


- © 2008 Canadian Medical Association
Abstract
Background: Dementia can now be accurately diagnosed through clinical evaluation, cognitive screening, basic laboratory evaluation and structural imaging. A large number of ancillary techniques are also available to aid in diagnosis, but their role in the armamentarium of family physicians remains controversial. In this article, we provide physicians with practical guidance on the diagnosis of dementia based on recommendations from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, held in March 2006.
Methods: We developed evidence-based guidelines using systematic literature searches, with specific criteria for study selection and quality assessment, and a clear and transparent decision-making process. We selected studies published from January 1996 to December 2005 that pertained to key diagnostic issues in dementia. We graded the strength of evidence using the criteria of the Canadian Task Force on Preventive Health Care.
Results: Of the 1591 articles we identified on all aspects of dementia diagnosis, 1095 met our inclusion criteria; 620 were deemed to be of good or fair quality. From a synthesis of the evidence in these studies, we made 32 recommendations related to the diagnosis of dementia. There are clinical criteria for diagnosing most forms of dementia. A standard diagnostic evaluation can be performd by family physicians over multiple visits. It involves a clinical history (from patient and caregiver), a physical examination and brief cognitive testing. A list of core laboratory tests is recommended. Structural imaging with computed tomography or magnetic resonance imaging is recommended in selected cases to rule out treatable causes of dementia or to rule in cerebrovascular disease. There is insufficient evidence to recommend routine functional imaging, measurement of biomarkers or neuropsychologic testing.
Interpretation: The diagnosis of dementia remains clinically integrative based on history, physical examination and brief cognitive testing. A number of core laboratory tests are also recommended. Structural neuroimaging is advised in selected cases. Other diagnostic approaches, including functional neuroimaging, neuropsychological testing and measurement of biomarkers, have shown promise but are not yet recommended for routine use by family physicians.
The case
Mrs. E, a 72-year-old woman in your practice who has experienced clear and progressive memory decline over the past 3 years, finally agrees to come and see you with her daughter and husband for an assessment. The patient is English speaking and has a bachelor's degree. Her medical history includes hypertension, a 20-pack–year history of smoking and a previous transient ischemic attack. Her family says that she is unable to currently handle her own banking and has become lost when driving. Mrs. E is increasingly anxious when left alone. Her husband is concerned that she might be depressed, but he adds that his mother-in-law developed dementia at age 80. Findings on physical examination are negative aside from Mrs. E's decreased cognitive abilities, which include disorientation to date and day of the week. She scores 24 out of 30 on the Mini-Mental State Examination, losing points for temporal orientation, short-term recall of test items and naming of test objects. Mrs. E's daughter asks you if her mother has Alzheimer disease.
What further diagnostic work-up should you perform to establish the diagnosis?
This hypothetical case highlights a range of issues that commonly emerge in the diagnosis of a mild dementia. Cognitive impairment and dementia are present in about 20% of the elderly population and are consistently rated among the top 3 concerns of elderly people.1 Accurately diagnosing dementia remains a challenge for family physicians and specialists. There are 5 reasons why family physicians in Canada should develop expertise in dementia diagnosis. First, increasing numbers of elderly patients will be presenting with memory complaints to their family physicians.1 Second, current planning for geriatric and neurologic services in Canada works under the assumption that the burden of dementia diagnosis will largely fall on the shoulders of family physicians. Third, there continue to be a small subset of treatable disorders presenting as memory loss that must not be missed. Fourth, planning by families of elderly patients is most effective when dementia is diagnosed early in the illness. Fifth, symptomatic therapy that exists for Alzheimer disease is underused, alternative approaches are necessary for other conditions such as vascular dementia and frontotemporal dementia, and the list of therapies specific for different dementia diagnoses is likely to grow in the future. Accurate diagnosis is the prerequisite for optimal therapy.
There has been a wealth of research into the role and utility of different diagnostic methods over the past decade. The work has led to the development of better cognitive screening tools and more specific (and often expensive) means of diagnosing Alzheimer disease. Although numerous novel approaches have reached the mainstream media and received wide publicity, much confusion exists over which methods are sufficiently valid, reliable, available and inexpensive enough to warrant wide use by family physicians.
In this article, we provide physicians with practical guidance on the diagnosis of dementia based on evidence-based recommendations from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (Box 1). A description of the process used to generate the recommendations is provided in the first article of this series1 and in an online appendix accompanying this article (available at www.cmaj.ca/cgi/content/full/178/7/825/DC2). Published background papers provide details of the evidence-based reviews on which the recommendations are based.8–13

Approach to diagnosis
The diagnostic process in dementia has 3 major conceptual components: the clinical diagnosis, a logical search for the cause, and the identification of treatable comorbid conditions and other contributing factors, such as the degree of cerebrovascular disease. The diagnostic process should involve 6 main steps: taking the patient's history, interviewing a caregiver or family member, physical examination, brief cognitive tests, basic laboratory tests, and structural imaging for patients meeting certain criteria. The conclusion involves meeting with the patient and his or her family to discuss the results and diagnosis, and their implications. Practically speaking, the diagnosis is rarely “urgent,” and these steps are best carried out during repeated visits with the family practitioner over the course of weeks. Families should be alerted that this is an important process that warrants their time and effort. Most provinces have billing codes to allow adequate reimbursement of such assessments when spread over an extended period. In the following sections, we will outline these steps in more detail and address a number of other ancillary diagnostic methods, specifically functional imaging, neuropsychological testing, and measurement of blood and cerebrospinal fluid biomarkers. These last 3 diagnostic methods are usually restricted to specialist practice, but it is not uncommon for families to request information from their family physicians about the latest test for Alzheimer disease.
Clinical evaluation
Despite the remarkable progress that has been made in the basic neurosciences elaborating the molecular genetics, pathophysiology and neurochemistry of the degenerative dementias, the diagnosis of dementia is one that is still made clinically in the office, with a history from the patient, collateral history from an informant, and a physical examination. This must be supplemented by a cognitive assessment. The sensitivity for each of these components in detecting dementia varies strongly with the degree of dementia, moderate dementia being far less challenging to detect than very mild dementia.
