


Abstract
ORGANIZED SCREENING HAS CONTRIBUTED TO A DECLINE in cervical cancer incidence and mortality over the past 50 years. However, women in developing countries are yet to profit extensively from the benefits of screening programs, and recent trends show a resurgence of the disease in developed countries. The past 2 decades have witnessed substantial progress in our understanding of the natural history of cervical cancer and in major treatment advances. Human papillomavirus (HPV) infection is now recognized as the main cause of cervical cancer, the role of coexisting factors is better understood, a new cytology reporting terminology has improved diagnosis and management of precursor lesions, and specific treatment protocols have increased survival among patients with early or advanced disease. Current research has focused on the determinants of infection with oncogenic HPV types, the assessment of prophylactic and therapeutic vaccines and the development of screening strategies incorporating HPV testing and other methods as adjunct to cytology. These are fundamental stepping stones for the implementation of effective public health programs aimed at the control of cervical cancer.
An estimated 371 000 new cases of invasive cervical cancer are diagnosed world wide each year, representing nearly 10% of all cancers in women. In frequency, it is the seventh cancer site overall and third among women, after breast and colorectal cancer.1 In developing countries, cervical cancer was the most frequent neoplastic disease among women until the early 1990s, when breast cancer became the predominant cancer site.2,3
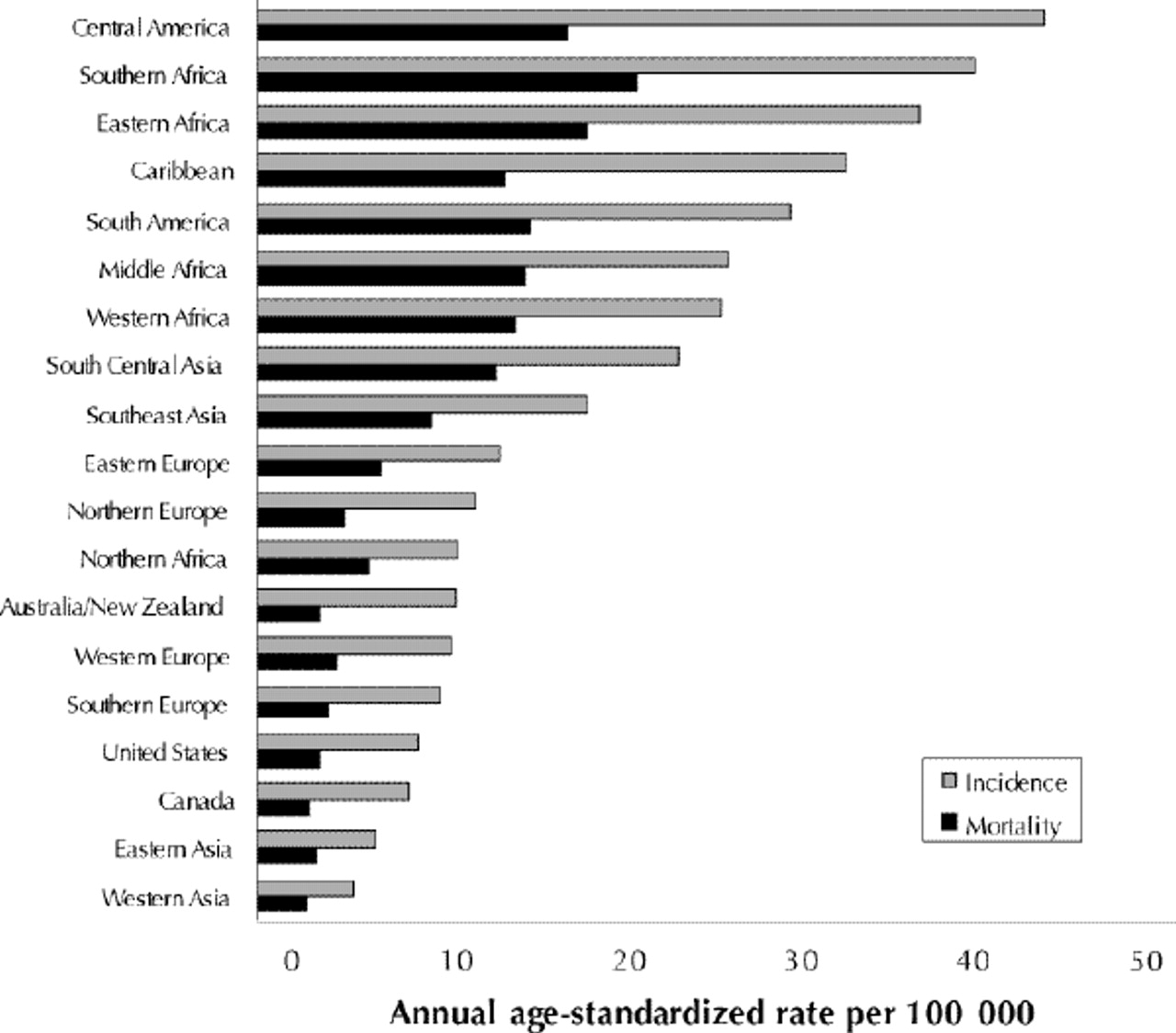
Fig. 1 shows age-standardized incidence and mortality rates for cervical cancer in Canada, the United States and the cancer surveillance regions of the World Health Organization (WHO). The highest risk areas are in Central and South America, southern and eastern Africa, and the Caribbean, with incidence rates of at least 30 new cases per 100 000 women per year. In general, there is a correlation between incidence and mortality across all regions, but some areas, such as Africa, seem to have a disproportionately higher mortality. Incidence and mortality rates in North America are relatively low. The mortality rate in Canada is the lowest among all regions.

