


Pupil dilation is important for diagnosis
The dilated fundus examination can be valuable to non-ophthalmologists for diagnosis. For example, acute loss of vision can be due to causes such as retinal detachment, occlusion of the central retinal artery or vein, vitreous hemorrhage and ischemic optic neuropathy, each having characteristic findings within the portion of the fundus visualized with a direct ophthalmoscope (for examples, see Appendix 1A–1C, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.101597/-/DC1). When raised intracranial pressure is a possibility, dilation may aid in visualizing papilledema (Appendix 1D) but will affect assessment of the pupils for several hours.
Dilated fundus examination is an important therapeutic tool
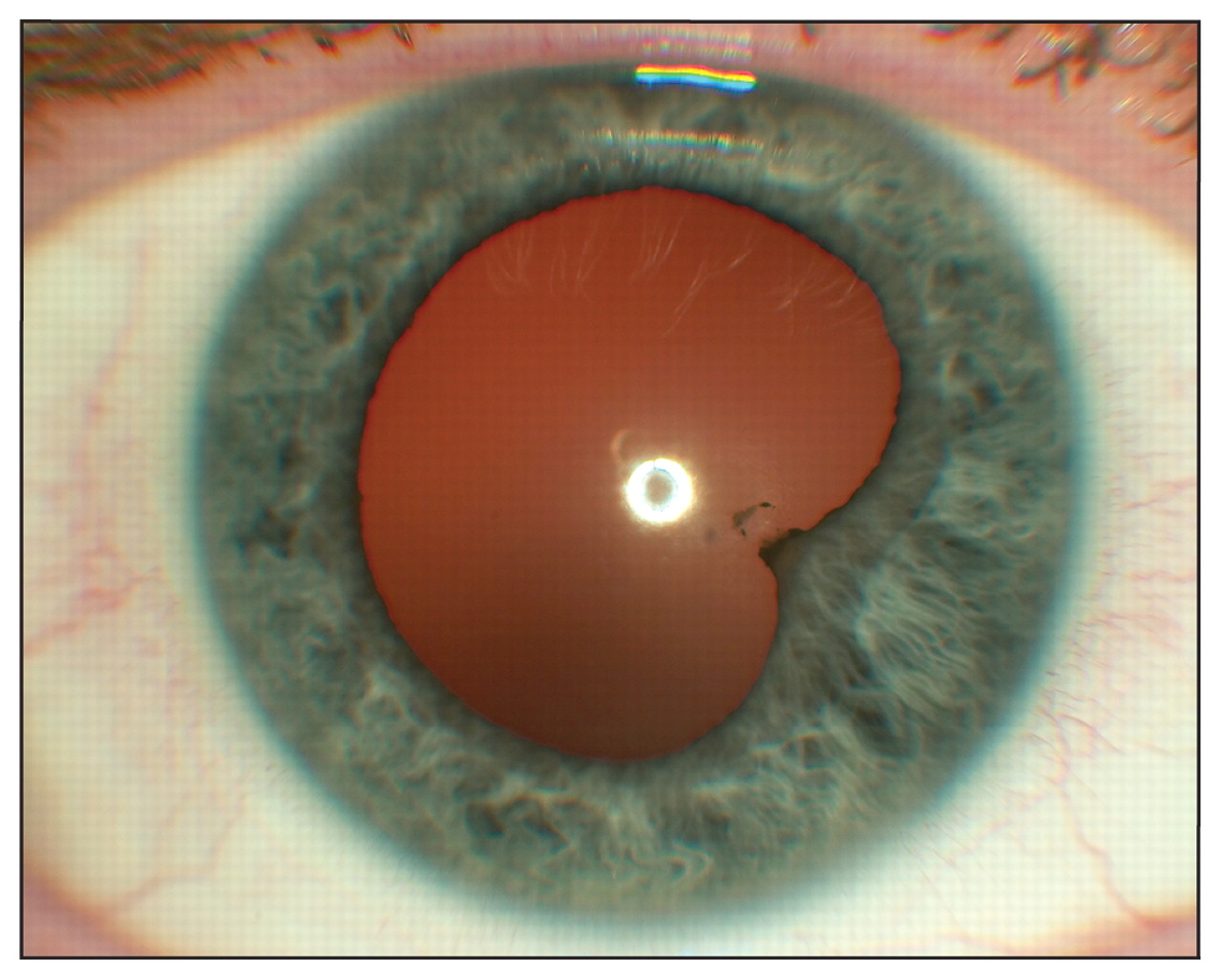
Muscarinic antagonist agents (e.g., homatropine 2%) are used routinely by ophthalmologists in the treatment of anterior uveitis (iritis).1 They prevent adherence of the iris to the lens (Figure 1) and provide safe, effective pain relief by paralyzing the ciliary body (cycloplegia). These drops can also be used by non-ophthalmologists to alleviate symptoms of large corneal abrasions, various forms of keratitis, and iritis while the patient awaits consultation with an ophthalmologist.1
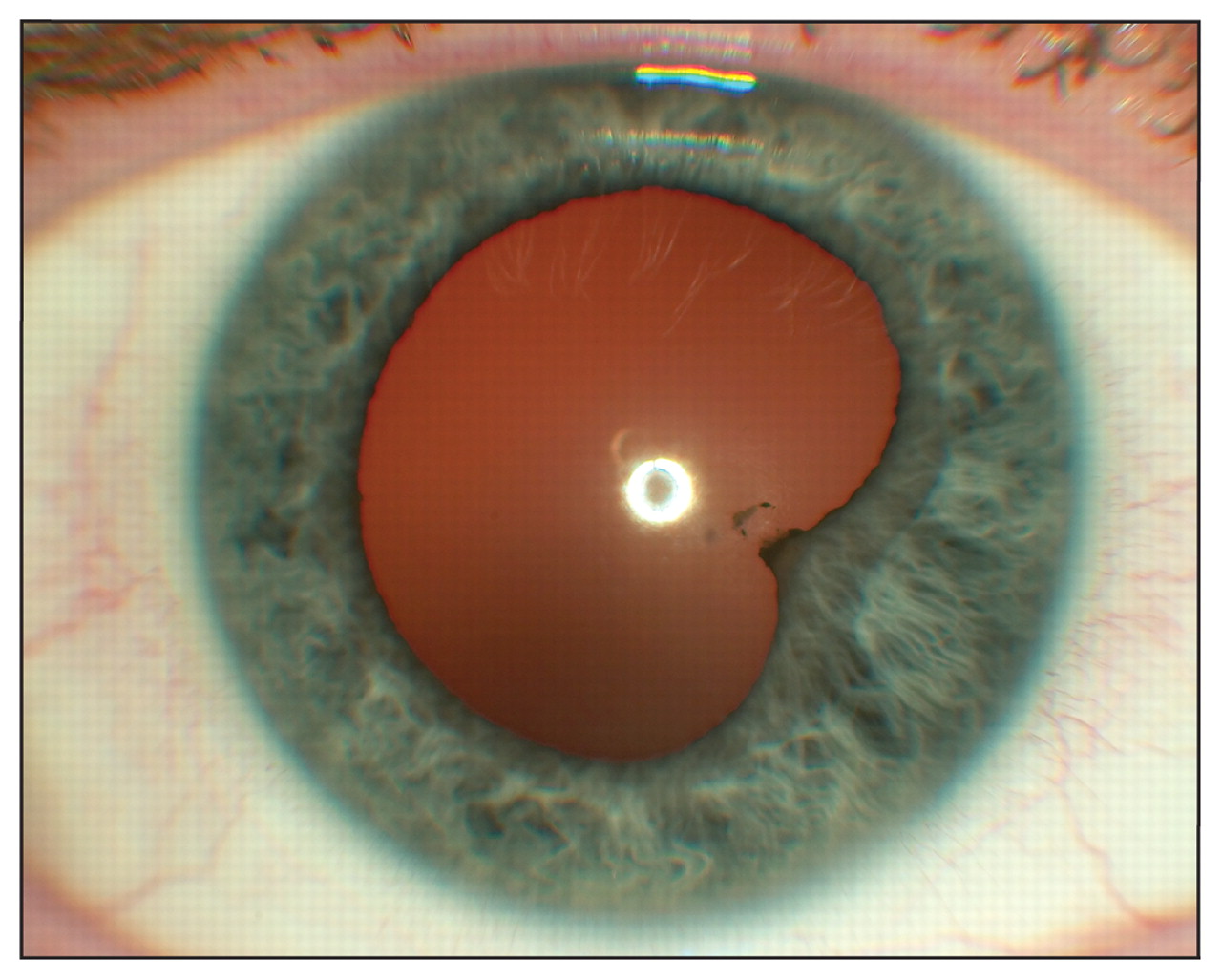
Adherence of the iris to the lens (posterior synechia) in idiopathic acute iritis. If extensive, synechiae can block movement of the aqueous humour through the pupil, leading to acute angle-closure glaucoma. This patient’s synechia was lysed by dilation.
Routine dilation takes 20 minutes and lasts a few hours