Patient history
The history taking should focus on the cadence of the illness (gradual and insidious in Alzheimer disease, stepwise in vascular dementia) and the relation to any vascular events such as stroke. Causes of dementia such as alcohol abuse and renal failure should be assessed. Vascular risk factors, including hypertension, diabetes mellitus, smoking history, family history of stroke and lipid status, should be ascertained. Risk factors such as family history of dementia or repetitive head trauma, and protective factors such as high education level, should also be ascertained.
Family interview
A separate history taken from a caregiver or family member with the patient absent is obligatory. It is necessary to ascertain whether the memory complaint represents a consistent change from the previous level of function. Frontotemporal dementia is characterized by early personality changes that the patient will almost invariably fail to note or report. Reports of “embarrassing behaviour” or even functional impairment will often not be mentioned by family members if the patient is present. Functional impairment should be directly assessed and significant impairment documented. This involves questioning the caregiver or family member about the patient's independent performance of activities of daily living, such as feeding and toileting. In early dementia, the functional impairment is more likely to emerge in “higher” functions, such as the ability to carry out complicated financial affairs such as banking, the ability to use public transport or to drive, normal attention to hobbies, and the ability to learn to use new machines or appliances.14 This interview is also an opportunity to gauge family support systems and the social setting, which may prove crucial in the future management of the patient. A separate visit may often be arranged for such a family interview.
Physical examination
During the physical examination, the physician should pay particular attention to the potential signs of stroke, including hyperreflexia, extensor plantar responses, frontal gait apraxia and pseudobulbar palsy. The presence of small-vessel ischemic cerebrovascular disease with concurrent senile neuritic plaques and neurofibrillary tangles increases the risk of dementia by an estimated 20 times.15
Brief cognitive tests
All patients evaluated for dementia should have their cognitive function evaluated. Brief cognitive tests serve to determine the presence and overall severity of memory and cognitive deficits and can be recommended for both primary care and specialty practice (Table 1). They have grown to be part of the lexicon of communication across health disciplines caring for individuals with dementia. All such tests are a trade-off between the practical need for brevity and the importance of reliably documenting impairment across a set of cognitive domains, as is required for a clinical diagnosis of dementia. In essence, all brief cognitive tests have a lower sensitivity and specificity than does a full neuropsychological evaluation, but they are far faster and more accessible than specialized testing.
Table 1.
The Mini-Mental State Examination (MMSE)19 remains the most widely used instrument, with high sensitivity and specificity for separating moderate dementia from normal cognition. It requires little training, is administered in about 10 minutes and has vast medical acceptance. A rough rule of thumb is that patients with mild dementia usually have a score of 18–26 out of 30, those with moderate dementia a score of 10–18, and those with severe dementia a score of less than 10. Some clinical trials of Alzheimer disease have accepted only patients with a score of less than 24.16 At scores above this level, the Mini-Mental State Examination lacks sensitivity for the diagnosis of mild dementia, and other assessments are needed. The Mini-Mental State Examination focuses on memory, attention, construction and orientation domains. The Modified Mini-Mental State Examination is a more expanded version that also includes assessment of delayed recall20 and has been widely used in clinical and research settings in Canada.
The clock-drawing test evaluates general executive functioning of the frontal lobe, as well as visuospatial abilities (Figure 1).22 It requires 5–10 minutes to administer and has achieved widespread clinical use. Like the Mini-Mental State Examination, however, the clock-drawing test may lack sensitivity for the diagnosis of early or mild dementia.18

Figure 1: Clock drawings and test scores for patients without dementia and those with Alzheimer disease or suspected frontotemporal dementia. Patients are instructed to draw a clock face with all the numbers in it, and to show the time as 10 minutes past 11. The list of criteria used to determine a patient's score appears only in the print version of this article and is reproduced from Freedman et al.21). Images courtesy of Dr. Howard Feldman, ACCORD Lab, Brain Research Centre, University of British Columbia Hospital, Vancouver, BC
A number of newer tests have been developed to provide improved sensitivity. Of these, it is worth mentioning the Montréal Cognitive Assessment,2 DemTect,3 the 7-Minute Screen,4 the General Practitioner Assessment of Cognition5 and the Behavioural Neurology Assessment short form.6 All of these tests have been shown to be more accurate than the Mini-Mental State Examination in discriminating between dementia and normal cognition, particularly in cases of very mild dementia.2–6 The General Practitioner Assessment of Cognition5 requires 5–10 minutes to administer and was evaluated in family practice offices in Australia. The other tests require about 10 or more minutes to administer, were evaluated in specialty clinics or population studies and are used to evaluate multiple cognitive domains. This coverage probably makes them more accurate in detecting dementia in heterogeneous populations, but this remains to be proven. Although consideration of the details of these tests is beyond the scope of our review, interested readers may refer to the background paper by Jacova and colleagues3 on neuropsychological testing and brief cognitive testing (see the Editor's Note at the end of the article for information on how to obtain a copy). We lack clear knowledge of the advantages of one brief cognitive test over the others. At this point, the best advice is for physicians to gain experience and familiarity with one test and to use it routinely for diagnosing dementia.
Does the patient meet criteria for dementia?