Fig. 1: Annual incidence and mortality rates (per 100 000 women) of invasive cervical cancer in Canada, the United States and cancer surveillance regions of theWorld Health Organization. Rates are standardized according to age distribution of world population in 1960. Source: Ferlay et al.3
Table 1 shows Canada's incidence and mortality rates for cervical cancer (averages for latest 5-year reporting periods) and estimated numbers of new cases and deaths for 2000. Nearly 1500 new cases of cervical cancer were estimated to have been diagnosed in Canadian women in 2000, and an estimated 430 women died from the disease in the same year.4 The provinces with the highest incidence rates are Nova Scotia, Newfoundland and Prince Edward Island.
Table 1.
Cervical cancer takes a particularly heavy toll in North American Aboriginal, black and Hispanic populations. Among the Canadian Inuit, it accounts for nearly 15% of all cancers among women. The proportion is even greater among Aboriginal Canadians in Saskatchewan (29%), with an age-standardized rate 6 times higher than the national average.5
Incidence and mortality have declined in North America during the last 50 years because of increased availability of Papanicolaou smear screening programs and a decline in fertility rates over the last 4 decades. Fig. 2 shows the decline in age-standardized incidence and mortality rates in Canada since 1960. There is an indication that the marked declines seen until the mid-1980s have been slowing in recent years. This can be more easily seen by examining incidence rates by age in Canada and in the United States (Fig. 3). There seems to be a trend of increasing incidence during the last few years among white women less than 50 years old living in the United States in areas covered by the Statistics, Epidemiology, and End Results (SEER) program of the National Cancer Institute. This trend, suggestive of a resurgence in cervical cancer, has also been observed in many European countries and could reflect increased cancer detection by the use of new diagnostic techniques, such as human papillomavirus (HPV) testing and cervicography, or it could be the result of a cohort effect. Another factor potentially affecting incidence trends is the increase in rates of adenocarcinomas and adenosquamous carcinomas, which account for about 10% of all cervical cancers in Western populations.6,7

Fig. 3: Annual incidence rates (per 100 000 women) of invasive cervical cancer among women less than 50 years of age and among those 50 years or older in Canada (solid line) and in the United States (broken line). Rates are standardized according to age distribution of Canadian population in 1991. Source: Cancer Bureau, Population and Public Health Branch, Health Canada, and the National Cancer Institute Statistics, Epidemiology, and End Results (SEER) program.
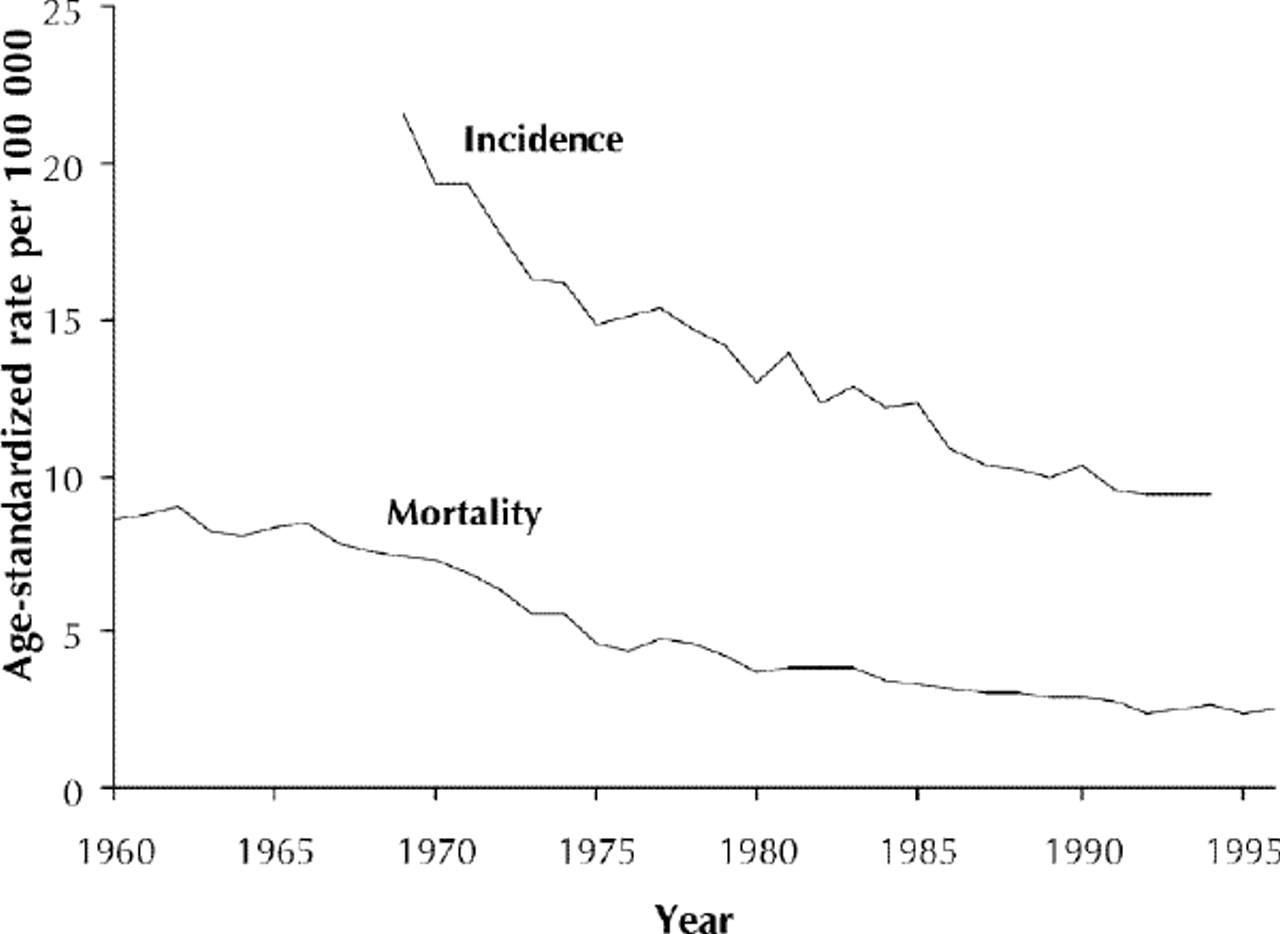
Fig. 2: Annual incidence and mortality rates (per 100 000 women) of invasive cervical cancer in Canada. Rates are standardized according to age distribution of Canadian population in 1991. Source: Cancer Bureau, Population and Public Health Branch, Health Canada.
Survival
Table 2 shows relative survival rates in some Canadian provinces, US populations and selected developed and developing countries. Patients diagnosed and treated in Canada have had somewhat better long-term (5-year) survival than those in the United States. Although survival among US women improved dramatically until the mid-1970s, these gains did not continue in recent years. Moreover, 5-year survival rates among black women have actually declined, widening the gap between races.
Table 2.
Ability to pay for health care could be a determinant for why survival rates differ substantially between white and black women in the United States and between the United States and Canada. A recent study comparing cancer survival between Detroit and Toronto revealed that socioeconomic status was associated with survival in Detroit but not in Toronto. Furthermore, survival among the poorest patients in Toronto was significantly better than that among the poorest ones in Detroit for most types of cancer, including cervical cancer.8
