


The case
Mr. S, a 63-year-old man with a recent history of peptic ulcer disease who is taking proton pump inhibitor therapy (his only medication) as an outpatient, is admitted to the intensive care unit (ICU) with respiratory distress. Community-acquired pneumonia is diagnosed, although pulmonary embolism was considered in the differential diagnosis. Treatment with both antibiotics and intravenous heparin is initiated. Over the next 24 hours, the patient’s clinical condition improves, and his care is transferred to the medical teaching unit. Before discharge from the ICU, a computed tomography chest scan with contrast confirms the absence of a pulmonary embolism. On day 4 after admission, hematemesis, hypotension and respiratory distress develop. The patient is intubated, readmitted to the ICU and given 6 units of blood. Endoscopy shows an actively bleeding peptic ulcer. The patient’s intravenous heparin therapy is stopped. Protamine is administered because his partial thromboplastin time is greater than 150 seconds, and a proton pump inhibitor is prescribed.
Why did this medication error occur? What could have been done to prevent this error? How should the medical team proceed?
Medication errors in critical care
Critically ill patients admitted to an ICU experience, on average, 1.7 medical errors each day, and many patients suffer a potentially life-threatening error during their stay. 1,2 Medication errors are the most common type of error and account for 78% of serious medical errors in the ICU. 3 Providing 1 critically ill patient with a single dose of a single medication requires correctly executing 80–200 steps. 4 The medication process involves 5 broad stages: prescription, transcription, preparation, dispensation and administration. 5 Medication errors, defined as any error in the medication process regardless of whether a patient experiences an adverse consequence, can occur at any step. 6 It is important to have an understanding of the risk factors for medication errors and the evidence base for preventing medication errors and disclosure, should an error occur.
Although the medication process is similar for all patients in hospital, we have restricted our review to studies focused on critically ill adult patients because the environment, patient characteristics and medications used in the ICU are substantially different from those in other hospital units. 7 The ICU brings together high-risk patients who require urgent, complex interventions from multiple health care professionals in a complex environment where patients are exposed to twice as many medications as those in general medical wards. 7,8 In addition, critically ill patients differ from most other hospital patients because they have limited ability to participate in their medical care and lack the physiologic reserve to tolerate additional injury.
Methods
Our search strategy (Appendix 1, available at www.cmaj.ca/cgi/content/full/180/9/936/DC1) resulted in the identification of 1168 citations: 870 from MEDLINE, 262 from EMBASE and 36 from Evidence-Based Medicine Reviews. Of these, 57 full-text articles met our initial inclusion criteria and were retrieved for assessment (Appendix 2, available at www.cmaj.ca/cgi/content/full/180/9/936/DC1). An additional 5 articles were selected from the reference lists of the retrieved articles. After assessment, 17 articles 3,7,9–23 remained for review. These articles were published between 1950 and 2008. We extracted key elements from the selected studies, including study design, study population, recruitment and sampling, blinding, attrition rates and statistical methods (Appendix 3, available at www.cmaj.ca/cgi/content/full/180/9/936/DC1).
What is the incidence of medication errors in the intensive care unit and what are the risk factors?
