


Asthma is one of the most common chronic conditions affecting both children and adults, yet much remains to be learned of its etiology. This paper evolved from the extensive literature review undertaken as part of a proposal for a longitudinal birth cohort study to examine risk factors for the development of allergy and asthma in early childhood.
Although genetic predisposition is clearly evident, gene-by-environment interaction probably explains much of the international variation in prevalence rates for allergy and asthma. Environmental factors such as infections and exposure to endotoxins may be protective or may act as risk factors, depending in part on the timing of exposure in infancy and childhood. Some prenatal risk factors, including maternal smoking, have been firmly established, but diet and nutrition, stress, use of antibiotics and mode of delivery may also affect the early development of allergy and asthma. Later in childhood, putative risk factors include exposure to allergens, breastfeeding (which may initially protect and then increase the risk of sensitization), family size and structure, and sex and gender. In adulthood, recurrence of childhood asthma may be just as common as new-onset asthma, which may have an occupational basis. A better understanding of these risk factors may eventually lead to opportunities for primary prevention of asthma.
Methods
This paper arose from an extensive literature review undertaken in developing the Canadian Healthy Infant Longitudinal Development (CHILD) study, a multicentre national observational study that is currently in progress. The study, which will eventually recruit 5000 pregnant women, has the aim of determining the environmental, host, genetic and psychosocial risk factors for development of allergy and asthma in children. Although not a systematic review, the examination of epidemiologic risk factors in the development of asthma presented here began in 2004 with a search of MEDLINE, using the Medical Subject Heading (MeSH) terms “asthma,” “longitudinal” and “cohort study.” One of us (P.S.) reviewed the abstracts of all studies identified in the search, excluding those without at least one objective outcome measure and those in which the primary outcome measure was not asthma. Studies examining the same outcome measure were tabulated but not combined, since most did not consider exactly the same outcome at the same age. We then performed specific searches to fill gaps in the information gathered via the original search, specifically nutrition, sex and gender effects, and novel environmental exposures. The review was updated in July 2008.
Although the present article includes some references to adult asthma, its primary focus is the epidemiology of and risk factors for this condition in children. A more extensive summary of the literature review for the Canadian Healthy Infant Longitudinal Development study has been published elsewhere. 1
Epidemiology of asthma: an overview
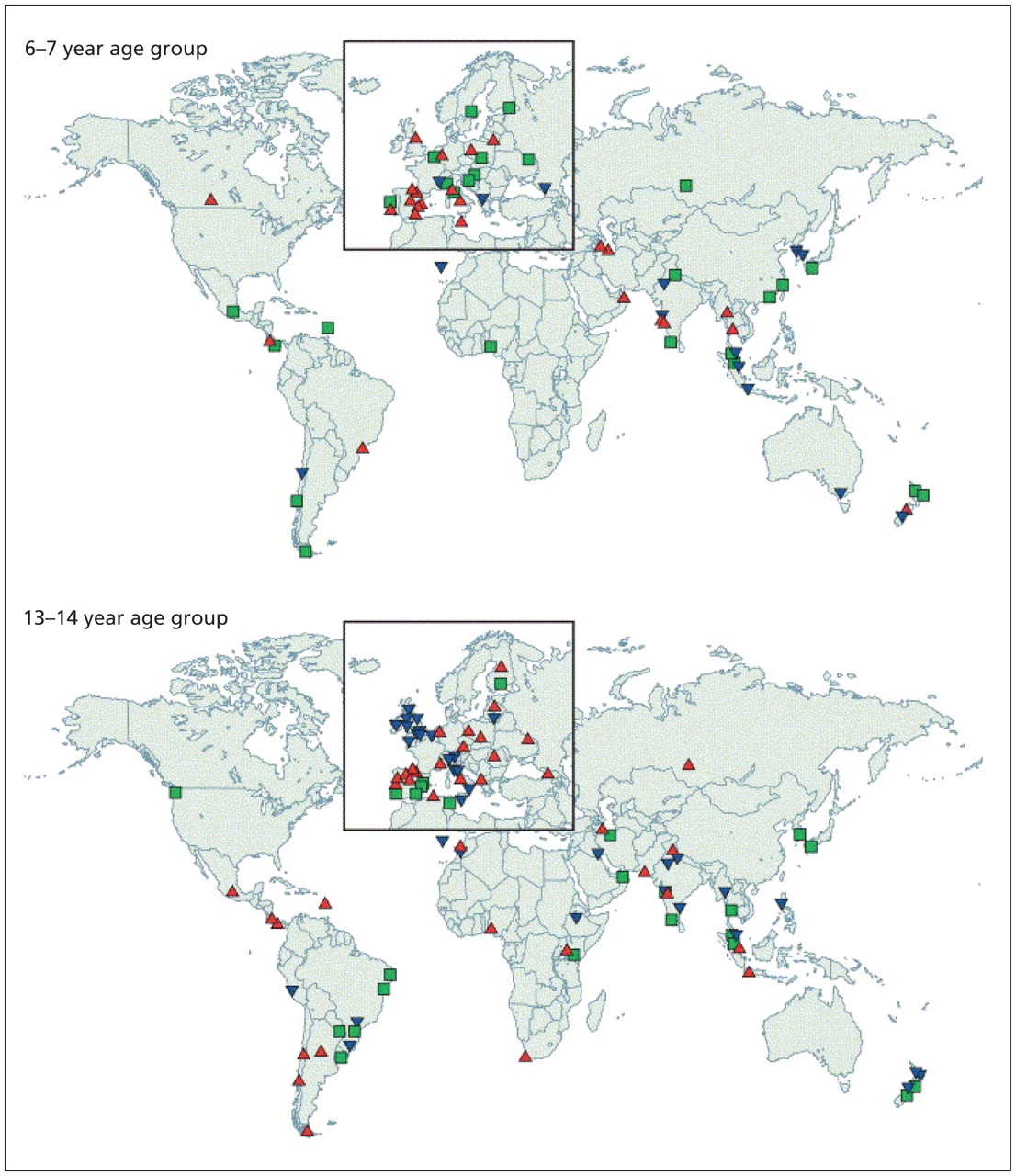