Risk factors
Epidemiological studies conducted during the past 30 years have consistently indicated that cervical cancer risk is strongly influenced by measures of sexual activity: number of sexual partners, age at first sexual intercourse and sexual behaviour of the woman's male partners.9,10 Circumstantial evidence for sexual transmission of an infectious agent comes from studies showing that wives of patients with penile cancer are at an increased risk of cervical cancer later in life.11 Such findings are further supported by results from correlation studies, in which strong associations were found between cervical and penile cancer mortality and incidence.12,13
Tobacco smoking has been a well-known risk factor for cervical cancer.14 A direct carcinogenic action of cigarette smoking on the cervix has been upheld on the grounds that nicotine metabolites can be found in the cervical mucus of women who smoke.15 Since smoking is associated with sexual behaviour, it is difficult to determine whether this association is spurious given the impossibility of effectively eliminating confounding through adjustment for measures of sexual activity.
The number of live births is a consistent risk factor for cervical cancer. There is a linear trend in the association between parity and risk, as seen in studies in North America and Central and South America.16 Apart from issues of screening coverage and quality, the high parity and deficient diets of women in developing nations may be contributory factors for the high incidence rates of cervical cancer observed in these regions.
There is an excess risk of cervical cancer associated with long-term use (12 years or more) of oral contraceptives. The association is somewhat stronger for adenocarcinomas than for squamous cell carcinomas.17 The association with oral contraceptive use observed in studies in which precancer was an outcome may have been due to detection bias, since women who use oral contraceptives undergo more frequent gynecological examinations, and are thus more likely to have disease detected early, than those who do not use them. The difficulty in properly assessing the effect of oral contraceptive use stems from the fact that this variable is highly associated with other risk factors, such as sexual activity and history of Pap smear screening.10
The evidence for an effect of diet on risk of cervical cancer indicates that a high intake of foods containing beta carotene and vitamin C and, to a lesser extent, vitamin A may reduce the risk of cervical cancer.18,19 The results from studies using diet recall methods have generally been corroborated by laboratory surveys assaying dietary constituents in plasma.20 As with reproductive factors, it is likely that diet may influence between-country differences in cervical cancer incidence rates.
HPV infection and cervical cancer
The WHO's International Agency for Research on Cancer (IARC) classified HPV infection as "carcinogenic" to humans (HPV types 16 and 18), "probably" carcinogenic (HPV types 31 and 33) and "possibly" carcinogenic (other HPV types except 6 and 11).23
Clinical and subclinical HPV infections are the most common STDs today. Asymptomatic cervical HPV infection can be detected in 5%-40% of women of reproductive age.24 HPV infection is a transient or intermittent phenomenon; only a small proportion of women positive for a given HPV type are found to have the same type in subsequent specimens.25,26 Risk of subsequent cervical intraepithelial neoplasia (CIN) is proportional to the number of specimens testing positive for HPV,27 which suggests that carcinogenic development results from persistent infections.