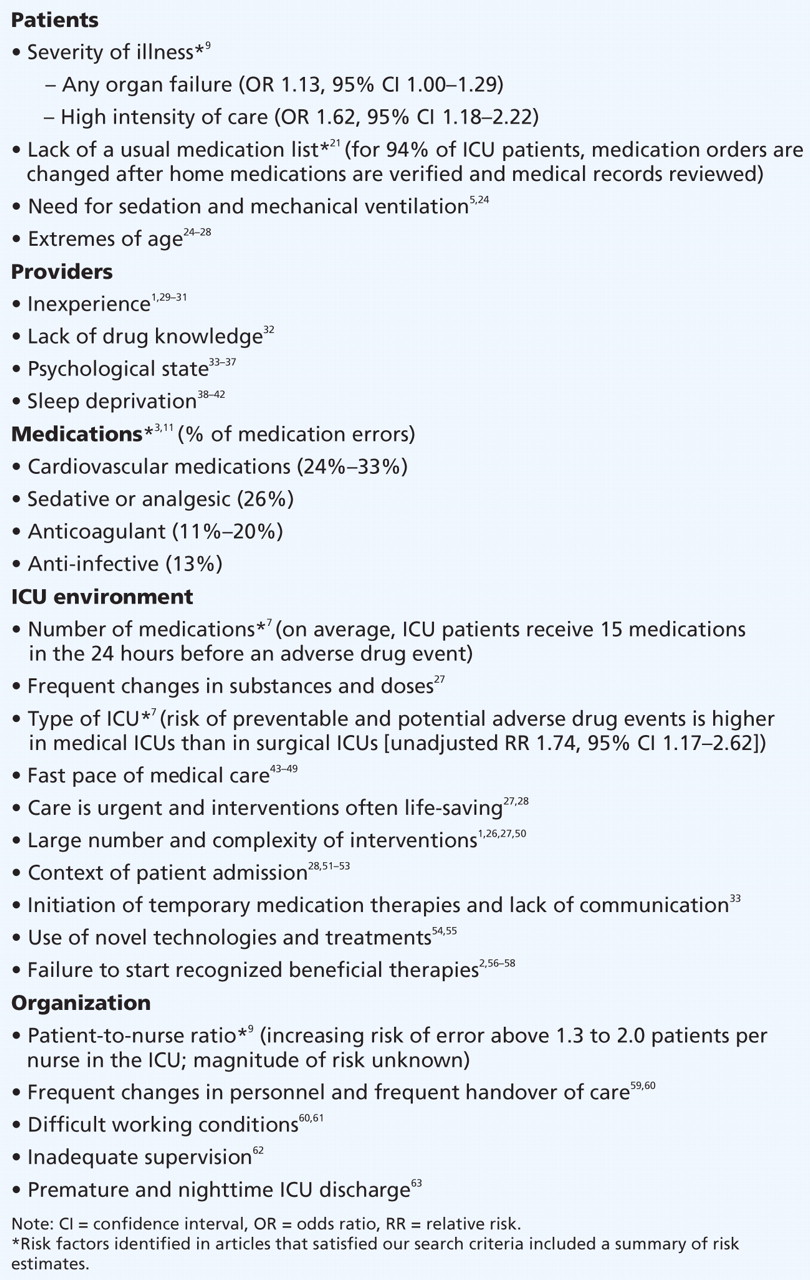
From 49 of the articles retrieved in our search, we identified and categorized potential risk factors for medication errors in the ICU (Box 1). Only 6 of these studies satisfied our inclusion criteria. The first used a survey of nurses and physicians to examine the point prevalence of sentinel events and their risk factors in 205 ICUs in 29 countries. 9 Medication errors were the second most frequent sentinel event, with a point prevalence of 10.5 medication errors per 100 patient-days. The frequency of medication errors was similar during the prescription (54%) and administration (46%) phases of the medication process. Multiple variable logistic regression analysis revealed that the patient-to-nurse ratio in the ICU (range 1.3:1 to 2:1), exposure time to medications, organ failure and the high level of care provided to each patient were independent risk factors for sentinel events including medication errors.