The recent substantial increase in the reported prevalence of asthma worldwide (Figure 1) has led to numerous studies of the prevalence and characteristics of this condition. 2 Foremost among these are 2 major international initiatives that have collected data using validated questionnaires, one among children, the International Study of Asthma and Allergies in Childhood, 3 and the other among young adults, the European Community Respiratory Health Survey. 4 Follow-up investigations for both of these studies 5,6 have examined temporal trends within and across populations. During a mean of 7 years following phase I of the International Study of Asthma and Allergies in Childhood, which in most participating countries was conducted between 1991 and 1993, the prevalence of asthma was stable or decreased in some areas of the world but increased substantially in many other areas, especially among children 13–14 years of age (Figure 2). 5

Figure 1: Changes in prevalence of diagnosed asthma (A) and asthma symptoms (B) over time among children and young adults. Reproduced, with permission, from Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med 2006;355:2226–35. Copyright 2006 Massachusetts Medical Society. 2

Figure 2: Annual changes in worldwide prevalence of asthma symptoms among children 6–7 years old and 13–14 years old, over a mean of 7 years following phase I of the International Study of Asthma and Allergies in Childhood (which in most participating countries was conducted between 1991 and 1993). Blue triangles identify locations where prevalence was reduced by at least 1 standard error (SE) per year, green squares identify locations where there was little change in prevalence (i.e., change of less than 1 SE per year) and red triangles identify locations where prevalence increased by at least 1 SE per year. Reproduced from The Lancet, Vol. 368, Asher MI, Montefort S, Bjorksten B, et al.; ISAAC Phase Three Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. page 733–page 43, copyright 2006, with permission from Elsevier. 5
Cross-sectional population-based studies such as these are highly dependent on recognition of symptoms, so they do not necessarily reflect the true heterogeneity of asthma. However, a wide variation in prevalence rates has been documented: studies of both children and adults have revealed low prevalence rates (2%–4%) in Asian countries (especially China and India) and high rates (15%–20%) in the United Kingdom, Canada, Australia, New Zealand and other developed countries. 3–6
Observations of migrating populations 7 and of Germany after reunification 8 have strongly supported the role of local environmental factors, including allergens but likely many lifestyle factors as well, in determining the degree of expression of asthma within genetically similar populations. A recent analysis of data from the International Study of Asthma and Allergies in Childhood, comparing data from Vancouver, Canada, with data from centres in China, showed significant differences in prevalence rates between children of similar genetic ancestry living in different environments, with evidence for an effect of duration of residence in the new environment. 9 Prevalence rates for asthma among children 13–14 years old were lowest for Chinese children born and studied in China, intermediate for Chinese children who had migrated during their lifetime to Canada and highest for Chinese children who had been born in Canada. In addition, the prevalence rate for the third of these groups was still lower than among non-Chinese children in the same environment. Together, these results strongly suggested gene-by-environment interactions.