It is now well established that HPV infection is the central causal factor in cervical cancer.28,29 The thrust of epidemiological research in recent years has focused on the understanding of the role of risk factors that influence acquisition of persistent HPV infection or of coexisting factors that mediate progression in the continuum of lesion grades (Fig. 4).
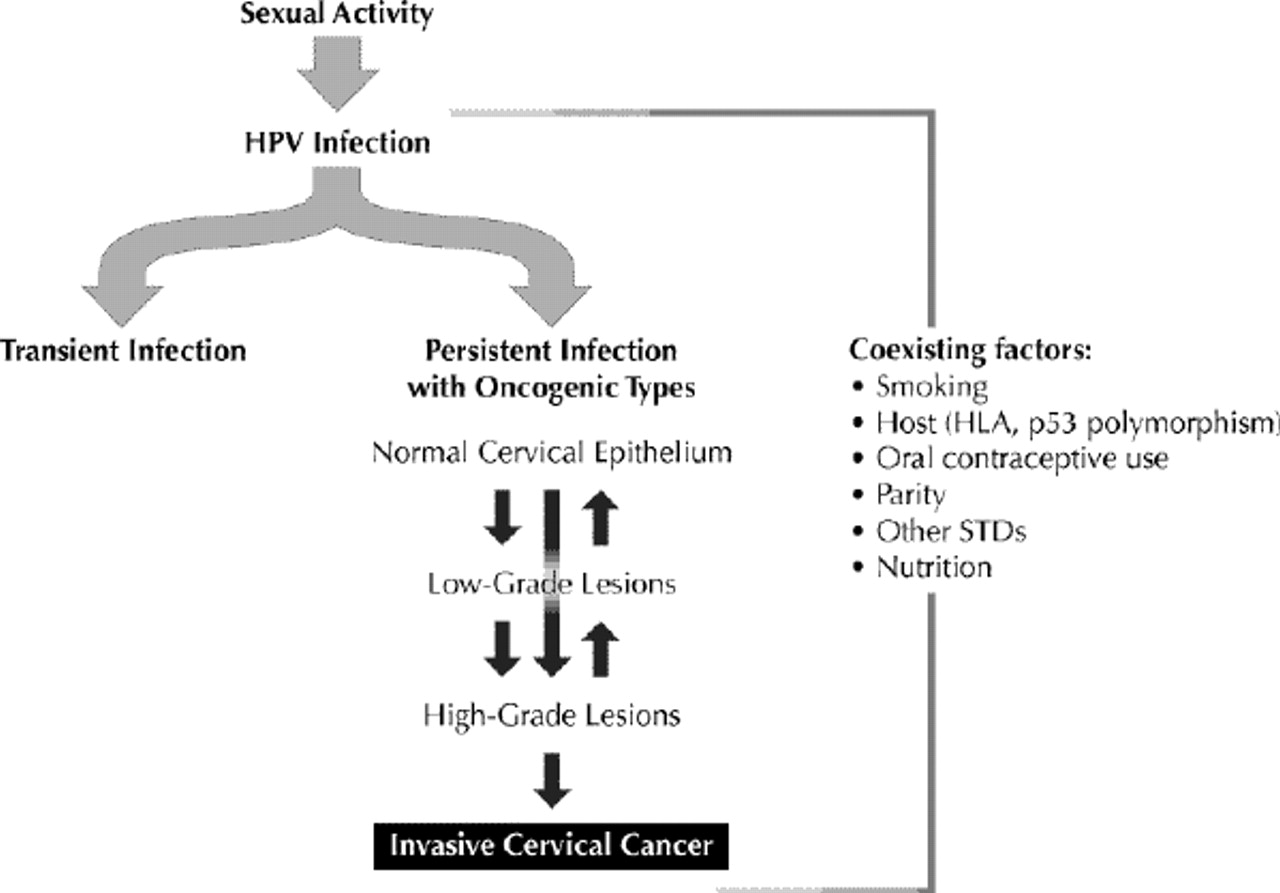
Fig. 4: Etiological model of human papillomavirus (HPV) infection and cervical cancer, illustrating probable role of remote behavioural risk factors for persistent infection and of coexisting factors that mediate lesion progression. Photo by: Lianne Friesen
The relative risks for the association between HPV infection and cervical neoplasia are of high magnitude, typically in the 20-70 range. This range is greater than that for the association between smoking and lung cancer and is comparable only to that of the association between chronic hepatitis B and liver cancer, causal relations that are undisputable.30 Recent evidence using meticulous testing by polymerase chain reaction of a large international collection of cervical cancer specimens has shown that HPV DNA is present in 99.7% of cases.22,31,32 This finding indicates that HPV infection could be a necessary cause of cervical neoplasia — the first instance in which this causal link would have been shown in cancer epidemiology — a realization that has obvious implications for primary and secondary prevention.33
Cytology screening
Despite its success, cytology has important limitations, false-negative results being the most important. Nearly half of specimens yield false-negative results; about one-third of these results are attributable to errors in interpreting slides and two-thirds to poor sample collection and slide preparation.34 The solution to minimize errors in cytology is to improve the quality of sample taking, slide processing and overall diagnostic performance of cervical cytology. False-negative results have important medical, financial and legal implications; the last is an acute problem in North America, where false-negative cytology specimens are a leading reason for medical malpractice litigation.
