


Abstract
Background: Data on resting heart rate and risk of all-cause and cardiovascular mortality are inconsistent; the magnitude of associations between resting heart rate and risk of all-cause and cardiovascular mortality varies across studies. We performed a meta-analysis of prospective cohort studies to quantitatively evaluate the associations in the general population.
Methods: We searched PubMed, Embase and MEDLINE from inception to Jan. 1, 2015. We used a random-effects model to combine study-specific relative risks and 95% confidence intervals (CIs). We used restricted cubic spline functions to assess the dose–response relation.
Results: A total of 46 studies were included in the meta-analysis, involving 1 246 203 patients and 78 349 deaths for all-cause mortality, and 848 320 patients and 25 800 deaths for cardiovascular mortality. The relative risk with 10 beats/min increment of resting heart rate was 1.09 (95% CI 1.07–1.12) for all-cause mortality and 1.08 (95% CI 1.06–1.10) for cardiovascular mortality. Compared with the lowest category, patients with a resting heart rate of 60–80 beats/min had a relative risk of 1.12 (95% CI 1.07–1.17) for all-cause mortality and 1.08 (95% CI 0.99–1.17) for cardiovascular mortality, and those with a resting heart rate of greater than 80 beats/min had a relative risk of 1.45 (95% CI 1.34–1.57) for all-cause mortality and 1.33 (95% CI 1.19–1.47) for cardiovascular mortality. Overall, the results did not differ after adjustment for traditional risk factors for cardiovascular disease. Compared with 45 beats/min, the risk of all-cause mortality increased significantly with increasing resting heart rate in a linear relation, but a significantly increased risk of cardiovascular mortality was observed at 90 beats/min. Substantial heterogeneity and publication bias were detected.
Interpretation: Higher resting heart rate was independently associated with increased risks of all-cause and cardiovascular mortality. This indicates that resting heart rate is a predictor of all-cause and cardiovascular mortality in the general population.
Resting heart rate is a familiar, straightforward and inexpensive-to-measure clinical variable, and it can be modified by a number of factors, such as physical activity, psychologic stress, smoking, intake of omega-3 fatty acids and medications.1–4 Higher heart rate has been linked to increased risks of cardiovascular disease and premature mortality through a multitude of actions, including its detrimental effects on progression of coronary atherosclerosis, on occurrence of myocardial ischemia and ventricular arrhythmia, on left ventricular function and on circulating levels of inflammatory markers.5–7 However, measurement of resting heart rate has not been recommended in American and European guidelines on risk assessment of cardiovascular disease.8,9 The major reasons for this may be that the magnitude of risk with each increment of higher resting heart rate has been inconsistent among studies, and that resting heart rate may not be an independent predictor because higher heart rate coexists with traditional risk factors of cardiovascular disease.10–13 In addition, data are lacking on the dose–response relation between resting heart rate and all-cause and cardiovascular mortality,5,9 although a previous review showed a continuous increase in risk with resting heart rate above 60 beats/min.5
Therefore, we conducted a meta-analysis of prospective cohort studies involving the general population, following the MOOSE checklist,14 to assess the risk of all-cause and cardiovascular mortality associated with each increment of 10 beats/min; to evaluate the possible dose–response relation by restricted cubic spline functions and by pooling risks of all-cause and cardiovascular mortality for comparable categories of resting heart rate (60–80 beats/min and > 80 beats/min); and to evaluate the effect of traditional risk factors of cardiovascular disease on the association of resting heart rate with risk of all-cause and cardiovascular mortality.
Methods
Literature search and selection
We searched PubMed, Embase and MEDLINE from inception to Jan. 1, 2015, restricting the search to studies involving humans and published in English or Chinese. Details of the search strategy are shown in Appendix 1 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150535/-/DC1). We reviewed the reference lists from retrieved articles to search for further relevant studies.
Studies were included if they met the following criteria: the study group was the general population (i.e., excluding studies in disease-specific populations); the exposure of interest was resting heart rate; the outcome of interest was all-cause or cardiovascular mortality; age- or multivariate-adjusted relative risk estimates with 95% confidence intervals (CIs) were provided; and the study used a prospective design. If data were duplicated in more than 1 study, we included the study with the longest follow-up duration. Two investigators (D.Z. and X.S) independently conducted the literature search and selection.