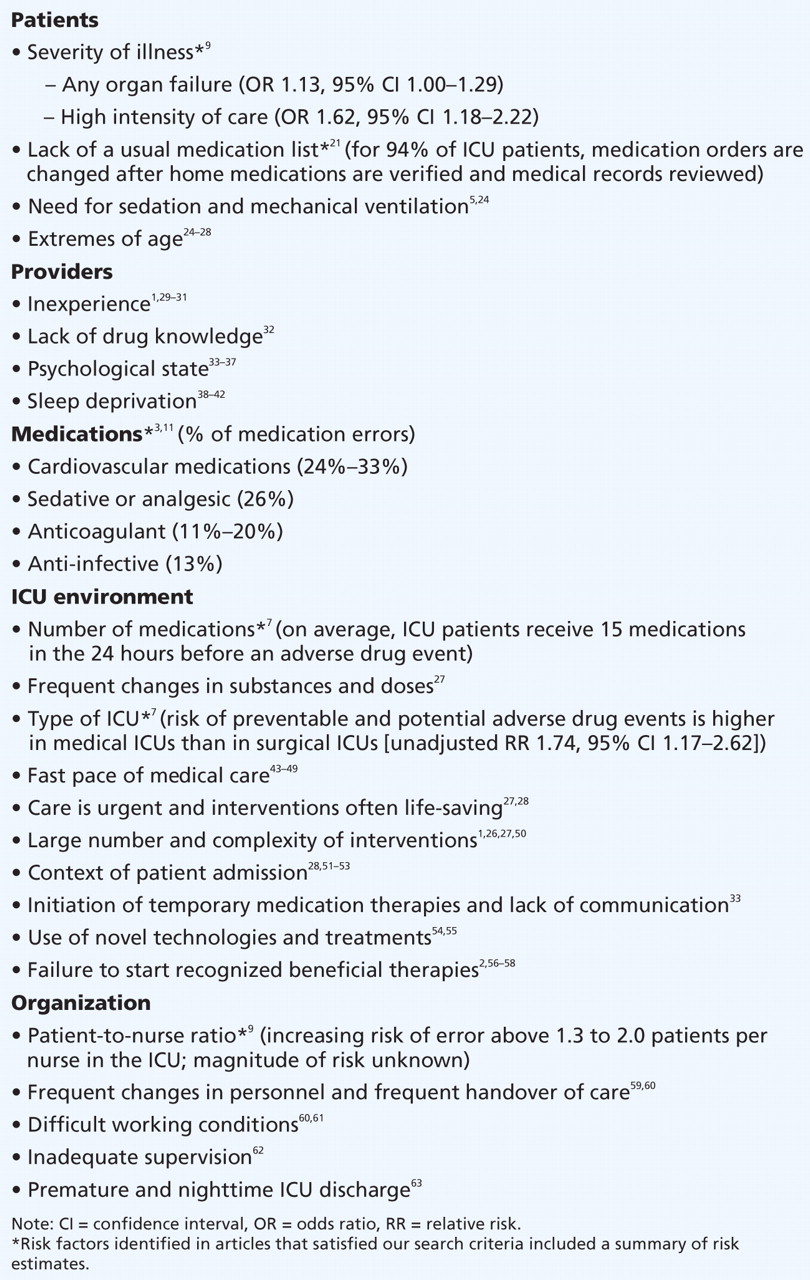
Box 1: Potential risk factors for medication errors in the intensive care unit (ICU)
The second was a prospective cohort study of 4031 medical and surgical patients admitted to 5 ICUs and 6 general care units over 6 months. 7 Adverse drug events and medication errors were identified by direct reporting, investigator visits to each care unit and chart review. In this study, 2 physician reviewers independently evaluated all potential adverse drug events, and structured interviews were performed to determine the circumstances of the adverse event. The number of preventable and potential adverse drug events per 1000 patient-days was higher in ICUs than in general care units (19 v. 10, p < 0.01), but the number was similar after adjustment for the number of medications prescribed (1.27 v. 1.07 per 1000 patient-days per prescribed medication). The rate of preventable and potential adverse drug events was higher in medical ICUs (25 per 1000 patient-days) than in surgical ICUs (14 per 1000 patient-days) (p < 0.05) with similar numbers of medications prescribed in both types of ICU. A similar finding was reported in the third article, a multicentre prospective trial of safety incidents. 10 This study reported that medication errors were more frequent in medical ICUs than in surgical ICUs (13% v. 6%; p ≤ 0.001). 10 Cullen and colleagues 7 also found that most medication errors occurred during either the administration (44%) or ordering (38%) phase of the medication process. Interviews suggested that most errors occurred during what caregivers perceived as normal working conditions.
The study by Calabrese and colleagues 11 reported medication errors in a cohort of 851 patients admitted to 5 ICUs over 3 months. Pharmacists prospectively monitored each patient twice daily using direct observation and review of the administered medications. Medication errors were identified during 187 of the 5744 observations (3.3%). The most frequently reported errors were wrong infusion rate (40.1%), dose omission (14.4%), improper dose (11.7%) and wrong time (13.9%). The authors identified vasoactive medications (32.6%) and sedatives or analgesics (25.7%) as the medication classes most commonly associated with error.