The Canadian Task Force on Preventive Health Care (formerly the Canadian Task Force on the Periodic Health Examination)35 and various consensus workshops36,37,38,39 have provided national recommendations that have been reaffirmed on separate occasions by provinces or by cancer prevention coalitions. The Cervical Cancer Prevention Network, which brings together federal and provincial representatives and clinical professional bodies, is the most important of these coalitions. This network spawned from a national workshop held in Ottawa in 1995 to identify barriers, needs and new directions in the development of organized cytology screening. The empirical basis for the soundness of these management guidelines was recently published.40
A new terminology for reporting results of cervical cytology — the Bethesda system — considers the information on HPV as part of the cytologic criteria to define lesion grade (Table 3). In addition, a new category for borderline lesions — atypical squamous cells of undetermined significance (ASCUS) — was created. These changes result in an increased proportion of low-grade lesions, which, combined with ASCUS, can account for up to 13% of smears in certain ethnic groups.42 On follow-up, most of these abnormalities revert to normal, and in some cases women have persistent minor grade lesion or hidden high-grade squamous intraepithelial lesion (HSIL) (20% of those with low-grade intraepithelial lesion [LSIL] and 10% of those with ASCUS).40 There is much debate over whether management of LSIL should be conservative or interventionist.43 The National Institutes of Health is conducting a large trial to assess whether HPV testing could improve the detection of missed HSIL among women with an initial diagnosis of ASCUS or LSIL.
Table 3.
HPV testing as an adjunct screening method
If HPV infection is an early precursor of cervical neoplasia, should HPV testing be used in screening for cervical cancer? Opponents to HPV testing have claimed that cytology screening alone has been very successful in decreasing invasive cervical cancer morbidity and mortality in many countries. An additional criticism is that HPV infection is highly prevalent among women of reproductive age and that it would be impractical to follow-up all positive cases. On the other hand, proponents of HPV testing claim that it would represent a scientifically sound approach for secondary prevention, particularly in developing countries, where high-quality cytology screening is difficult to implement, and that any pending issues could be evaluated by intervention trials. Consensus panels of the IARC and WHO have concluded that there is enough justification to evaluate HPV testing as an adjunct to Pap smear screening in cervical cancer.44,45
Treatment
Management options for LSIL (CIN grade 1) on histology vary widely across North America, ranging from simple observation to excisional therapies. Patients with persistent LSIL should be treated, chiefly with the use of office-based ablative therapies. Management guidelines for HSIL (CIN grade 2 or 3) are well established and recommend colposcopy-directed biopsy with or without endocervical curettage. Cold-knife conization or electroconization should be performed in all patients with biopsy-confirmed HSIL in order to exclude invasive disease.
In women with invasive cancer, additional tests are required to establish the stage of the disease. Treatment depends primarily on the extent of the lesion, but it also depends on factors such as the patient's age, her desire to preserve fertility and the presence of other medical conditions.46 Virtually all patients with stage IA disease are cured with either simple hysterectomy or, if fertility preservation is desired, by conization if margins are free of disease. For women with stage IB disease without involvement of the lymph nodes, prognosis is best after radical hysterectomy. Recent randomized phase III trials involving women with stage IB or stage II disease and metastatic pelvic node involvement demonstrated significant survival benefits for the combined use of cisplatin chemotherapy and radiation at the time of primary surgery, with a reduction in risk of death of 30%-50%.47,48,49 More advanced clinical stages are associated with relatively lower survival rates, even after radiation or chemotherapy, or both.
Current and future research
Recognition that HPV infection is the central cause of cervical neoplasia has created new research fronts in primary and secondary prevention of this disease.
Primary prevention of cervical cancer can be achieved through prevention and control of genital HPV infection. Health promotion strategies geared at a change in sexual behaviour targeting all STDs of public health significance can be effective in preventing genital HPV infection.50 Although there is consensus that symptomatic HPV infection (genital warts) should be managed by way of treatment, counselling and partner notification, active case-finding of asymptomatic HPV infection is currently not recommended as a control measure. Further research is needed to determine the effectiveness of such a strategy.
Vaccination against HPV may have greatest value in developing countries, where 80% of the global burden of cervical cancer occurs each year and where Pap screening programs have been largely ineffective. Two main types of vaccine are currently being developed: prophylactic vaccines to prevent HPV infection and consequently the various HPV-associated diseases, and therapeutic vaccines to induce regression of precancerous lesions or remission of advanced cervical cancer.
DNA-free virus-like particles synthesized by self-assembly of fusion proteins of the major capsid antigen L1 have been found to induce a strong humoral response with neutralizing antibodies. These virus-like particles are thus the best candidate immunogen for HPV vaccine trials. Protection seems to be type specific, which will require the production of virus-like particles for a variety of oncogenic types. Such vaccines are already being evaluated in phase I and II trials in different populations.
