screening purposes. Whether to initiate discussion about PSA screening with patients who do not ask about it is problematic for us. Informing all patients about the availability of the PSA test may well lead to increased screening with uncertain benefits. However, by not introducing the topic the physician runs the risk of being confronted by a patient who is later diagnosed with prostate cancer and wants to know why he was never informed about the availability of the PSA test. Certainly, some physician-initiated PSA screening is done to avoid this distressing situation. If the situation does arise there should be a full and honest discussion about why PSA screening was not offered, and a good physician-patient relationship and excellent communication skills are essential for this. The patient should be told that this test may or may not have benefited him; there is still no evidence that screening results in increased survival rates. For some, this test may simply mean more years living with the knowledge that they have cancer. As physicians we need to recognize our own discomfort with this situation and prepare for it. Before we met to discuss the issue of PSA screening, 3 physicians in our group reported that they did not normally discuss the topic with patients unless asked, and 6 said they provided information without being asked; our group discussion did not change this.
We all attempt to inform our patients about prostate cancer and the benefits and drawbacks of PSA screening before they decide for themselves whether to have the test. We currently give patients a handout from the Institute for Clinical Evaluative Sciences (available at http://www.ices.on.ca/docs/urology.htm) that provides this information in a clear and understandable manner. It is often difficult for us to discuss evidence-based information with many of our patients, however, because they have been led to believe from media reports that a PSA test after the age of 50 is essential. Failing to present a balanced view about this controversial issue is, in our opinion, a disservice to the public.
Our group agreed that PSA testing in men over 70 should be avoided;6 if a patient in that age group requests a PSA test we generally counsel against it. We agreed to restrict the use of PSA screening to men between 50 and 70 years of age unless they are at higher risk (e.g., black American men and those with a family history), in which case screening will be initiated at 40 years of age.