In the fifth study, 12 pharmacists directly observed the preparation and administration process for 2009 prescriptions filled by nurses. They identified errors in 6.6% of the observations and characterized the most frequent errors as errors in the dose, wrong rate, wrong preparation technique, physico-chemical incompatibility, wrong administration technique and wrong time.
The Critical Care Safety Study, performed by Rothschild and colleagues 3 as part the Harvard Work Hours and Health Study, 13 was a 1-year prospective observational study with multifaceted determination of adverse events, including adverse drug events, in a medical ICU and a coronary care unit of a tertiary care hospital. The authors reported a similar medication error rate in both units (ICU 127.8 errors per 1000 patient-days; coronary care unit 131.5 errors per 1000 patient-days, p = 0.12). Medication errors were most commonly associated with treatment, but errors were also found in prevention (e.g., prophylaxis), diagnosis (e.g., intravenous contrast agents) and monitoring (e.g., glycemic monitoring and insulin therapy). The most common medication errors were ordering or administering the wrong dose. Medication classes most frequently associated with errors were cardiovascular drugs (24%), anticoagulants (20%) and anti-infective agents (13%).
Our review of the literature highlighted 2 important findings. First, medication error rates vary widely among clinical settings (both ICU and non-ICU settings), patient populations and studies. The reasons for this variation are likely multifactorial, but the reasons may include different patient populations (illness severity, number and type of prescriptions) clinical practice variation, lack of uniformity of definitions, the processes under investigation (e.g., prescription, transcription), methods of reporting and the culture of the different centres reporting their data. 2,25,64,65 The lack of standard definitions and reporting techniques make comparisons across organizations, regions or countries difficult. 2 The single multicountry study included in our analysis did not report medication error rates across different countries. 9
Second, although there are many potential risk factors for medication errors (Box 1), the strongest evidence that critically ill patients are at increased risk of a medication error are increased severity of illness; failure to document the patient’s usual medication list; prescription of cardiovascular, sedative, analgesic, anticoagulant or anti-infective medications; prescription of each additional medication; admission to a medical ICU compared with a surgical ICU; and more critically ill patients per nurse (increasing risk above 1.3 to 2.0 patients per nurse in the ICU).
What strategies can be used to prevent medication errors in intensive care units?
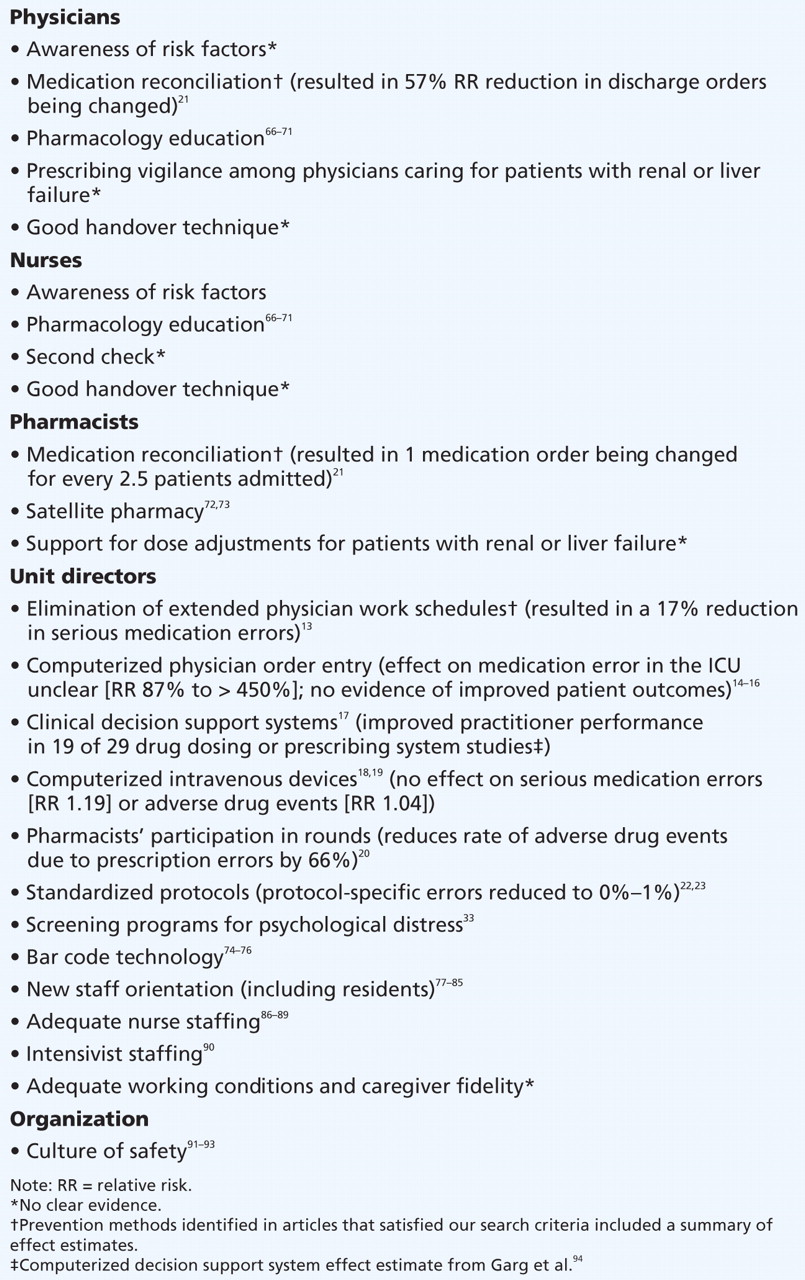