Local and national studies have also provided insights into the epidemiology of exacerbations of asthma. For example, epidemics of asthma exacerbations in Barcelona, Spain, were eventually linked to exposure to atmospheric soybean dust released during cargo handling at the local port. 10 The highly predictable annual epidemic of asthma exacerbations in school-age children in the northern hemisphere every September, peaking some 17 days after the return to school, appears to be predominantly driven by seasonal rhinovirus infection, probably compounded by other risk factors for asthma exacerbations, including reduction in use of asthma controller therapy over the summer months, exposure to seasonal allergens and possibly the stress of returning to school. 11,12
Complementing these cross-sectional studies are longitudinal epidemiologic studies in a variety of populations and countries, which have allowed examination of risk factors predicting the development, persistence, remission or relapse of childhood asthma. One such population-based birth cohort study in Dunedin, New Zealand, which had a high retention rate, examined outcomes of childhood asthma at age 26 years. 13 Female sex, airway hyperresponsiveness in mid and later childhood, and sensitization to house dust mites were all significantly and independently related to the likelihood of persistence of childhood asthma to early adulthood. Early age of onset of wheezing symptoms was predictive of relapse after remission, as were airway hyperresponsiveness and allergy to house dust mites. That study and others have clearly demonstrated the tracking of characteristics of asthma from childhood to adulthood, including severity and impairment of lung function.
Etiology of and risk factors for asthma
Asthma comprises a range of heterogeneous phenotypes that differ in presentation, etiology and pathophysiology. The risk factors for each recognized phenotype of asthma include genetic, environmental and host factors. Although a family history of asthma is common, it is neither sufficient nor necessary for the development of asthma. 14
The substantial increases in the incidence of asthma over the past few decades and the geographic variation in both base prevalence rates and the magnitude of the increases support the thesis that environmental changes play a large role in the current asthma epidemic. Furthermore, environmental triggers may affect asthma differently at different times of a person’s life, and the relevant risk factors may change over time.
Short-term studies of risk factors may suggest a lower likelihood of asthma, whereas the same factors may be associated with greater risk if follow-up is more prolonged. This pattern may relate to overlap between different wheezing phenotypes in early childhood, only some of which persist as asthma in later childhood and adulthood. Because of this phenomenon, we examine here the risk factors for persistent asthma at different ages, specifically the prenatal period, infancy, childhood and, briefly, adulthood.
Genetics
Family and twin studies have indicated that genetics plays an important role in the development of asthma and allergy, 15 likely through several genes of moderate effect (i.e., genes associated with relative risks in the range of 1.2–2). 16,17
Genome-wide linkage studies and case–control studies have identified 18 genomic regions and more than 100 genes associated with allergy and asthma in 11 different populations. In particular, there are consistently replicated regions on the long arms of chromosomes 2, 5, 6, 12 and 13. Association studies of unrelated individuals have also identified more than 100 genes associated with allergy and asthma, 79 of which have been replicated in at least one further study. 18 A recent genome-wide association study 19 identified a new gene, ORMDL3, that exhibited a highly significantly association with asthma (p < 10−12) (for single nucleotide polymorphism rs8067378, odds ratio 1.84, 95% confidence interval 1.43–2.42) a finding that has now been replicated in several populations. 20,21
Extensive heterogeneity in the genetic basis of asthma, and in gene-by-environment interactions, is likely. Failure to identify and precisely quantify environmental exposures and their timing may account for some of the difficulty that researchers have had in replicating genetic associations.
Prenatal risk factors
Risk factors in the prenatal period are multifactorial. Assessment is complicated by the variety of wheezing conditions that may occur in infancy and childhood, only some of which evolve to classical asthma.
Prenatal tobacco smoke
Prenatal maternal smoking has been consistently associated with early childhood wheezing, 22–25 and there is a dose–response relation between exposure and decreased airway calibre in early life. 26,27 Prenatal maternal smoking is also associated with increased risks of food allergy, 24 cytokine responses in the cord blood 28,29 and concentrations of nitric oxide in exhaled air in newborns. 30 Studies have shown a clear prenatal effect of smoking; this effect is increased when combined with postnatal smoke exposure.