Data extraction
The same 2 investigators independently extracted the following data from each study: the first author’s last name, publication year, follow-up duration, country or region where the study was performed, number of participants and deaths, method of resting heart rate assessment, use of heart rate–lowering medication at baseline, variables adjusted for in the analysis and relative risk estimates with corresponding 95% CIs for each category of resting heart rate.
For dose–response analysis with restricted cubic spline models, we extracted the number of deaths and participants (person-years) and relative risk (95% CI) for each category of resting heart rate. For each study, the median level of resting heart rate for each category was assigned to each corresponding RR estimate. If the upper boundary of the highest category was not provided, we assumed that the boundary had the same amplitude as the adjacent category. We extracted relative risk estimates that reflected the greatest degree of control for potential confounders.
Statistical analysis
Pooled measurement was calculated as the inverse variance-weighted mean of the logarithm of relative risk for an increment of 10 beats/min in resting heart rate. We used a random-effects model to combine study-specific relative risks, which considers both within-study and between-study variation.15 The I2 test was used to assess heterogeneity.16 We conducted meta-regression and subgroup analysis to explore potential sources of heterogeneity and perform comparisons between groups, and we calculated p values from meta-regression with a permutation test of 1000 to control spurious findings.17 A sensitivity analysis was performed, with one study removed at a time to assess whether the results could have been affected markedly by a single study. We evaluated publication bias using the Egger regression asymmetry test.18 When publication bias was detected, we adopted the trim-and-fill method to adjust the meta-analysis. This method first “trims” the smaller studies, causing funnel plot asymmetry, and estimates the true “centre” of the funnel with the trimmed funnel plot, and then replaces the omitted studies and their missing “counterparts” around the centre (filling).19 In addition, we pooled relative risks for comparable categories of resting heart rate (60–80 beats/min and > 80 beats/min) as compared with the lowest category. We assessed study quality using the 9-star Newcastle-Ottawa Scale.20
To assess the dose–response relation, we performed a 2-stage random-effects dose–response meta-analysis,21 taking into account between-study heterogeneity. In the first stage, a restricted cubic spline model with 3 knots at the 25th, 50th and 75th percentiles22 of the levels of resting heart rate was estimated using generalized least-square regression, taking into account the correlation within each set of published relative risks.23 We then combined study-specific estimates using the restricted maximum likelihood method in a multivariate random-effects meta-analysis.24 A p value for nonlinearity was calculated by testing the null hypothesis that the coefficient of the second spline is equal to 0. We used 45 beats/min (the lowest value in the included studies) as the reference. In addition, 70 beats/min was then adopted as the reference to examine the potentially protective effect by lower values of heart rate (45–69 beats/min). All statistical analyses were performed with STATA version 12.0. All reported probabilities (p values) were 2-sided, with p < 0.05 considered significant.
Results
Search results and study characteristics
After a review of titles and abstracts of the records identified through the literature search, 185 potentially eligible records were identified. After a review of the full texts, 139 records were excluded (Appendix 1). Of the 46 prospective cohort studies included in the meta-analysis, 40 studies provided the results for all-cause mortality, involving 1 246 203 patients and 78 349 deaths, and 29 studies provided the results for cardiovascular mortality, involving 848 320 patients and 25 800 deaths. The follow-up duration ranged from 3 to 40 years. The study quality ranged from 5 to 9 stars (Appendix 2, www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150535/-/DC1). Details about the included studies are shown in Table 1.
Characteristics of studies included in the meta-analysis
Quantitative synthesis
All-cause mortality
Pooled results on resting heart rate and risk of all-cause mortality are shown in Table 2. The multivariate-adjusted relative risk of all-cause mortality with every 10 beats/min increment was 1.09 (95% CI 1.07–1.12) (Figure 1). Publication bias was detected (p < 0.01), and the corrected effect with the trim-and-fill method was 1.04 (95% CI 1.02–1.06). No individual study had an excessive influence to the pooled effect in sensitivity analysis. The relative risk of all-cause mortality was 1.12 (95% CI 1.07–1.17) for those with a resting heart rate of 60–80 beats/min and 1.45 (95% CI 1.34–1.57) for those with a resting heart rate greater than 80 beats/min.