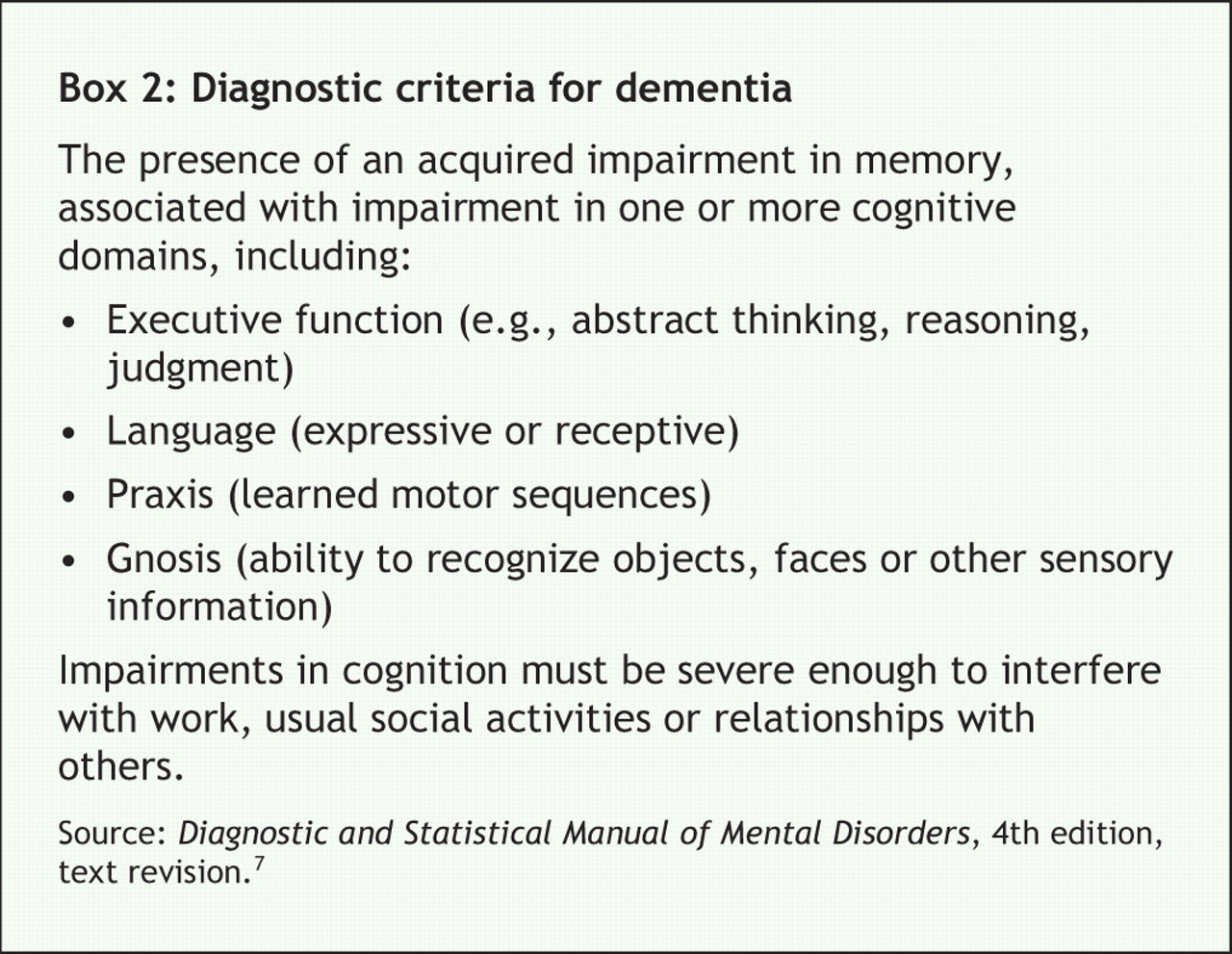
At this point in the evaluation, the physician has accumulated sufficient information to decide whether the patient meets clinical criteria for dementia (Box 2). There is good evidence that clinical diagnostic criteria for dementia can be readily applied at the bedside. Well-validated criteria such as the Diagnostic and Statistical Manual of Mental Disorders, third edition, revised (DSM-III-R),23 and fourth edition, text revision (DSM-IV-TR),7 form the most widely used diagnostic framework in Canada. Objective testing of memory and cognitive function is fundamental to the application of these diagnostic criteria.
The challenges in diagnosing dementia should not be understated. It can be difficult in some individuals with mild dementia to reliably demonstrate objective cognitive impairment as well as functional impairment. Some individuals without dementia can score low in the Mini-Mental State Examination, and only a score below 20 provides specific evidence for dementia.24 Conversely, dementia is possible even with a Mini-Mental State Examination score greater than 26.25 Furthermore, the score may vary by several points from one evaluation to the next. Language barriers, advanced age and low education can also confound the results and provide false-positive scores. A briefer test, such as the clock-drawing test, has the same challenges. No one brief cognitive test has been found to be superior over the others. No brief cognitive test has been developed to differentiate between subtypes of dementia, and none can be recommended for this purpose.26 Often the best recommendation is to repeat the testing on several occasions over several months, to provide more convincing evidence of cognitive impairment. The documentation of functional impairment can also be challenging. If the patient had limited premorbid activities, it can be difficult to document convincing functional decline for several years.