Diet and nutrition
Observational studies examining prenatal nutrient levels or dietary interventions and the subsequent development of atopic disease have focused on foods with anti-inflammatory properties (e.g., omega-3 fatty acids) and antioxidants such as vitamin E and zinc. Several studies have demonstrated that higher intake of fish or fish oil during pregnancy is associated with lower risk of atopic disease (specifically eczema and atopic wheeze) up to age 6 years. 31–33 Similarly, higher prenatal vitamin E and zinc levels have been associated with lower risk of development of wheeze up to age 5 years. 34–36 However, no protective effect against the development of atopic disease in infants has been shown for maternal diets that excluded certain foods (e.g., cow’s milk, eggs) during pregnancy. 37–40 The authors of 2 recent studies 41,42 reported an inverse relation of maternal vitamin D levels with wheeze in early life, but no relation with atopy or symptoms in later life.
Stress
A number of animal models have suggested that prenatal maternal stress acts through regulation of the offspring’s hypothalamic–pituitary–adrenal axis to decrease cortisol levels, which may affect the development of an allergic phenotype. Although there is a correlation between caregiver stress early in the infant’s life and higher levels of immunoglobulin E in the infant 43–45 and early wheezing, 46 no studies to date have shown an association with asthma. 47,48
Antibiotic use
The association between prenatal antibiotic treatment and subsequent development of atopic disease has been examined in 2 ways: with treatment as a dichotomous predictor (i.e., any antibiotic use) and by number of courses of antibiotics during pregnancy. Longitudinal cohort studies examining any antibiotic use showed a greater risk of persistent wheeze and asthma in early childhood 49,50 and a dose–response relation between number of antibiotic courses and risk of wheeze or asthma. 49,51
Mode of delivery
Development of atopy was 2 to 3 times more likely among infants delivered by emergency cesarean section, 29,52–56 although no such association occurred with elective cesarean section. 29,52,53,56–59 Potential reasons for these findings include maternal stress and differences in the infant’s gut microflora associated with different modes of delivery.
Risk factors in childhood
Phenotypes of asthma
Although some 50% of preschool children have wheezing, only 10%–15% have a diagnosis of “true” asthma by the time they reach school age. 13,60 Commonly described phenotypes in early infancy and childhood are transient wheezing, nonatopic wheezing, late-onset wheezing and persistent wheezing. 61 Only transient wheezing in early infancy has been well characterized, with decreased airflow rates on pulmonary function testing at birth, 56,60,62 onset of wheezing within the first year and resolution by mid-childhood with no lasting effects on pulmonary function.
The other 3 phenotypes have been described primarily by age of onset in cohort studies, and their genesis in early infancy is largely unknown. The majority of children with persistent wheezing (in whom asthma will subsequently be diagnosed) experience their first symptoms before age 3. By 3 years, they have abnormal lung function that persists to adulthood, 13,60,61 and by adolescence, most have atopy. Of children with nonatopic and late-onset wheezing, some experience remission, whereas others experience persistent symptoms and atopy. 63
Distinguishing among these different phenotypes in early childhood is critical to understanding the role of risk factors and their timing in early infancy.
Breastfeeding
The influence of breastfeeding on the risk of childhood atopy and asthma remains controversial. The following represents observational data accumulated to date. Some studies have shown protection, 64–66 whereas others have reported higher rates of allergy and asthma among breastfed children. 67,68 A meta-analysis 69 and several individual studies 66,70 showed that exclusive breastfeeding for at least 3 months was associated with lower rates of asthma between 2 and 5 years of age, with the greatest effect occurring among those with a parental history of atopy. One of the difficulties in interpreting these data lies in differentiating viral-associated wheeze in childhood from development of atopic asthma. In a longitudinal birth cohort study, breastfeeding was associated with a higher risk of atopic asthma in later childhood, with the greatest in fluence occurring among those with a maternal history of atopy. 67,68,71
The influence of avoiding nutritional allergens during breastfeeding is also controversial. In some studies, exclusion of milk, eggs and fish from the maternal diet was associated with decreased atopic dermatitis in infancy, 72,73 but other studies found no association. 40,74,75 Studies following children to 4 years of age have demonstrated no effect of maternal dietary restriction during lactation on the subsequent development of atopic diseases, including asthma. 76
Lung function
Decreased airway calibre in infancy has been reported as a risk factor for transient wheezing, 60 perhaps related to prenatal and postnatal exposure to environmental tobacco smoke. 26,27 Furthermore, the presence of airways with decreased calibre has been associated with increased bronchial responsiveness and increased symptoms of wheeze. 26 Several studies have suggested an association between reduced airway function in the first few weeks of life and asthma in later life. 62,77 The magnitude of the effect of this risk factor in isolation (i.e., without concomitant allergy) is unclear; perhaps individuals with smaller airways require less stimulus (i.e., airway inflammation) before symptoms become apparent.