Pooled results on resting heart rate and risk of all-cause mortality
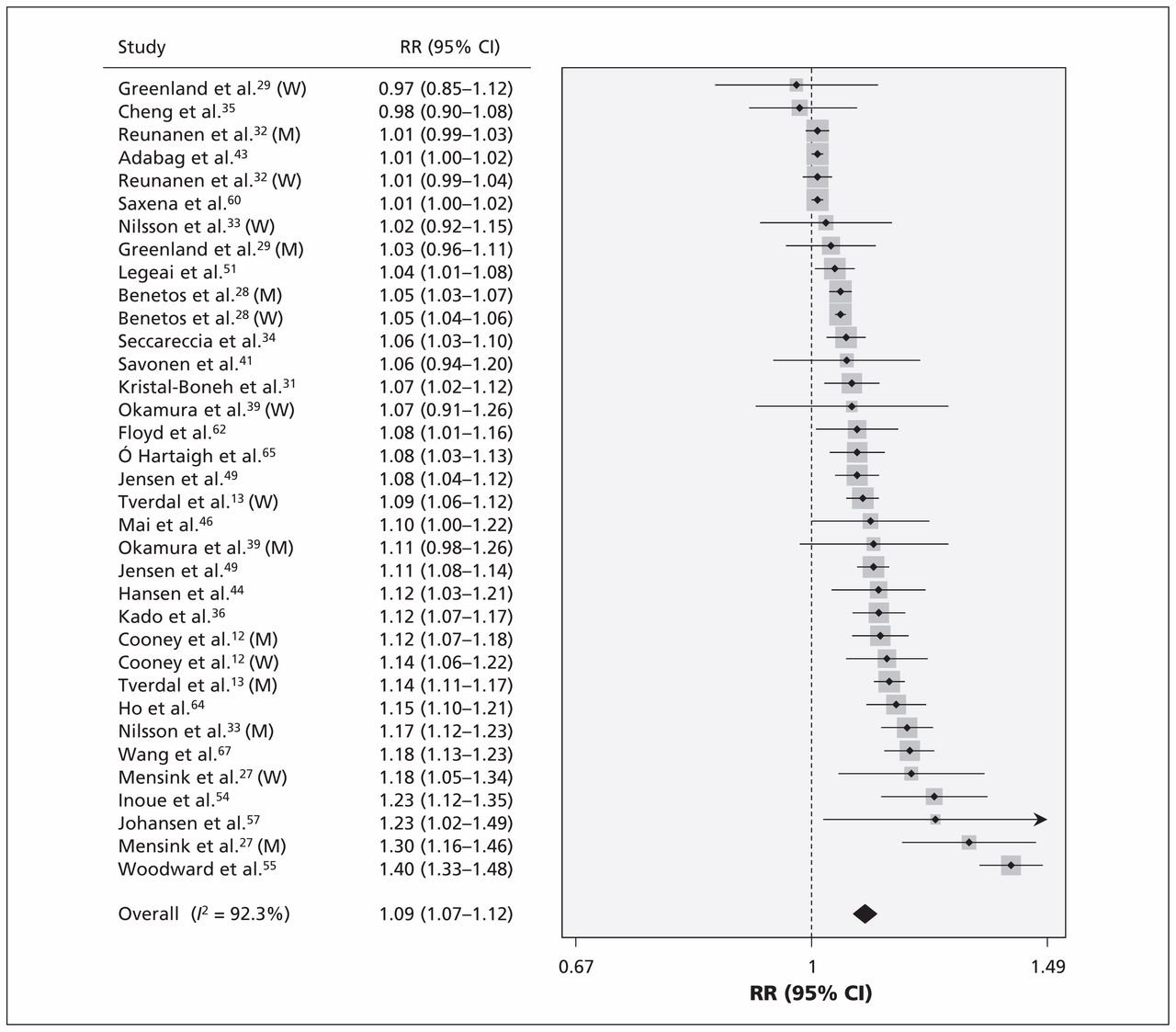
Risk of all-cause mortality for each 10 beats/min increase in resting heart rate. Note: CI = confidence interval, M = men, RR = relative risk, W = women.