Differential diagnosis
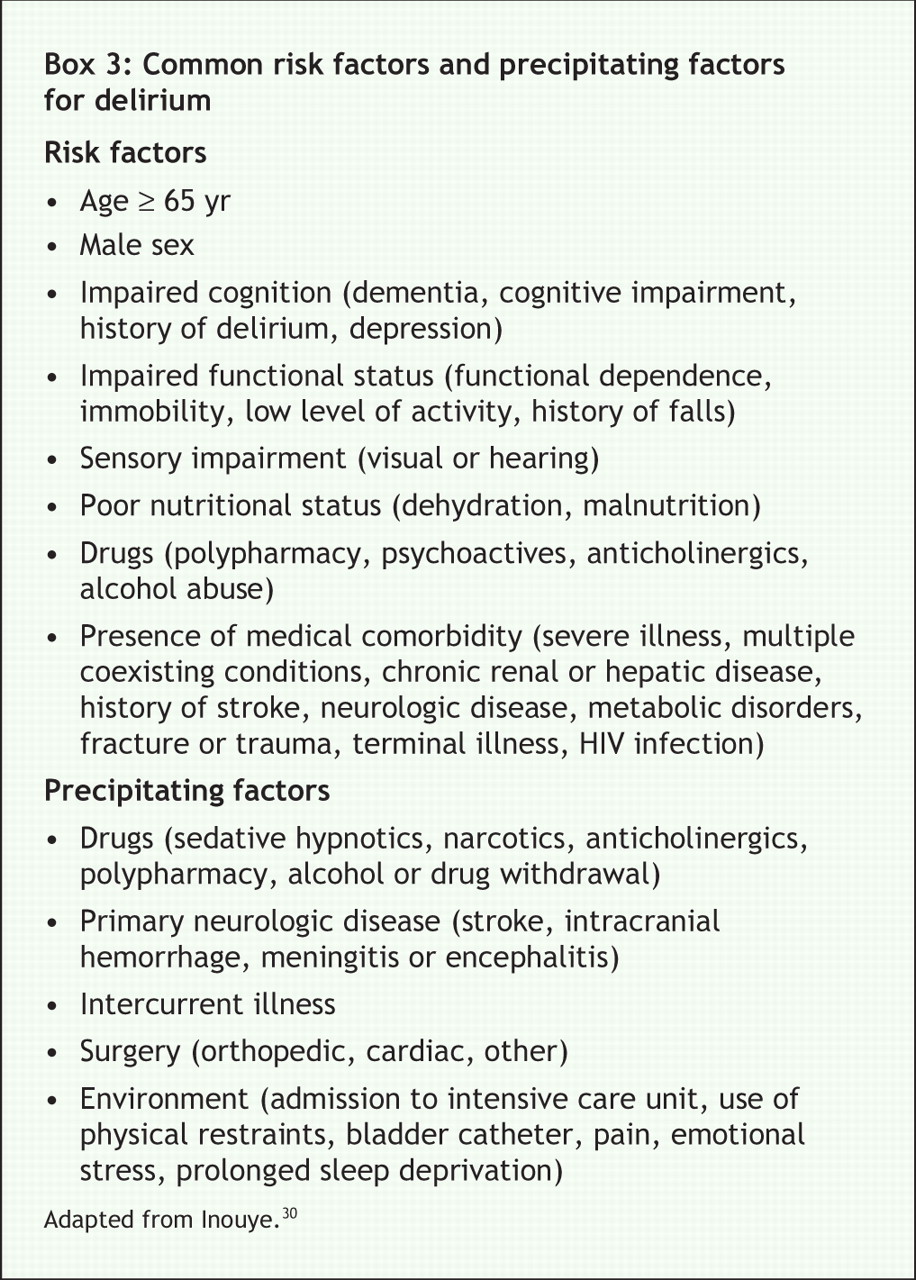
Having established the presence of a dementia, the specific cause should be determined. This determination relies on clinical evaluation, along with laboratory investigations and structural imaging (discussed in more detail in the next 2 sections). In considering diagnosis of a degenerative dementia, it is important to exclude delirium, a condition that is a transient, usually reversible, acute confusional state. Its clinical hallmarks are impaired attention and fluctuations in levels of consciousness. Delirium is a medical emergency with an increased risk for morbidity and death, and as such it is particularly significant in the differential diagnostic considerations.27–29 It calls for immediate investigation and management of treatable medical conditions. Individuals with dementia are at risk for delirium; however, the initial diagnosis of dementia should not be made while the patient is in a delirious state. The most common risk factors and precipitating factors for delirium are listed in Box 3.30
Depression and its contributing role in creating a “pseudodementia” has received considerable emphasis in the past.31 It is now appreciated that some degree of depressive symptoms, anxiety and apathy are quite common in the prodrome and course of Alzheimer disease.32,33 Asking the patient, or a family