Children with wheezing (and diagnosed asthma) persisting to adulthood have a fixed decrement in lung function as early as age 7 or 9 years. 13,78 Recent studies of preschool children have documented abnormal lung function in children with persistent wheezing as young as age 3 years. 61 However, some infants in whom persistent wheezing develops have normal lung function shortly after birth, which suggests a critical period of exposures within the first few years of life, before the development of these persistent abnormalities in expiratory flows. 60,79 In contrast, infants who exhibit early transient wheezing have decreased airflow shortly after birth. 60,80 Maternal smoking with in utero nicotine exposure has been correlated with this type of lung dysfunction, 26,27,60 but the effects of other exposures have been less well studied.
Family structure
Family size and the number and order of siblings may affect the risk of development of asthma. The hygiene hypothesis posits that exposure of an infant to a substantial number of infections and many types of bacteria stimulates the developing immune system toward nonasthmatic phenotypes. 81,82 This may be exemplified in the real world by large family size, whereby later-born children in large families would be expected to be at lower risk of asthma than first-born children, because of exposure to their older siblings’ infections.
Although this theory has been supported by some studies of allergy prevalence, 83,84 it has been partially refuted by recent studies of asthma prevalence suggesting that although large family size (more than 4 children) is associated with a decreased risk of asthma, birth order is not involved. 85,86 Furthermore, doubt has been cast on simplistic renditions of this hypothesis, in that infections per se cannot explain some epidemiologic patterns (e.g., prevalence rates for allergy and asthma are high in some South American countries, where exposures to infection are higher than in some countries with lower rates of asthma 3). In addition, not only allergic but also autoimmune and other chronic inflammatory diseases are increasing, 87 a trend that is difficult to explain by the hygiene hypothesis alone, since allergic and autoimmune diseases are associated with competing immunologic phenotypes.
Socio-economic status
Children of parents with lower socio-economic status have greater morbidity from asthma, 88–92 but findings with respect to the prevalence of asthma are mixed. 93–97 Such results may depend both on how socio-economic status is measured and on the specific outcome examined. Some studies have reported associations of lower socio-economic status with greater airway obstruction and symptoms but not with a diagnosis of asthma. 91,92 Whether socio-economic status is as relevant to the incidence of allergy and asthma as it is to the expression, severity and management of these diseases re mains unclear. Parental stress has also been prospectively associated with wheezing in infancy, 46 and family difficulties have been linked to asthma. 48,98 Children whose caregivers report high levels of stress and who have difficulties parenting are at greatest risk for asthma. 99
Antibiotics and infections
The use of antibiotics has been associated with early wheezing and asthma in several studies, 47,100,101 One suggested mechanism for this association is immunologic stimulation through changes in the bowel flora, but Kummeling and associates 100 found no coincident increase in eczema or atopy, despite increased wheezing rates, which would argue against this mechanism. Greater antibiotic use might also represent a surrogate marker for a higher numbers of infections (perhaps viral) in early life.