Cardiovascular mortality
Pooled results on resting heart rate and risk of cardiovascular mortality are shown in Table 3. The relative risk of cardiovascular mortality with every 10 beats/min increment was 1.08 (95% CI 1.06–1.10) (Figure 2). Publication bias was detected (p < 0.01), and the corrected effect with the trim-and-fill method was 1.03 (95% CI 1.01–1.06). No individual study had an excessive influence to the pooled effect in sensitivity analysis. The relative risk of cardiovascular mortality was 1.08 (95% CI 0.99–1.17) for those with a resting heart rate of 60–80 beats/min and 1.33 (95% CI 1.19–1.47) for those with a rate of greater than 80 beats/min.
Pooled results on resting heart rate and risk of cardiovascular mortality

Risk of cardiovascular mortality for each 10 beats/min increase in resting heart rate. Note: CI = confidence interval, M = men, RR = relative risk, W = women.
Subgroup analysis and meta-regression
As shown in Tables 2 and 3, between-study heterogeneity was found. Overall, no single factor successfully explained the between-study heterogeneity; however, when all of the factors were included in meta-regression simultaneously, they explained all (100%), most (89.2%, 61.9%) or part (44.9%, 37.6%) of the heterogeneity (Appendix 3, www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150535/-/DC1).
To examine potential influencers (e.g., medication and disease states) of resting heart rate, we conducted several subgroup analyses. Among patients not taking heart rate–lowering medication, the relative risk of all-cause and cardiovascular mortality was 1.11 (95% CI 1.06–1.16) and 1.13 (95% CI 1.07–1.19), respectively, with each 10 beats/min increment. To take into account the possibility of an effect by an existing or preclinical disease at baseline, we conducted a separate analysis in which deaths within the first 6 months to 5 years of follow-up were excluded, and the risk of all-cause mortality and cardiovascular mortality with each 10 beats/min increment was 1.09 (95% CI 1.06–1.13) and 1.09 (95% CI 1.05–1.12), respectively. For studies excluding patients with cardiovascular disease at baseline, the relative risk of all-cause mortality and cardiovascular mortality with each 10 beats/min increment was 1.09 (95% CI 1.06–1.12) and 1.06 (95% CI 1.04–1.08), respectively.
Dose–response analysis with restricted cubic spline functions
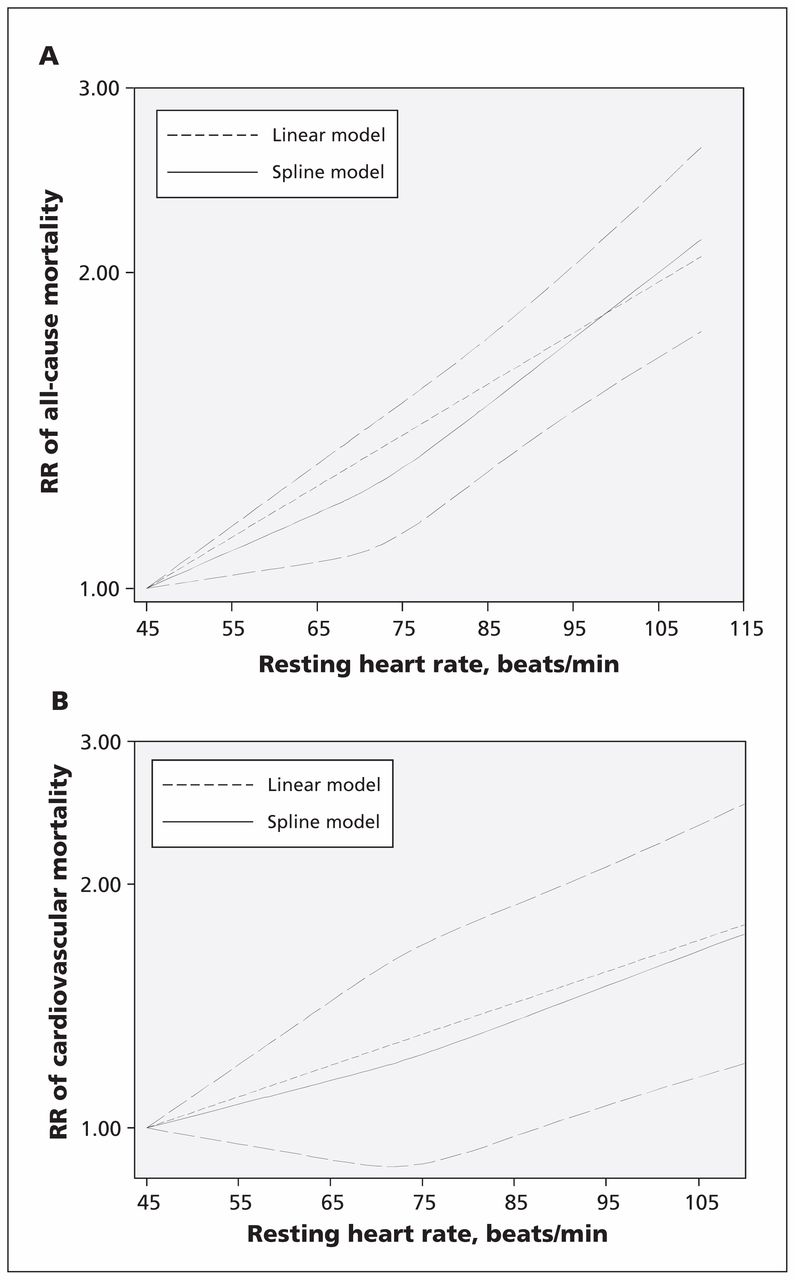
For all-cause mortality, data from 13 studies including 26 636 deaths were used. The departure from a linear relation was not significant (pfor nonlinearity = 0.1). Compared with 45 beats/min, the risk of all-cause mortality increased significantly with increasing levels of resting heart rate (Figure 3A).
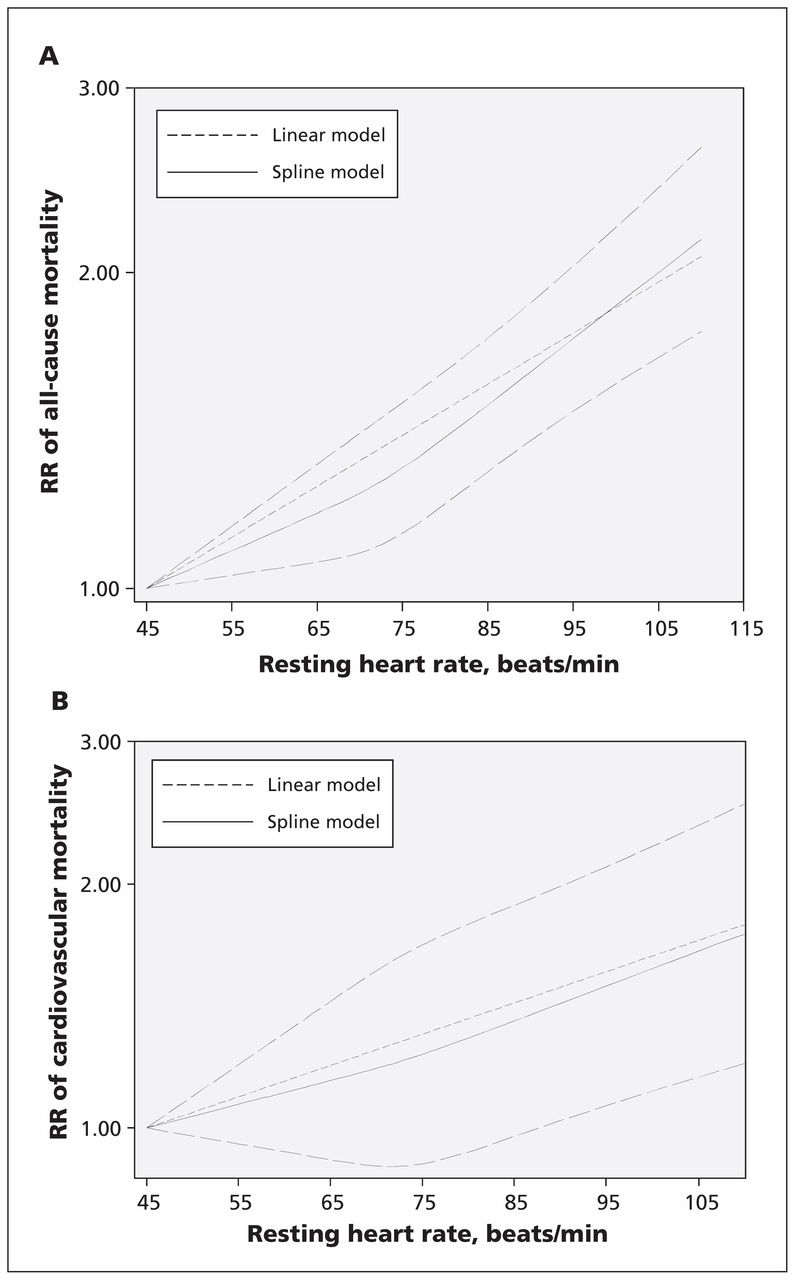
The dose–response analysis of resting heart rate with risk of (A) all-cause mortality and (B) cardiovascular mortality. The solid and long dash lines represent the estimated relative risks (RRs) and 95% confidence intervals. The short dash lines represent the linear relation.