member or caregiver, about vegetative symptoms, including disorders of sleep, appetite and weight, can further address this diagnostic possibility of depression and the need for its treatment. Important symptoms to review include the presence of feelings of guilt, loss of enjoyment of pleasurable activities, current outlook and suicidal ideation.
The spectrum of dementias seen in patients referred to dementia clinics in Canada is provided in Table 2.34 The significant majority of dementia referrals in this setting are clinically diagnosed as Alzheimer disease, either alone or in association with other comorbid conditions such as cerebrovascular disease, Parkinson disease or Lewy bodies. The aging brain is recognized to frequently play host to multiple pathologies. In particular, it has been increasingly appreciated that senile neuritic plaques and neurofibrillary tangles often exist with concurrent cerebrovascular lesions.35
Table 2.
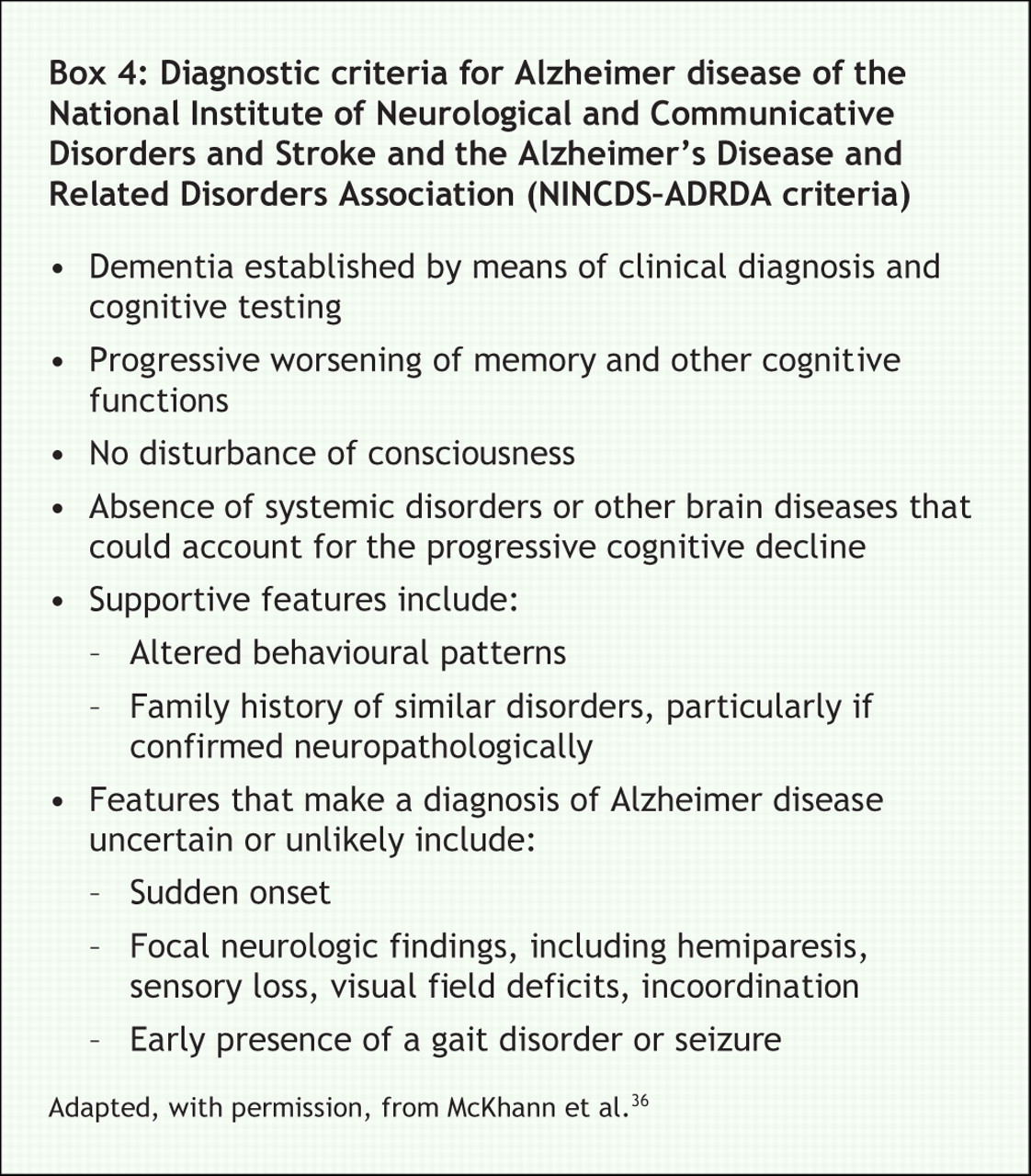
In terms of clinical criteria for Alzheimer disease, the diagnostic criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (NINCDS–ADRDA criteria) (Box 4) have been the most widely adapted for clinical use and have been neuropathologically validated.36,37
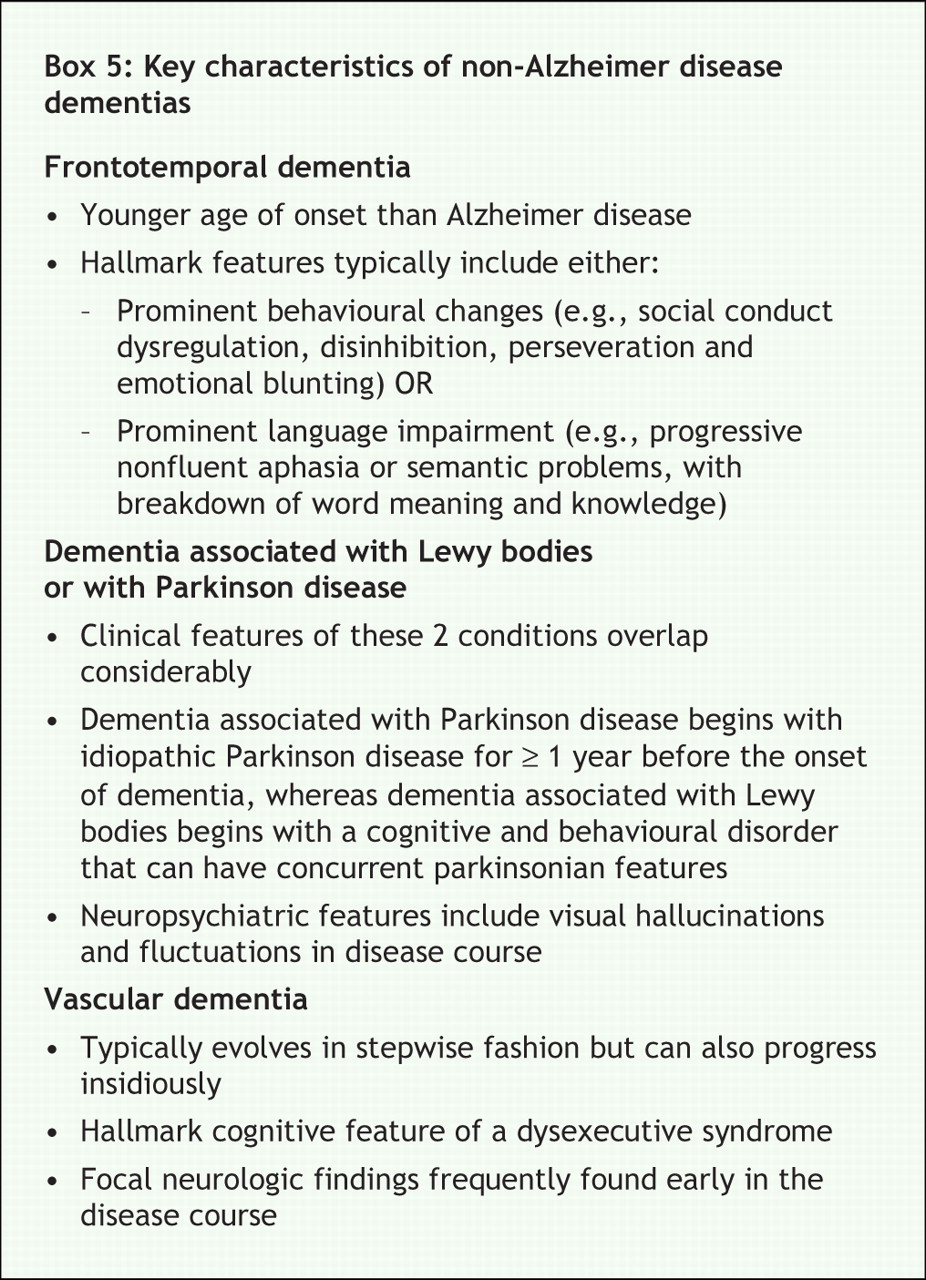
A brief description of the key characteristics of non-Alzheimer dementias is provided in Box 5.