Viral infections of the lower respiratory tract affect early childhood wheezing. Whether lower respiratory tract infection promotes sensitization to aeroallergens causing persistent asthma is controversial: childhood viral infections might be pathogenic in some children but protective in others. 102–106 Infants of mothers with allergy or asthma have a relatively persistent maturational defect in Th1 cytokine synthesis in the first year of life, which may play a role in the development of persistent or severe viral infections. 107 Severe viral infection of the lower respiratory tract in genetically susceptible infants who are already sensitized to inhalant allergens may lead to deviation toward Th2 responses promoting asthma. It is unclear whether these effects of lower respiratory tract infection are virus-specific (e.g., respiratory syncytial virus, rhinovirus) or whether synergistic exposures to allergens can induce asthma even in individuals who are not genetically susceptible. Interactions of genes with environmental exposures (including allergens, air pollution, environmental tobacco smoke and diet) modulate the host response to infections. 108,109 It remains controversial whether the occurrence or timing of childhood infection is pathogenic or protective for the development and long-term outcome of asthma and allergy and of nonallergic wheeze phenotypes. This controversy relates in part to small sample size, cross-sectional analysis, lack of precise case definition and incomplete microbial assessment in studies of this phenomenon. 110,111
Respiratory infections in early childhood are associated with early wheezing, 109 but it is unclear whether infection alone has a role in the development of persistent asthma. Repeated lower respiratory tract infection may affect infants who are already at risk for asthma because of family history or atopy. 63,112 Severe infection with certain viruses such as respiratory syncytial virus 106 and rhinovirus 113 may play a role in persistent wheezing, although other studies have suggested no effect. 114 Considered as a proxy for viral infections, daycare attendance is associated with greater incidence of early wheeze but lower incidence of persistent wheeze. 115
Allergic sensitization
Total serum immunoglobulin E level, a surrogate for allergen sensitivity, has been associated with the incidence of asthma. 116 High levels of immunoglobulin E at birth were associated with greater incidence of both atopy 117–119 and aeroallergen sensitivity but not necessarily asthma. However, sensitization to aeroallergens, particularly house dust mite, cat and cockroach allergens, is well documented as being associated with asthma.
Immune responses in the developing infant and young child may affect the development of asthma. For example, impairment in interferon γ production at 3 months was associated with a greater risk of wheeze. 115 Immaturity in neonatal immune responses may promote the persistence of the Th2 immune phenotype and development of atopy, 120 but an association with persistent asthma is as yet unproven. More recent work has focused on the role of the innate immune system in handling and presentation of antigens and suggests that polymorphisms in Toll-like receptors 121,122 may play a greater role than previously recognized in the development of the skewed immune responses associated with persistent asthma.
Exposure to environmental tobacco smoke
Postnatal exposure to environmental tobacco smoke, especially from maternal smoking, has been consistently associated with respiratory symptoms of wheezing. 22,26,56 Exposure to environmental tobacco smoke also consistently worsens asthma symptoms and is a risk factor for severe asthma. 123,124
Exposure to animals
Although several studies have demonstrated a lower risk of development of atopy and asthma with exposure to farm animals in early life, the findings of studies of the influence of exposure to domestic cats and dogs have been inconsistent. 125,126 In some studies, exposure to cats was associated with a greater risk of allergic sensitization, 127 whereas other studies showed a lower risk. 128,129 Exposure to dogs may be protective not only against the development of specific sensitization to dog allergen 127,128 but also against other sensitization (e.g., to house dust mites) and asthma. Other studies of exposure to dogs have suggested that protection against wheezing may be mediated by high levels of endotoxin. 130
Gene-by-environment interactions
The effects of gene-by-environment interactions in asthma are complex. In some cases the genes code for enzymes that detoxify inhaled agents (e.g., glutathione transferase genes and environmental pollution), whereas in other cases, the exposures may have a more direct effect on gene expression via epigenetic mechanisms, such as DNA methylation or histone modification. Epigenetic modification of DNA is believed to be responsible for the phenotypic differences that develop over time between monozygotic twins. 131 It has been suggested that it is principally through epigenetic modification of DNA that lifestyle and chemical exposures affect susceptibility to diseases. 132 Nutrition and diet (e.g., folic acid, vitamin B12), smoking, exposure to microbial products, maternal stress and maternal care are potential factors influencing fetal genetic expression, and a further window for epigenetic modification in early life may allow environmental factors to modify a child’s genome with the potential to cause or prolong allergy and asthma. Further work is needed to verify and understand these risks.
Sex and gender
Sex affects the development of asthma in a time-dependent manner. Until age 13–14 years, the incidence and prevalence of asthma are greater among boys than among girls. 133–142 Studies through puberty 139,143–155 have shown a greater incidence of asthma among adolescent and young adult females 133–135,156,157 and a greater proportion of males with remission of asthma. 136–140 Before age 12, boys have more severe asthma than girls, 142 with higher rates of admission to hospital. 158–165 In contrast, adult females have more severe asthma than males, with more hospital admissions, 161,166,167 slower improvement, 120 longer hospital stays 161 and higher rates of readmission. 168 Most authors have attributed these changes in prevalence and severity to events of puberty, 140,141 although mechanisms for differences between the sexes have not been established.
In childhood, airway hyperresponsiveness is more common and more severe among males; 169 however, airway hyperresponsiveness increases in females during adolescence, 170,171 such that by adulthood it is both more common and more severe among adult women. 154,155,172–174 Similar findings have been reported from studies of atopy, which is more common in males before age 13; 175 during adolescence, the rate of new-onset atopy is higher among females, 176,177 so that by young adulthood the prevalence of atopy is almost equal.