For cardiovascular mortality, data from 10 studies including 6502 deaths were used. The departure from a linear relation was not significant (pfor nonlinearity = 0.6). Compared with 45 beats/min, the risk of cardiovascular mortality increased significantly at 90 beats/min (Figure 3B).
With use of 70 beats/min as the reference, the linear dose–response analysis indicated a protective effect of lower resting heart rate (45–69 beats/min) on risk of all-cause and cardiovascular mortality, respectively (Appendix 4, www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150535/-/DC1).
Interpretation
Results from this meta-analysis suggest the risk of all-cause and cardiovascular mortality increased by 9% and 8% for every 10 beats/min increment of resting heart rate. Compared with 45 beats/min, the risk of all-cause mortality increased significantly with increasing resting heart rate in a linear relation, but a significantly increased risk of cardiovascular mortality was observed at 90 beats/min. The threshold (90 beats/min) associated with cardiovascular mortality is consistent with the traditionally defined tachycardia threshold of 90 or 100 beats/min for prevention of cardiovascular disease.5
One mechanism is that higher resting heart rate is a marker of an imbalance between the vagal and the sympathetic tone, and dysfunctional autonomic nervous activity likely plays a central role in the pathogenesis of numerous adverse health conditions.5,68 A relatively high heart rate has direct detrimental effects on progression of coronary atherosclerosis, on occurrence of myocardial ischemia and ventricular arrhythmias, and on left ventricular function. In this meta-analysis, the magnitude of association between resting heart rate and all-cause mortality was stronger than that with cardiovascular mortality, and this discrepancy can be expected because resting heart rate has also been found to be associated with noncardiovascular mortality.28,34,44,51,54,69
One main concern lies in whether a high resting heart rate is an independent predictor, because higher heart rates coexist with traditional risk factors of cardiovascular disease and poor health status.10–13,70 Overall, the association of resting heart rate with risk of all-cause and cardiovascular mortality is independent of traditional risk factors of cardiovascular disease, suggesting that resting heart rate is a predictor of mortality in the general population. In addition, previous studies found that resting heart rate is also related to prognosis in settings of substantial cardiovascular comorbidities, such as renal disease, erectile dysfunction and pulmonary hypertension, as well as in noncardiovascular conditions such as chronic obstructive pulmonary disease.71 To comply with the definition of a risk factor, a reduction in heart rate by therapy should be associated with improved clinical outcomes. Several trials with ivabradine (the specific heart rate–reducing agent without any other known cardiovascular effects) have been conducted to explore this issue. Although no benefit was observed of heart rate reduction on outcomes in patients with stable coronary artery disease without clinical heart failure and with a heart rate of 70 beats/min or greater,72 a higher heart rate may serve as a risk factor for cardiovascular mortality and all-cause mortality in patients with left-ventricular systolic dysfunction with coronary artery disease and/or heart failure73,74 (Appendix 5, www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.150535/-/DC1). These findings suggest that the association of heart rate reduction with outcomes may differ among populations of different risk, and higher heart rate is due to different pathophysiological mechanisms in different conditions.5
A linear relation was found between resting heart rate and risk of all-cause mortality and cardiovascular mortality, respectively. Among the included studies, only 3 studies described the dose–response relation continuously,13,34,64 and all indicated a linear relation. However, a J-shaped curve was also indicated by categorizing resting heart rate.44,48,55 Because this is a meta-analysis focusing on the general population (i.e., excluding studies in disease-specific populations), patients with a very low resting heart rate are likely to be more physically fit. Therefore, more benefit could be anticipated for patients with a very low resting heart rate. In addition, findings from trials involving patients with cardiovascular disease also indicated the possibility of “the slower the heart rate, the better.”75
Limitations
Our study had several limitations. First, measurement of resting heart rate is susceptible to numerous factors,76 and nighttime heart rate was found to be a better prognostic variable relative to resting heart rate and 24-hour heart rate; nighttime heart rate should be a better measure of heart rate because both the interference of sensory input as well as physical and mental activities were minimized.57 Second, patients with cardiovascular disease or subclinical cardiovascular disease with no antihypertensive treatment at baseline could have started taking heart rate–lowering medications during follow-up, and this would lead to an underestimation of the true magnitude of the observed associations. Third, although we extracted risks that reflected the greatest degree of control for potential confounders, the covariates adjusted and the extent to which they were adjusted varied in the original studies. Fourth, single factor did not successfully explain the substantial between-study heterogeneity; however, meta-regression suggested that population characteristics and study designs might contribute in concrete to the heterogeneity. Finally, we searched for only English- and Chinese-language studies, and we found publication bias. However, the observed associations remained after incorporating theoretical missing studies.