Laboratory investigations
The primary role of laboratory investigations and structural neuroimaging with computed tomography or magnetic resonance imaging is to rule out the rare presence of a treatable disorder presenting as memory loss, such as renal failure, brain tumour, normal pressure hydrocephalus and subdural hemorrhages. Recent studies have found such “treatable dementias” to account for less than 1% of dementia cases.38 The previous consensus conference on the assessment and treatment of dementia reviewed the best evidence to guide laboratory investigations.39 It recommended basic investigations for all patients, including complete blood count, thyroid stimulating hormone, and serum calcium, electrolytes and fasting glucose. Other laboratory tests were to be applied selectively based on an individual's presenting medical history, and cognitive and physical examination findings. Selective testing of serum vitamin B12 and folate levels, rapid plasma reagin for syphilis screening, and HIV antibodies were recommended.
The current recommendations for core laboratory investigations have not changed except for the measurement of serum B12 levels, which is now recommended for all older adults who have suspected dementia or cognitive impairment (Box 1). There is insufficient evidence to recommend testing of red blood cell folate or serum folic acid levels. Since the introduction of folic acid fortification of grain products in Canada in 1998, folate deficiencies are rare, and testing of red blood cell folate levels is recommended only if the patient has a history of inadequate diet, celiac disease or other conditions preventing the ingestion of grain products. The measurement of homocysteine levels has been a recent focus of attention, with epidemiologic studies suggesting that elevated levels may be a risk factor for Alzheimer disease and vascular dementia. There is insufficient evidence to recommend the measurement of homocysteine levels or the treatment of elevated levels. Genetic testing, including screening for the apolipoprotein E gene, is not recommended.
Neuroimaging with computed tomography and magnetic resonance imaging
The availability of neuroimaging with computed tomography or magnetic resonance imaging permits a detailed assessment of the structural patterns of brain atrophy, with particular attention to the medial temporal lobe, where the early atrophy in Alzheimer disease can be seen (Figure 2). In addition, neuroimaging allows exclusion of neurosurgical lesions, including tumours, subdural hematomas and hydrocephalus. The previous recommended indications for computed tomography scanning have not changed41 (Box 1). The selective use of computed tomography as part of the work-up for dementia is still recommended.

Figure 2: T1-weighted coronal magnetic resonance imaging scan showing extensive hippocampal atrophy (arrows). These landmarks are based on a visual rating scale of medial temporal lobe atrophy developed by Scheltens and colleagues.40. Image courtesy of Dr. Howard Feldman, ACCORD Lab, Brain Research Centre, University of British Columbia Hospital, Vancouver, BC
There is fair evidence to add the indication of using computed tomography or magnetic resonance imaging to rule in concomitant cerebrovascular disease. It was not possible on the basis of the available evidence to separate the indications for computed tomography from those for magnetic resonance imaging.
Additional procedures for diagnosis
Functional neuroimaging
In addition to imaging techniques that look at brain structure (computed tomography and magnetic resonance imaging), there are techniques that look at the function of brain tissue and can visualize brain activity in vivo. There has been significant recent progress in these techniques. Modalities of functional neuroimaging include positron emission tomography with fluoro-D-2-deoxyglucose, single photon emission computed tomography, functional magnetic resonance imaging and magnetic resonance spectroscopy. They vary from being widely available (single photon emission computed tomography) to being available only in research settings (magnetic resonance spectroscopy). None of these technologies is recommended for current routine diagnostic evaluation of dementia. Nevertheless, there is fair evidence that positron emission tomography or single photon emission computed tomography can assist specialists in diagnosing cases of questionable early dementia or in discriminating between frontotemporal dementia and Alzheimer disease.
Neuropsychological testing
Beyond the administration of brief cognitive tests, it is possible in many settings to refer patients for neuropsychological testing. However, such referrals should be made selectively in clinical settings42 (Box 1). Neuropsychological testing routinely requires 2–4 hours of the patient's time, costs between $600 and $1500 and is often not covered by provincial government insurance plans. Within hospitals, there can be long waiting times for a neuropsychological evaluation, which can also limit its utility in routine dementia diagnosis. The diagnosis and differential diagnosis of dementia remain a clinically integrative process, with neuropsychological testing providing supportive evidence only. Nevertheless, neuropsychological testing provides detailed, standardized assessment across a wide range of cognitive domains, and with expert interpretation it has shown utility in distinguishing early or mild dementia from mild cognitive impairment or cognitive impairment without dementia and from normal cognitive function.43–45 Neuropsychological testing has greater sensitivity than brief cognitive tests in documenting clear cognitive abnormalities across a range of cognitive domains. (The topics of mild cognitive impairment and cognitive impairment without dementia will be covered extensively in the next article in the series.)
There is evidence that neuropsychological testing can contribute to determining the likelihood of future dementia in at-risk groups.46 Neuropsychological testing has demonstrated utility in distinguishing between dementia subtypes, for instance, in suggesting that there might be frontotemporal dementia rather than Alzheimer disease.47–49 In this sense, the impairment that is detected through neuropsychological testing has considerable specificity, far greater than brief cognitive testing.
Measurement of biological markers
A biological marker of a disease can be defined as a measurable change in the physical constitution of a host that indicates the presence of that disease. The successful development of a specific biomarker for Alzheimer disease that could distinguish Alzheimer disease from normal aging and other forms of dementia would represent a major advance. Although there has been definite progress along this path, there is no ideal biomarker currently available. There are rare genetic factors that are invariably causative of early-onset familial Alzheimer disease.50 They do not play a role in the vast majority of cases of Alzheimer disease, which are sporadic. The leading biochemical biomarkers that have advanced most in research include cerebrospinal fluid levels of β-amyloid1–42,51 total tau,52 and phospho-tau (p-tau) proteins.53–55 Decreased levels of β-amyloid1–42 and increased levels of p-tau are currently the most accurate and reproducible chemical biomarkers for early-onset Alzheimer disease.51,53–55 However, they require lumbar puncture, and laboratories for testing these biomarkers are not readily available in Canada. Currently, these cerebrospinal fluid biomarkers may have utility for specialists who seek to distinguish between frontal variants of Alzheimer disease and frontotemporal dementia. When indicated, testing for biomarkers should be performed at a commercial or academic facility with a track record of generating reproducible, high-quality data.