The influence of some environmental risk factors such as allergens may be modified by sex. In one study of adults, 18% of women with asthma, but only 2.3% of men with asthma, had normal results on common tests related to atopy (negative skin prick tests, immunoglobulin E < 100 IU/mL and eosinophilia < 5%), 178 which suggested different disease mechanisms between the sexes. Interactions have been found between maternal and paternal history of atopy, breastfeeding and sex of the child in terms of the risk of asthma and atopy. 71 Finally, the influence of obesity on the development of asthma is greater among women than among men and has not been shown to be influenced by caloric intake or physical activity. 179,180 Some have suggested that the relation between obesity and asthma may be causal, given the consistency, temporal association and dose–response relationships reported in the epidemiologic literature, but the mechanisms remain to be elucidated. 181
Adult-onset asthma
Asthma in adults may have persisted from childhood, may have occurred as a relapse of earlier childhood asthma (whether or not recalled by the individual) or may be true adult-onset asthma with no symptoms in earlier life. 182–184 New-onset asthma in adulthood may have environmental (especially occupational) causes with or without allergen sensitization. 185–187 Although adult asthma may develop in relation to specific drug treatments (e.g., β-blockers, nonsteroidal anti-inflammatory drugs) or, in women, the use of hormone replacement therapy, 188 occupational exposure to sensitizing agents or irritants is more common.
Occupational asthma
Asthma related to workplace exposures has been documented in many occupational settings. Commonly associated occupations and exposures include car painting (isocyanates), hairdressing (various chemicals), domestic and commercial cleaning (cleaning solutions), health care professions (latex) and baking (flour dust), among many others. 189
The relation between exposure to substances in the work-place and new-onset adult asthma was explored among 6837 participants with no previously reported asthma symptoms in phase I of the European Community Respiratory Health Study. 187 Exposure to substances known to cause occupational asthma was associated with a higher risk of asthma overall (relative risk [RR] 1.6, 95% confidence interval [CI] 1.1–2.3) and of asthma defined by airway hyperresponsiveness (RR 2.4, 95% CI 1.3–4.6). Of common occupations, nursing was associated with the highest risk of occupational asthma (RR 2.2, 95% CI 1.3–4.0, p = 0.007), whereas exposure to an acute inhalation event, such as fire, mixing of cleaning agents or a chemical spill, was associated with an even higher risk (RR 3.3, 95% CI 1.0–11.1, p = 0.05). The population attributable risk of occupational exposure for adult asthma in that study ranged from 10% to 25%.
Other risk factors for adult asthma
Smoking tobacco 190 or marijuana 191,192 may give rise to symptoms suggesting asthma, although symptoms of cough and sputum production, suggesting chronic bronchitis, are more common. As in childhood, the differential diagnosis should include other forms of airway inflammation and other causes of intermittent dyspnea and wheezing, such as cardiac failure. However, new-onset asthma can occur at any age, without prior illness or concomitant disease. Atopy as a risk factor for asthma is less common with increasing age, 193 but occasionally it is the dominant trigger. Air pollution may affect adult asthma, but more often it is a factor worsening pre-existing asthma rather than a cause of incident asthma. 194–196
Conclusions
Many cross-sectional studies have confirmed increases in the incidence and prevalence of asthma over the past 2 to 3 decades, but much remains unknown as to the fundamental immunologic, genetic and environmental mechanisms underlying the development of this condition and its increased expression, especially in the developed world. Nonetheless, some risk factors have now been clearly and consistently identified. For instance, avoidance of maternal smoking in pregnancy and in the early postpartum period can be strongly encouraged, as can avoidance of known occupational sensitizers. In contrast, previous advice to avoid animals and to breastfeed as long as possible to reduce the risks of asthma has been challenged by more recent studies. It is likely that detailed studies of gene-by-environment interactions and of epigenetics will eventually untangle the inconsistencies among the many putative exposures and outcomes. Although there are indications that the increase in asthma has reached a plateau, at least in countries with the highest prevalence rates, much of the epidemiology and many of the risk factors for asthma remain to be adequately explained. Reduction in risk, and perhaps even true primary prevention of asthma, remains elusive but is a key goal of asthma management.
-
The prevalence of asthma varies widely around the world, probably because of gene-by-environment interactions.