Conclusion
Resting heart rate was associated with risk of all-cause and cardiovascular mortality in the general population, independent of traditional cardiovascular risk factors. However, considering that the covariates adjusted for and the extent to which they were adjusted for varied in the included studies, as well as the presence of between-study heterogeneity and publication bias, collaborative pooling of individual participant data from prospective cohort studies is needed to better describe the association. Identification of the contribution of heart rate reduction on effects of cardiovascular events and mortality by other interventions like exercise with a clinical trial in the general population will provide evidence on whether heart rate is also a risk factor. Further studies are warranted to develop a prediction algorithm that would consider both resting heart rate and classic cardiovascular risk factors to allow physicians to use resting heart rate in clinical settings.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All of the authors made substantial contributions to study conception and design, acquisition of data, analysis and interpretation of data; and drafting of the article or revising it critically for important intellectual content. All of the authors gave final approval of the version to be published and agreed to act as guarantors of the work.
- Accepted September 17, 2015.
References
In this issue
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Which Components of the Haemodynamic Response to Active Stand Predict Cardiovascular Disease and Mortality? Data From The Irish Longitudinal Study on Ageing
- Heart rate: an accessible risk indicator in adult congenital heart disease
- Heart Rate as a Predictor of Mortality in Heart Failure Patients at the Time of Discharge from the Intensive Care Unit
- On the reliability of wearable technology: A tutorial on measuring heart rate and heart rate variability in the wild
- On the reliability of wearable technology: A tutorial on measuring heart rate and heart rate variability in the wild
- Cardiovascular outcomes in obstructive sleep apnoea and implications of clinical phenotyping on effect of CPAP treatment
- Isometric exercise versus high-intensity interval training for the management of blood pressure: a systematic review and meta-analysis
- Resting Heart Rate predicts all-cause mortality in sub-Saharan African Patients with Heart Failure: Insight from the Douala Heart failure registry (Do-HF)
- Development and validation of risk scores for all-cause mortality for the purposes of a smartphone-based 'general health score application: a prospective cohort study using the UK Biobank
- Resting heart rate and incident venous thromboembolism: the Multi-Ethnic Study of Atherosclerosis
- Effect of exercise referral schemes upon health and well-being: initial observational insights using individual patient data meta-analysis from the National Referral Database
- Cardiovascular Effects of Switching From Tobacco Cigarettes to Electronic Cigarettes
- Impact of changes in heart rate with age on all-cause death and cardiovascular events in 50-year-old men from the general population
- A Controlled Increase in Dietary Phosphate Elevates BP in Healthy Human Subjects
- Resting heart rate, temporal changes in resting heart rate, and overall and cause-specific mortality
- Heritability of resting heart rate and association with mortality in middle-aged and elderly twins
- Heart Rate Recovery and Risk of Cardiovascular Events and All-Cause Mortality: A Meta-Analysis of Prospective Cohort Studies
- Association between resting heart rate and coronary artery disease, stroke, sudden death and noncardiovascular diseases: a meta-analysis
- Surface Electrocardiogram Predictors of Sudden Cardiac Arrest
- How valuable is physical examination of the cardiovascular system?
More in this TOC Section
Similar Articles