Knowledge gaps
In this article we have alluded to several relevant current gaps in our knowledge. We have stressed the centrality of “clinical assessment,” but we must acknowledge that our clinical definitions have a historical basis rather than an empirical one. For instance, the importance of demonstrating “impaired day-to-day function” in dementia is largely a function of the tendency of psychiatric diagnoses to stress presence or lack of functional impairment. We lack proof that the definition of dementia noted above is superior to alternative ones, or that our definition of cognitive domains is optimal. We do not know exactly how accurate brief cognitive tests are in comparison with one another, or even which method of scoring tests, such as the clock-drawing test, is preferable. For instance, is it better to administer a shorter test (the clock-drawing test) at biannual visits rather than a longer test (the Mini-Mental State Examination) at an initial visit? The ultimate impact of applying different approaches to brief cognitive testing is unknown. It is also unknown exactly how many cases of reversible dementia would be missed in a family practice if structural neuroimaging was not used — the only data have been generated retrospectively in a tertiary care memory clinic.56 Regarding the ancillary tests (neuropsychological testing, functional imaging and measurement of biomarkers), we lack informed large-scale studies with a cost–benefit analysis sufficient to justify their general application. For functional imaging, there is variability across centres, which require requisite expertise for this technology to have diagnostic utility.57,58 Standardization of techniques is necessary for them to have diagnostic utility.
Perhaps more important than any of these knowledge gaps are the large gaps between what we know about diagnosis and what is practised in many family physicians' offices. Less than 25% of cases of Alzheimer disease in Canada are diagnosed and treated,59,60 which implies a lack of application of known diagnostic approaches. The major hurdles to diagnosing dementia in family practice are (a) the complexity of the diagnostic process, (b) physicians' lack of familiarity with cognitive screening, (c) the pressures of time (the diagnostic process requires multiple visits to complete) and (d) the lack of general conviction that an accurate diagnosis of dementia warrants the requisite effort. Physician education is needed to help address these hurdles, and we hope that this article will help to encourage family physicians to undertake the diagnostic process more routinely.
The case revisited
Mrs. E presents with a memory complaint corroborated by her family, along with clear historical evidence of a progressive cognitive decline with collateral information from her husband that her impairment has reached the point of interfering with her social functioning and activities of daily living. Her physician conducts the Mini-Mental State Examination as the objective brief cognitive test, and her score confirms the presence of memory impairment, as evidenced by her impaired learning of test objects and by her temporal disorientation. There is also mild impairment of language (naming). In her daily life, there is evidence of impaired executive functioning (inability to handle banking) and topographic disorientation (getting lost while driving). On this basis, Mrs. E meets the clinical definition of dementia.
The next step is to determine the cause of Mrs. E's dementia. Her physician works through a logical list of exclusions. There is no evidence of delirium. The depressive symptoms and anxiety require more exploration to determine their significance and their relationship to the cognitive impairment. However, from the available information, a confounding major depression or primary anxiety disorder is unlikely to be present. The physician reviews Mrs. E's medications, paying particular attention to the use of any psychoactive medications, including sedative hypnotics, antipsychotics and antidepressants as well as drugs with potential anticholinergic properties. None of these confounding disorders are identified.
In the continued search for the cause of her dementia, the physician notes the patient's history of a transient ischemic attack and considers a potential contributing cerebrovascular component to the dementia. A review of vascular risk factors and examination for signs of stroke would be appropriate. However, although the presence of a transient ischemic attack does bring up cerebrovascular considerations, the overall natural history is not one of stroke-like episodes with step-wise decline, or of a stroke followed within short order by a progressive dementia, as might be the case in a vascular dementia.61,62 On physical examination, Mrs. E's physician finds no focal neurologic signs. From a differential diagnosis standpoint, he finds no parkinsonian features, fluctuations in cognition and alertness, or visual hallucinations to suggest the core features of dementia associated with Parkinson's disease or dementia associated with Lewy bodies.63 Mrs. E has no myoclonus, and her course is not rapidly progressive as would typically be the case with Creutzfeld–Jakob disease.64 The lack of an early and prominent behavioural change with impairment in social conduct, progressive aphasia or motor neuron features puts aside consideration of frontotemporal dementia. The core and supportive features of Alzheimer disease are therefore met, and Mrs. E meets the clinical diagnostic criteria for Alzheimer disease.
Mrs. E's Mini-Mental State Examination score revealed impairment that was at the cut-off point for dementia. Her physician considers administering one of the newer brief cognitive tests, such as the Montréal Cognitive Assessment, the DemTect, the Behavioural Neurology Assessment, the General Practitioner Assessment of Cognition or the 7-Minute Screen (Table 1). These tests would likely demonstrate a greater degree of impairment, reinforcing the degree and significance of the cognitive impairment and its commensurate relationship with dementia. However, he decides not to because there is already considerable evidence of sufficient cognitive impairment (on temporal orientation, short-term recall and naming) and functional impairment (on history) to establish a diagnosis of dementia.
Mrs. E's physician orders a basic laboratory work-up, including a complete blood count and serum levels of calcium, thyroid stimulating hormone, fasting serum glucose and vitamin B12. Beyond the investigations required for dementia diagnosis, her physician reviews her history of transient ischemic attack to ensure that measures for secondary stroke prevention are in place.