-
Prenatal risk factors for asthma may include maternal smoking, diet and nutrition, stress, use of antibiotics and delivery by cesarean section.
-
Childhood risk factors for asthma may include allergic sensitization, environmental tobacco smoke, exposure to animals, breastfeeding, decreased lung function in infancy, family size and structure, socio-economic status, antibiotics and infections, and sex and gender.
-
Occupational exposures constitute a common risk factor for adult asthma.
Key points
Footnotes
-
This article has been peer reviewed.
Competing interests: Piush Mandhane has received speaker’s honoraria from Merck Canada and the Edmonton Thoracic Society. None declared for Padmaja Subbarao and Malcolm Sears.
Contributors: All authors contributed to the development and editing of the publication, and all approved the final version submitted for publication.
Funding: The Canadian Thoracic Society has received funding to facilitate the knowledge translation activities of the CTS Asthma Committee from AstraZeneca Canada, GlaxoSmithKline Inc., Merck Frosst Canada and Novartis Pharmaceuticals. None of the sponsors played a role in the collection, review, analysis or interpretation of the scientific literature or in any decisions regarding the key messages presented in the case studies.
Acknowledgement: The authors thank Dr. Peter Paré, iCapture Centre, University of British Columbia, for his invaluable assistance in editing and contributing to the genetics sections of this manuscript.
This article is the first in a 7-part case study series that was developed as a knowledge translation initiative of the Canadian Thoracic Society Asthma Committee. The series aims to educate and inform primary care providers and nonrespiratory specialists about the diagnosis and management of asthma. The key messages presented in the cases are not clinical practice guidelines but are based on a review of the most recent scientific evidence available. Financial support for the publication of this series has been provided, in part, by the Canadian Thoracic Society.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.
- 33.↵
- 34.↵
- 35.
- 36.↵
- 37.↵
- 38.
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.
- 56.↵
- 57.
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.
- 90.
- 91.↵
- 92.↵
- 93.↵
- 94.
- 95.
- 96.
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.
- 104.
- 105.
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.
- 135.↵
- 136.↵
- 137.
- 138.
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.
- 145.
- 146.
- 147.
- 148.
- 149.
- 150.
- 151.
- 152.
- 153.
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.
- 160.
- 161.↵
- 162.
- 163.
- 164.
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.
- 184.↵
- 185.↵
- 186.
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.
- 196.↵
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Impacts of ambient air quality on acute asthma hospital admissions during the COVID-19 pandemic in Oxford City, UK: a time-series study
- Perinatal and early life factors and asthma control among preschoolers: a population-based retrospective cohort study
- Disadvantage in early-life and persistent asthma in adolescents: a UK cohort study
- Impact of pharmacist-led educational intervention on knowledge of self-management among asthmatic patients: a prospective cohort study
- Development of a conceptual model of childhood asthma to inform asthma prevention policies
- Differential asthma risk following respiratory infection in children from three minority populations
- Isolated night cough in children: how does it differ from wheeze?
- What have we learnt from studies on the association between urbanisation and asthma prevalence?
- New-onset asthma in a bilateral lung transplant patient
- Effects of policy-driven hypothetical air pollutant interventions on childhood asthma incidence in southern California
- Does early onset asthma increase childhood obesity risk? A pooled analysis of 16 European cohorts
- Improving the global diagnosis and management of asthma in children
- {beta}2-Adrenoreceptor is a regulator of the {alpha}-synuclein gene driving risk of Parkinsons disease
- Social inequalities in wheezing in children: findings from the UK Millennium Cohort Study
- Association between traffic-related air pollution and asthma in preschool children in a national Japanese nested case-control study
- Job insecurity is associated with adult asthma in Germany during Europe's recent economic crisis: a prospective cohort study
- Pediatric Asthma in a Nutshell
- Lipid mediator profiles differ between lung compartments in asthmatic and healthy humans
- Ten years of asthma admissions to adult critical care units in England and Wales
- Mechanism of Action of Inhibition of Allergic Immune Responses by a Novel Antedrug TLR7 Agonist
- The role of prenatal, perinatal and postnatal factors in the explanation of socioeconomic inequalities in preschool asthma symptoms: the Generation R Study
- Asthma and allergies in Jamaican children aged 2-17 years: a cross-sectional prevalence survey
- Joint effects of birth outcomes and childhood body mass index on respiratory symptoms
More in this TOC Section
Similar Articles