From the 31 articles identified in our search, we identified potential strategies to prevent medication errors in the ICU (Box 2). Of these, 11 studies satisfied our inclusion criteria. These studies reported 7 prevention strategies: eliminating extended physician work schedules (n = 1), computerizing physician order entry (n = 3), implementing support systems for clinical decisions (n = 1), computerizing intravenous devices (n = 2), having pharmacists participate in the ICU (n = 1), reconciling medications (n = 1) and standardizing medications (n = 2).

Box 2: Strategies for preventing medication errors in the intensive care unit (ICU)
Physician work schedules
A single randomized nonblinded study compared the rates of medication errors made by interns working a traditional clinical schedule with those made when extended work shifts were eliminated and the number of consecutive hours of work was limited to about 16. 13 Interns in the traditional clinical schedule worked a mean 77–81 hours a week compared with 60–63 hours a week for the intervention group. Compared with interns working a traditional clinical schedule, those in the intervention group made 17.3% fewer serious medication errors (82.5 errors v. 99.7 errors per 1000 patient-days, p = 0.03). Serious medication errors were similarly reduced unit-wide among all clinicians during the intervention schedule (115.5 errors v. 135.2 errors per 1000 patient-days, p = 0.03).
Computerized physician order entry
We found 3 studies on computerized physician order entry and medication error in the ICU. Computerized physician order entry is the main component of a clinical information system that allows physicians to enter orders directly into a computer for electronic processing, potential recommendations about dosing, and checking for duplication and drug–drug interactions. 95 Computerized physician order entry targets the prescription and transcription stages of the medication process.
Shulman and colleagues 14 reported the rate of medication errors before and after institution of computerized physician order entry without decision support in their 22-bed multisystem ICU. A pharmacist prospectively identified medication errors during prescription review over 26 days of data collection. Following the introduction of computerized physician order entry, the proportion of prescriptions with errors decreased from 6.7% to 4.8% (p < 0.04). A second study by Colpaert and coworkers 15 prospectively compared prescription errors in 2 surgical ICUs, 1 using paper-based prescriptions and 1 using computerized physician order entry. The number of prescription errors was significantly lower in the ICU that used computerized entry (3.4% v. 27%, p < 0.001). Finally, Weant and colleagues 16 identified voluntarily reported medication errors before and after the implementation of computerized physician order entry in a neurosurgical ICU. Following implementation of computerized entry, there was an increase in the number of medication errors but a decrease in the number of errors resulting in patient harm. According to 2 recent systematic reviews 96,97 of studies of predominantly non-ICU inpatients, the weight of evidence is that computerized physician order entry systems decrease medication errors, but they do not improve patient outcomes.