Because of Mrs. E's history of transient ischemic attack and lack of prior neuroimaging, her physician will request that she undergo computed tomography or magnetic resonance imaging to rule in cerebrovascular disease. This approach is particularly focused on the patient with cerebrovascular risk factors, clinical stroke or transient ischemic attack episodes. The scans will allow her physician to assess the extent, location and contribution of underlying cerebrovascular disease to her Alzheimer dementia and may guide the intensity of treatment of her vascular risk factors. There is no indication for functional neuroimaging or neuropsychological testing given the strength of the clinical diagnosis. There are no signs of frontotemporal dementia or atypical features to support the use of lumbar puncture for the measurement of β-amyloid1–42 protein, total tau protein and p-tau protein levels.
In summary, Mrs. E was judged on clinical grounds to meet the diagnostic criteria for dementia. Her presentation is most consistent with Alzheimer disease, given the gradual onset of a progressive cognitive decline without any highlighting strokes, stepwise decline or clinical features to suggest an alternative diagnosis. The use of neuropsychological testing would clarify the cause of the dementia; however, in this instance it is not required. The physician schedules a further visit with the family after all the results are back so that he can describe the diagnostic results, give the diagnosis of Alzheimer disease, discuss the prognosis and initiate therapy. These management issues will be addressed in a further article in this series.
Conclusion
The diagnosis of dementia remains clinically integrative based on history, physical examination and cognitive assessment. Brief cognitive testing is indicated for each patient presenting for assessment of dementia. Recommended investigations also include a number of core laboratory tests. Structural neuroimaging with computed tomography or magnetic resonance imaging is advised on a selective basis according to clinical features and the natural history of the presentation.
There are a growing set of promising diagnostic approaches that families of patients will have encountered in the media but that are not yet recommended for routine use by family physicians. Although functional neuroimaging with positron emission tomography or single photon emission computed tomography is evolving rapidly, application of these technologies to the clinical investigation of dementia is still limited. Similarly, although the measurement of biomarkers is not yet ready for widespread use in clinical settings, it is showing promise in the research setting and may change our approach to dementia evaluation in the near future. Neuropsychological testing is powerful but expensive and not readily available to family physicians in Canada. It is not essential in the routine evaluation of dementia patients.
Articles to date in this series
• Chertkow H. Diagnosis and treatment of dementia: Introduction. Introducing a series based on the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia. CMAJ 2008;178: 316-21.
• Patterson C, Feightner JW, Garcia A, et al. Diagnosis and treatment of dementia: 1. Risk assessment and primary prevention of Alzheimer disease. CMAJ 2008;178: 548-56.
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/178/7/825/DC1
This series is based on recommendations from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia.
Series editor: Howard Chertkow MD, Department of Neurology, McGill University and the Bloomfield Centre for Research in Aging, Lady Davis Institute, Sir Mortimer B. Davis–Jewish General Hospital, Montréal, Que.
Editor's Note: The background papers with supporting evidence for the recommendations from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia were published in the October 2007 issue of Alzheimer's and Dementia and are available at www.alzheimersanddementia.org. These articles are also freely available at www.cccdtd.ca (through agreement with Elsevier).
This article has been peer reviewed.
Contributors: All of the authors contributed to the study conception and design, revised the manuscript critically for important intellectual content and approved the final version submitted for publication.
Acknowledgements: We gratefully acknowledge the expert technical assistance of Jacob Grand in developing this paper and Dr. Najeeb Qadi for his help with the references.
Competing interests: None declared for Howard Feldman, Claudia Jacova, Angeles Garcia, Tiffany Chow, Michael Borrie, Mervin Blair or Howard Chertkow. Alain Robillard has been a member of the speaker's board, has served as a consultant to or has given lectures sponsored by Janssen-Ortho, Novartis, Pfizer and Lundbeck; he has received travel assistance to attend scientific meetings by Novartis, Pfizer and Janssen-Ortho; and he is the principal investigator for a number of clinical trials sponsored by the previously named companies as well as Elan Pharmaceuticals, Sanofi Aventis, Voyager Pharmaceutical, SmithKline Beecham and Ono Pharmaceutical. Tiffany Chow has served as a consultant to Janssen-Ortho and has received speaker fees or educational grants from Novartis and Lundbeck. Hyman Schipper has served as a consultant to Osta Biotechnologies, Teva Neurosciences and Caprion Pharmaceuticals; he holds equity in Molecular Biometrics and stock options in Osta Biotechnologies. Andrew Kertesz has served as a consultant and has received honoraria, speaker fees and travel assistance from Pfizer, Janssen-Ortho, Novartis and Lundbeck.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.
- 10.
- 11.
- 12.
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Characterizing personalized neuropathology in dementia and mild cognitive impairment with explainable artificial intelligence
- Roles des medecins de famille dans les soins lies a la demence
- Role of the family physician in dementia care
- Care of community-dwelling older adults with dementia and their caregivers
- Charting age-associated cognitive decline
- Cognitive assessments in multicultural populations using the Rowland Universal Dementia Assessment Scale: a systematic review and meta-analysis
- MRI and cerebrospinal fluid biomarkers for predicting progression to Alzheimer's disease in patients with mild cognitive impairment: a diagnostic accuracy study
- Structured approach to patients with memory difficulties in family practice
- Approche structuree en pratique familiale pour les patients ayant des problemes de memoire
- Behaviour management in dementia
- How applicable are clinical practice guidelines to elderly patients with comorbidities?
- Building capacity for dementia care: Training program to develop primary care memory clinics
- Progressive impairment of cognition and motor function: Hashimoto encephalopathy
- Effectiveness of home treatment for elderly people with depression: randomised controlled trial
- The Rural Older Adult Memory (ROAM) Study: A Practice-based Intervention to Improve Dementia Screening and Diagnosis
- Diagnosis of dementia
- Diagnosis and treatment of dementia: 6. Management of severe Alzheimer disease
- Diagnosis and treatment of dementia: 4. Approach to management of mild to moderate dementia
- Diagnosis and treatment of dementia: 3. Mild cognitive impairment and cognitive impairment without dementia
More in this TOC Section
Similar Articles