Organized cytology screening programs have been successful in developed countries, but in developing countries these programs lack coverage, accessibility, effectiveness and acceptability — conditions that are not likely to change soon because of competing public health priorities. General improvement in socioeconomic status and educational level of the population tends to have a positive effect on the risk of cervical cancer by altering some of the known risk factors such as age at marriage, parity and health-care seeking behaviour. Other strategies such as low-intensity cytology screening (e.g., 1 Pap smear every 10 years after age 35) and visual inspection need to be better evaluated in randomized controlled trials to determine their cost-effectiveness.54
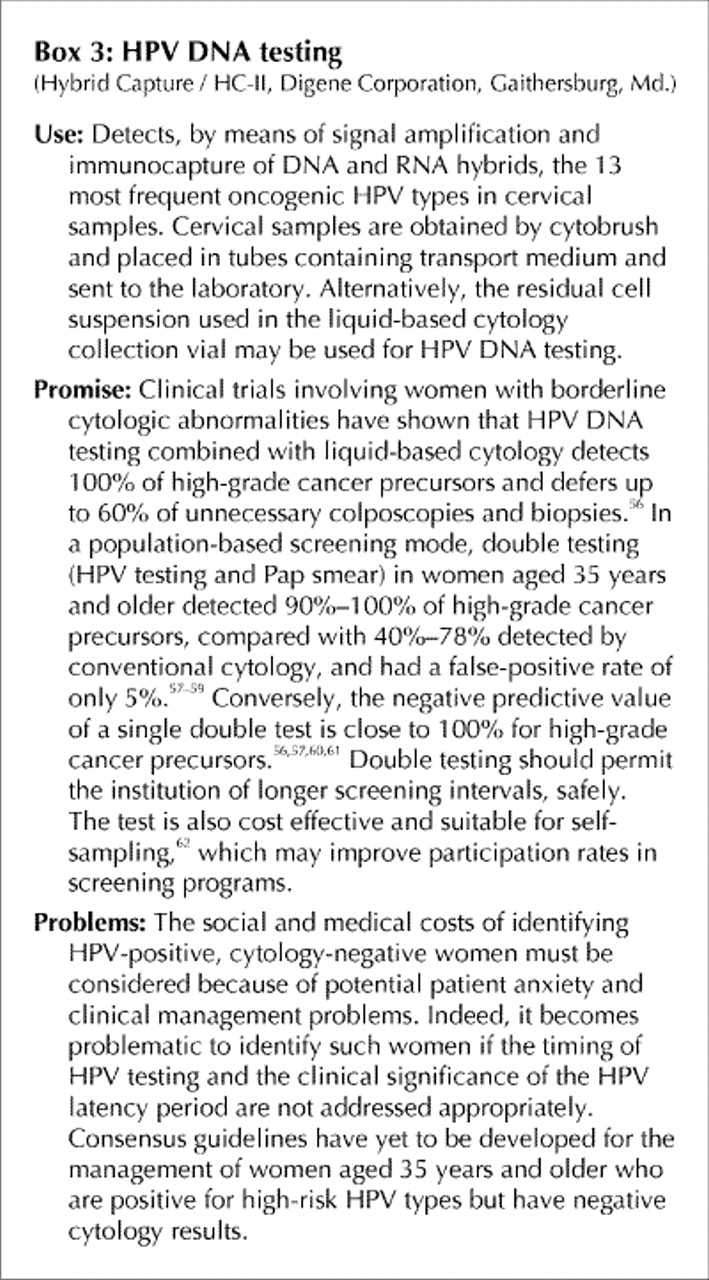
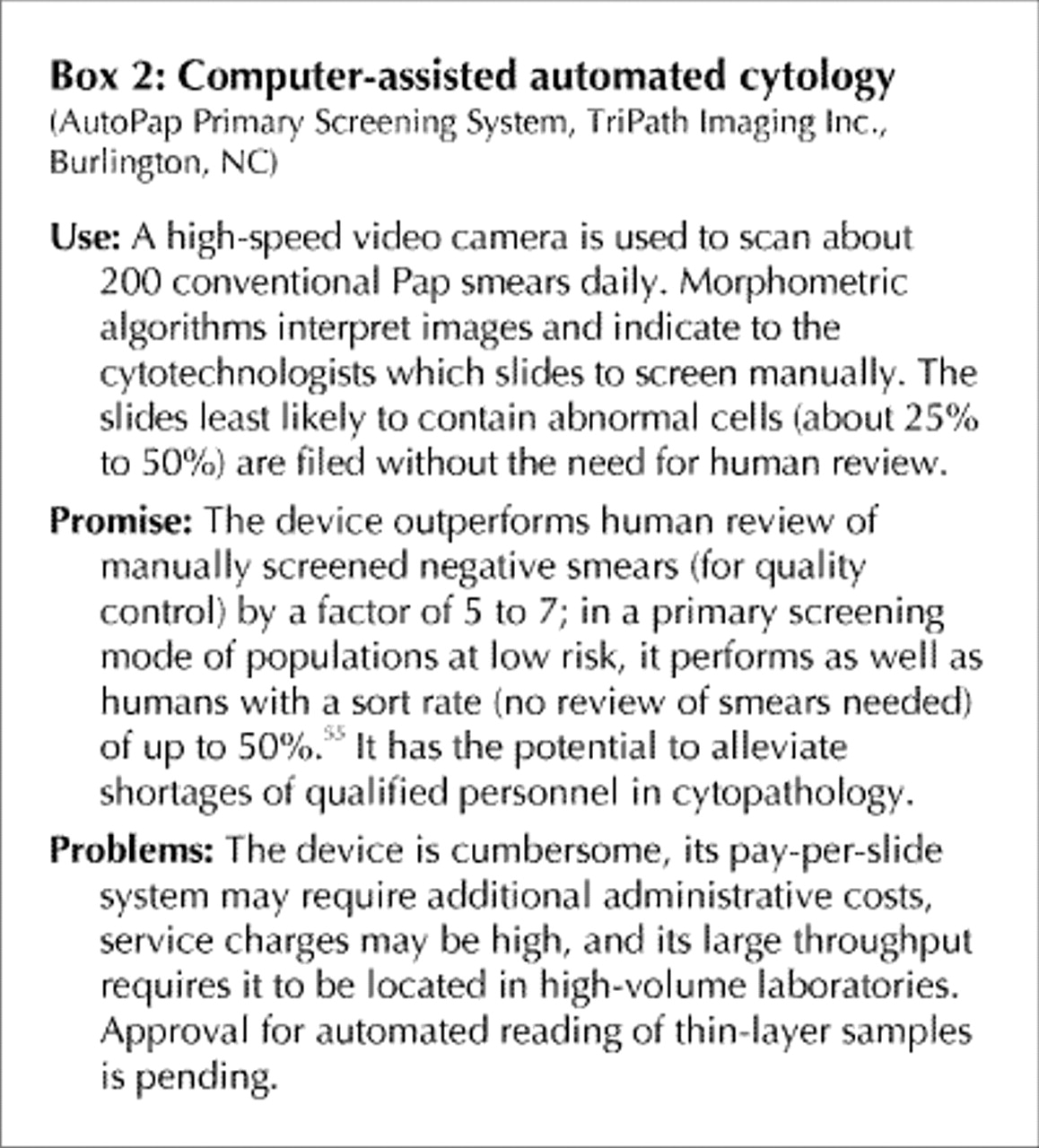