We discussed the frequency of testing at great length. Recommendations in the literature vary from every 2 years if the initial PSA result is less than 2.0 ng/mL16 to every 5 years if PSA is 4 ng/mL or below.5 Another report6 suggests following men with PSA results of 4 ng/mL and below with a test every 6 months for at least 3 consecutive tests. This approach, however, is of uncertain value because of variations in assays. Moreover, on a practical level it may be difficult to persuade asymptomatic low-risk patients to follow this course because of cost and inconvenience. Our current practice is to screen yearly, but screening every 5 years could be a reasonable alternative. Age-specific PSA ranges,6 although interesting, do not appear to be particularly useful in clinical practice; a lack of published guidelines and normal reference ranges, disagreement about cutoff values and the fact that age-related values vary according to race17 do not make them practical for use in primary practice.
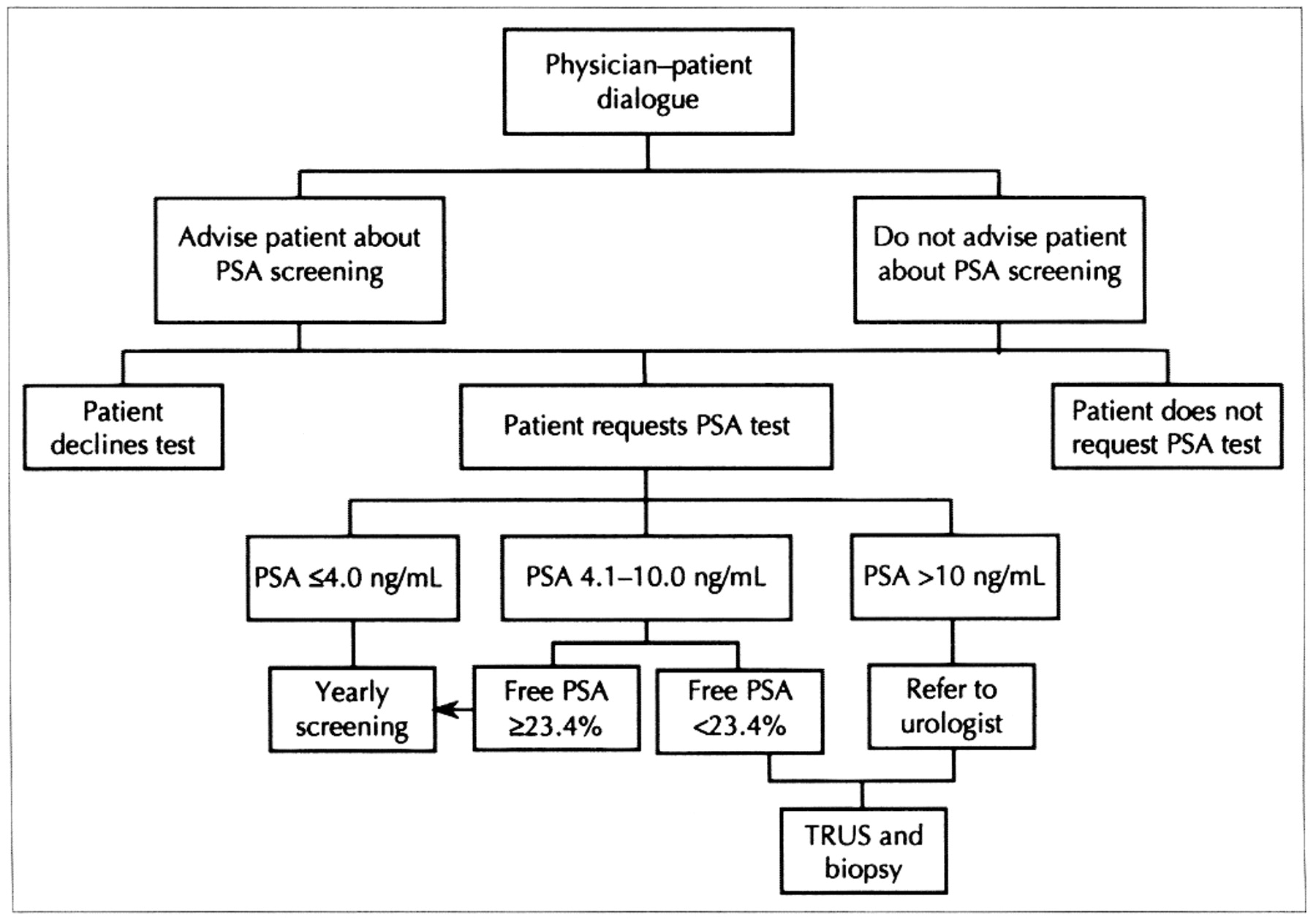
Karakiewicz and Aprikian6 suggest that transrectal ultrasonography and biopsy be recommended for men with a PSA test result over 4 ng/mL. However, the measurement of the percentage of free PSA may eliminate the need for biopsy in many patients, and we will be offering this test in our practices. Transrectal ultrasonography and biopsy will still be recommended if free PSA is below 23.4%, but if free PSA is 23.4% or more we will recommend continued observation with yearly screening. Retesting should be considered at 6 months for those with test results at the high end of normal. Because of the clear indications for transrectal ultrasonography and biopsy, the safety of the procedure and the burden of anxiety for patients, expedited referral for the procedure was recognized as an improvement in care. Fig. 1 presents a first approximation of a care map based on our interpretation of the articles we reviewed.
{kind=link}
Fig. 1: Suggested care map for men between 50 and 70 years of age at low risk for prostate cancer.
PSA screening continues to be problematic for us in primary care. If screening is undertaken, however, we must be more rigorous in our follow-up. Our meeting gave us the opportunity to review the most recent evidence on PSA screening and helped us determine how we could offer the best follow-up to patients should screening be initiated. We are now more aware of when to use the free PSA test and when to refer patients for transrectal ultrasonography and biopsy, and we hope to see this new knowledge translated into better outcomes for our patients.
Competing interests: None declared.
Footnotes
-
See related article page 791
Correspondence to: Dr. Michelle Greiver, 212-5460 Yonge St., Willowdale ON M2N 6K7; fax 416 221-3097; [email protected]
Members of the North York General-Branson Practice-Based Small Group: Michelle Greiver; Kenneth Jaskolka; Aaron Jesin; Irwin Keltz; Noel Rosen, Department of Family and Community Medicine, University of Toronto, Toronto, Ont.; Steve Rubenzahl; Martin Shack; Franklin Sheps; and Irving Zelcer, Department of Family and Community Medicine, University of Toronto, Toronto, Ont.
References
In this issue
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