Clinical decision support systems
Clinical decision support systems can be used with computerized physician order entry; they include any knowledge-based tool integrated into clinician workflow and patient data to improve quality of care. 98 We identified 1 study 17 of clinical decision support systems and medication error in the ICU, which compared the safety of anti-infective prescription before and after implementation of such a system in a 12-bed ICU. The authors reported that physicians prescribed the medication suggested by the computer for 46% of the orders and the dose and interval suggested by the computer for 93%. The clinical decision support system, which was linked with computerized medical records, was able to decrease prescription of medications to which patients had reported allergies from 146 to 35 (p < 0.01), excess dose errors from 405 to 87 (p < 0.01) and antibiotic-susceptibility mismatches from 206 to 12 (p < 0.01). The number of reported adverse drug events following implementation decreased from 28 to 4 (p < 0.02). A systematic review of computerized decision support systems in predominantly non-ICU inpatients suggests that, although these systems may reduce error, they may not improve patient outcomes. 94
Computerized intravenous devices
Computerized intravenous devices, or “smart pumps,” incorporate point-of-care decision support into standard intravenous delivery systems. The bedside clinician selects a medication from a predetermined medication library and is guided through the selection of dose units (e.g., μg/kg per minute or units/hour) and dose limits. Device safeguards include alerts for duplicate medication entry (medication already infusing on another channel) and dose safety limits. We identified 2 studies of computerized infusion pumps in the ICU. 18,19 In the first, Rothschild and colleagues 18 performed a nonblinded, prospective time series analysis that compared real-time decision support by smart pumps with no decision support in 2 cardiac surgery ICUs and 2 cardiac surgery intermediate care units. The rates of serious medication error did not differ between the intervention and control periods (2.41 v. 2.03 errors per 100 patient–pump-days, p = 0.124). In the second study, Nuckols and coworkers 19 retrospectively reviewed the medical records of ICU patients in 2 hospitals before and after their conventional pumps were replaced with smart pumps. The rate of adverse intravenous drug events was similar for the 2 periods (4.78 v. 4.95 per 1000 patient-days, p = 0.96).
Pharmacist participation in the intensive care unit
We identified 1 study 20 that reported the effects of pharmacist participation in the ICU. Adverse drug events in a medical ICU were compared before and after pharmacist participation in rounds. A coronary care unit with no pharmacist was used as a control. The rate of adverse drug events secondary to prescription errors decreased by 66%, from 10.4 adverse drug events per 1000 patient-days before the intervention to 3.5 per 1000 patient-days after (p < 0.001). No change in adverse drug events secondary to prescription errors was observed in the control unit (10.9 v. 12.4 errors per 1000 patient-days, p = 0.76). During the 9-month study period, 99% of the pharmacists’ recommendations were accepted by the attending physicians. Guideline statements from both the Society of Critical Care Medicine and the American College of Clinical Pharmacy recommend that pharmacists regularly participate in rounds as members of the multidisciplinary critical care team to provide pharmacotherapeutic advice. 99
Medication reconciliation
We identified 1 study 21 that described the use of a pre–ICU-discharge survey to compare discharge medication orders with the patient’s medical record. The aim was to identify whether discharge medications were the same as the patient’s regular medications and to verify the accuracy of documented allergies. According to Pronovost and colleagues, 21 the routine use of this discharge survey prevented an average of 10 medication errors per week in the 14-bed surgical ICU.