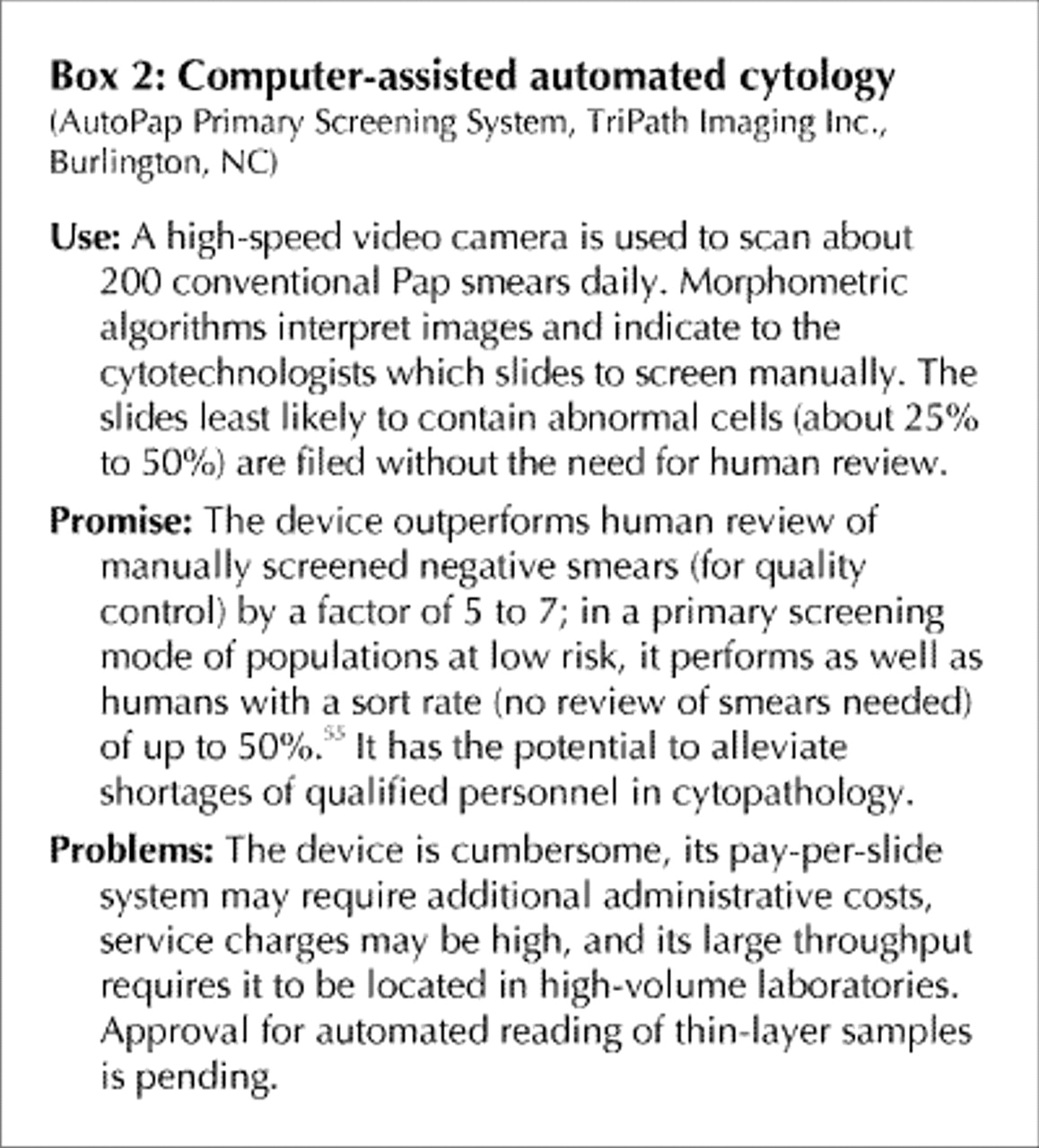
In recent years, 3 new laboratory tests have been developed for primary and secondary screening for cervical cancer and its precursors (Boxes 1, 2 and 3). These are thin-layer liquid-based cytology, HPV DNA testing and computer-assisted automated cytology. All have been approved by the US Food and Drug Administration for clinical use and by Health Canada.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Although there is enthusiasm concerning the possible application of HPV testing as an adjunct to Pap screening, there are several problems that need to be solved before any secondary prevention programs can be augmented. Ongoing research on the epidemiology of viral persistence will help to determine the utility of HPV testing as a screening tool for cervical cancer.