Maximal dilation with tropicamide 0.5% is reached after 20–30 minutes and reverses over three to six hours.2 The cycloplegia that is desirable in therapeutic use, but bothersome to the patient by impairing accommodation, is milder and briefer with this agent than with other muscarinic antagonists. Blurred vision, especially at near distances, is normal for several hours following dilation.
Patients require instructions after pupil dilation
Despite the low risk of acute angle-closure glaucoma, the patient should be warned of the symptoms (e.g., pain, progressive blurring of vision, headache, nausea) and advised to seek immediate care should they occur. Sunglasses can be worn to increase comfort in bright surroundings while the pupils are dilated. The patient should be advised not to drive following dilation, until accommodation has returned to normal.3
The risk of precipitating acute angle-closure glaucoma with pupil dilation is very low
Acute angle closure causes a dramatic rise in intraocular pressure and, if left untreated, leads to permanent vision loss from glaucoma. The fear of precipitating such an event with dilation may be a barrier to thorough funduscopy. However, large population-based studies and a systematic review including nearly 600 000 patients have shown that the risk is very low (1 to 6 per 20 000).4,5
CMAJ invites submissions to “Five things to know about …” Submit manuscripts online at http://mc.manuscriptcentral.com/cmaj
Footnotes
-
For references, see Appendix 2 (www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.101597/-/DC1).
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Pupil dilation is important for diagnosis
- Dilated fundus examination is an important therapeutic tool
- Routine dilation takes 20 minutes and lasts a few hours
- Patients require instructions after pupil dilation
- The risk of precipitating acute angle-closure glaucoma with pupil dilation is very low
- Footnotes
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