Medication standardization
We found 2 studies 22,23 of medication standardization in the ICU. Wasserfallen and colleagues 22 compared compliance with American Society of Health-System Pharmacists’ criteria 100 for prescription safety in a surgical ICU before and after implementation of a formatted order sheet. A medical ICU served as a control: physicians continued to use the usual medical order sheet but were briefed on the importance of prescribing in a correct format at the beginning of each new rotation period. The proportion of safe orders increased in both the surgical ICU (74% v. 48%, p < 0.001) and the medical ICU (74% v. 66%, p < 0.001) during the study. In the second study, McMullin and coworkers 23 prospectively examined implementation of a standardized protocol for treatment of venous thromboprophylaxis to decrease errors of omission in a medical–surgical ICU. They used 5 behaviour-change strategies as part of their thromboprophylaxis safety intervention: interactive education, verbal and written prompts, computer prompts, individual performance feedback and public displays of group performance. Heparin prophylaxis increased from 60% in the baseline period, to 90% in the study period and 100% in the follow-up period (p = 0.01).
Other prevention strategies
We found no studies of the prevention of medication errors in critical care with various models of intensivist staffing, nurse staffing, bar code technologies, simulation, cultures of patient safety or medication reporting that satisfied our inclusion criteria. Although these strategies may be intuitive, supported by evidence in other settings or industries and even conceptually simple, further study is warranted to determine whether they prevent medication errors among critically ill patients.
What can clinicians do right now to prevent medication errors?
The quality of most studies that met our inclusion criteria was low, highlighting the fact that most interventions to prevent medication errors are not supported by high-quality evidence and that important gaps exist in the literature. Thus, a practical approach is to recognize that errors are a reality of medicine and that all health care providers have a responsibility to ensure patient safety and to use caution in promoting what are seemingly intuitive interventions. Improved medication safety may be accomplished by optimizing the safety of the medication process, eliminating situational risk factors and adopting strategies to intercept errors and mitigate their consequences. Among the 7 prevention strategies identified in articles that met our inclusion criteria, 3 can be immediately implemented by clinicians.
Medication reconciliation
As many as 50% of all medication errors occur on admission to or discharge from the ICU, and about 60% of regularly scheduled medications are stopped on ICU admission. 21,101,102 Maintaining an up-to-date patient-medication list that includes long-standing medications, reasons why new medications were initiated and planned stop dates, and reasons why old medications were stopped or held may improve patient safety.
Pharmacist participation
Engaging the resources and skills of pharmacists, particularly with regard to patients with multiple risk factors or altered pharmacokinetics, is likely to improve the quality of care delivered.
Medication standardization
Many ICUs have developed protocols to facilitate the management of common important issues (e.g., prophylaxis for venous thromboembolism). Ensuring adherence to protocol for appropriate patients should improve safety.
What should the approach be once an error has occurred?
No studies about the disclosure of medication errors in critically ill patients met our inclusion criteria. However, our literature search identified articles which suggested that patients want full disclosure of harmful errors and that disclosure of medical errors is increasingly recognized as an ethical imperative. 103 Nonetheless, surveys show that only 17%–30% of physicians inform their patients when they experience a medical error. 103–105 Disclosure should take place whenever a patient has suffered an iatrogenic injury and should be guided by the following principles:
-
Perform in a timely fashion — as soon as possible after the injury, while ensuring the patient’s well-being.
-
Perform in a quiet room free of interruptions.
-
Disclose facts without speculation, opinion or blame.
-
Use simple, unambiguous lay words.
-
Include an expression of sympathy.
-
Allow time for questions.
-
Document disclosure in the medical record.
Resolution of the case
Our case highlights the risks of medication error and the potentially serious consequences in critical care. First, our patient was prescribed heparin, a medication reported to be associated with increased risk of medication error. 3 Second, medication reconciliation was not carried out when the patient’s proton pump inhibitor was discontinued on admission. Third, transition of the patient’s care from the ICU to the medical teaching unit provided an opportunity for the temporary administration of heparin to continue unnecessarily. Finally, either the dose of heparin or failure to monitor the patient’s condition resulted in a supratherapeutic level, shown by a partial thromboplastin time of greater than 150 seconds. The medication error was disclosed to the patient’s family. There was no further evidence of bleeding, and the patient was moved back to the medical teaching unit after 48 hours.
In this case, potential prevention strategies could have included the following. First, educating physicians about the risk factors for medication errors might have prevented prescription of heparin in a questionable risk–benefit scenario. Second, a structured medication reconciliation process on ICU discharge (e.g., re-prescribe all regular medications), such as the strategy proposed by Pronovost and colleagues, 21 might have resulted in restarting the proton-pump inhibitor. Third, a standardized process for transition of care (e.g., verbal communication, written communication, dictated transfer note) that ensures that important information on active diagnoses and important investigations and interventions are transmitted and recorded may have resulted in evaluation of the computed tomography scan result and discontinuation of heparin.
Conclusion
Given the large body of literature about patient safety, 106 the limited evidence available to guide clinicians in selecting strategies to prevent and disclose medication errors in critically ill patients is surprising. Nevertheless, patient safety is a first step in providing high-quality health care, and ensuring the safety of patients is everyone’s responsibility and challenge.
-
Medication reconciliation may improve patient safety in the intensive care unit, and an updated list of medications should be maintained, including long-standing medications, the reasons for starting new medications and their planned stop dates and the reasons for discontinuing or holding old medications.
-
Engaging pharmacists in inpatient rounds in the intensive care unit may decrease the risk of adverse drug events.
Key points
Recommended reading
-
Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA 1997;277:307–11.
-
Cullen DJ, Sweitzer BJ, Bates DW, et al. Preventable adverse drug events in hospitalized patients: a comparative study of intensive care and general care units. Crit Care Med 1997;25:1289–97.
-
Gallagher TH, Waterman AD, Ebers AG, et al. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA 2003;289:1001–7.
-
Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med 2004;351:1838–48.
-
Leape LL, Bates DW, Cullen DJ, et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA 1995;274:35–43.
-
Leape LL, Cullen DJ, Clapp MD, et al. Pharmacist participation on physician rounds and adverse drug events in the intensive care unit. JAMA 1999;282:267–70.
-
Pronovost PJ, Angus DC, Dorman T, et al. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA 2002;288:2151–62.
-
Rothschild JM, Landrigan CP, Cronin JW, et al. The Critical Care Safety Study: the incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med 2005;33:1694–700.
-
Sittig DF, Stead WW. Computer-based physician order entry: the state of the art. J Am Med Inform Assoc 1994;1:108–23.
-
Volpp KG, Grande D. Residents’ suggestions for reducing errors in teaching hospitals. N Engl J Med 2003;348:851–5.
Footnotes
-
An abridged version of this article appeared in the Apr. 28, 2009, issue of CMAJ and is available online at www.cmaj.ca/cgi/content/full/180/9/936/DC2
This article has been peer reviewed.
Competing interests: None declared.
Contributors: Henry Thomas Stelfox was responsible for the conception and design of the study, the analysis and interpretation of the data, and the revision of the manuscript. Eric Camiré and Eric Moyen were responsible for design of the study, the acquisition, analysis and interpretation of data, and the drafting and revision of the manuscript. All of the authors approved the final version of the manuscript submitted for publication.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.
- 25.↵
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.↵
- 65.↵
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.
- 105.↵
- 106.↵
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
- Article
- The case
- Medication errors in critical care
- Methods
- What is the incidence of medication errors in the intensive care unit and what are the risk factors?
- What strategies can be used to prevent medication errors in intensive care units?
- What can clinicians do right now to prevent medication errors?
- What should the approach be once an error has occurred?
- Resolution of the case
- Conclusion
- Recommended reading
- Footnotes
- REFERENCES
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- Evaluation of medication risk at the transition of care: a cross-sectional study of patients from the ICU to the non-ICU setting
- Dosing of enteral acetaminophen in critically ill children: a cohort study
- Patient, family and provider experiences with transfers from intensive care unit to hospital ward: a multicentre qualitative study
- Protocol to describe the analysis of text-based communication in medical records for patients discharged from intensive care to hospital ward
- Prospective cohort study protocol to describe the transfer of patients from intensive care units to hospital wards
- Pharmacist-led medication review in an acute admissions unit: a systematic procedure description
- Development of an orthopedic surgery trauma patient handover checklist
- Medication Errors in the Intensive Care Unit: Literature Review Using the SEIPS Model
- Use of simulation to assess electronic health record safety in the intensive care unit: a pilot study
- A Second Set of Eyes: An Introduction to Tele-ICU
More in this TOC Section
Similar Articles