Factors influencing the magnitude of survival rates in different populations
-
Relative proportions of patients with advanced versus early-stage disease.
-
Age distribution of the cohort of patients.
-
Access to surgery, radiation therapy and chemotherapy.
-
These 3 factors, particularly the first and third, are strongly correlated with socioeconomic status. Patients of lower economic means will have their diagnosis delayed, which may lead to more advanced disease at the time of treatment and consequently to poorer survival.
Human papillomaviruses
-
The epithelial lining of the anogenital tract is the target for infection by a group of mucosotropic viruses, the human papillomaviruses (HPVs).
-
Subclinical and clinical genital warts, also known as condylomata acuminata, and virtually all squamous cell cancers of the anogenital tract are caused by specific HPV types.
-
HPVs are DNA viruses with a genome size of about 8000 base-pairs.
-
There are more than 100 HPV types defined on the basis of DNA homology, of which more than 40 infect the anogenital tract.
-
Genital HPV types are typically divided into groups according to their presumed oncogenic potential.21,22
-
HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68 are considered to be of oncogenic risk.
-
The remaining genital types — types 6, 11, 42, 43 and 44 — are considered of low or no oncogenic risk.
Evidence for efficacy of Pap smear screening
-
There have been no controlled trials, randomized or otherwise, of the screening efficacy of the Pap test in cervical cancer. The evidence for its efficacy comes from 3 sources:
-
· Epidemiologic studies, indicating that the risk of invasive cervical cancer is 2-10 times greater among women who have not been screened and that the risk increases with time since the last normal smear or with lower frequency of screening.
-
· Surveillance statistics from different regions, indicating that cervical cancer incidence and mortality have decreased sharply following the introduction of screening in Scandinavian countries, Canada and in the United States, with reductions in incidence and mortality being proportional to the coverage of the screening programs.
-
· Multiple national and international consensus panels.
37
-
Pap screening is to begin at age 18 or at initiation of sexual activity and to continue annually.
-
After 2 negative consecutive results, 1 year apart, Pap screening is to proceed every 3 years to age 69.
-
This frequency of screening should be used in areas where a population-based information system exists for identifying the clientele and allowing rapid case notification and recall. In the absence of such a system it is advisable to repeat Pap smears annually.
-
If mild dysplasia (cytologic equivalent of cervical intraepithelial neoplasia [CIN] grade 1, or low-grade squamous intraepithelial lesion [SIL]) is found, the smear is to be repeated every 6 months for 2 years.
-
If the lesion persists or progresses to moderate or severe dysplasia (CIN grades 2 and 3, respectively, or high-grade SIL) the patient must be referred for colposcopy.
-
Refer for immediate colposcopy all initial cases of moderate dysplasia or worse lesions.
-
Cytologic evidence of HPV infection in the smear per se should not guide management.
41
-
Refinement of diagnostic methods.
-
Precise definition of HPV incidence in the population.
-
Assessment of risks associated with certain HPV genotypes for cancer progression.
-
Identification of coexisting factors influencing HPV transmission and carcinogenesis.
-
Treatment of HPV infection.
-
Development of vaccines.
-
Assessment of efficacy and cost-effectiveness of screening for HPV infection.
Acknowledgments
We are indebted to Adam Probert, Cancer Bureau, Population and Public Health Branch, Health Canada, for providing timely health statistics for Canadian provinces that were used in preparing the information given in this article.
Footnotes
-
Portions of this manuscript are to appear as a chapter about cervical cancer in the Women's Information Monograph, to be published by the Cancer Bureau, Population and Public Health Branch, Ottawa, Ont.
This article has been peer reviewed.
Contributors: All of the authors contributed equally in the review of the literature and in the writing and revising of this article.
Competing interests: None declared for Eliane Duarte-Franco. Eduardo Franco has received consultancy fees from Cytyc Canada Ltd. for work related to this field. Alex Ferenczy has received honoraria from Cytyc Canada Ltd. and Digene Corporation for research related to this field as well as speaker fees and travel assistance from these companies for various meetings.
Reprint requests to: Prof. Eduardo Franco, Department of Oncology, McGill University, 546 Pine Ave. W, Montreal QC H2W 1S6; fax 514 398-5002
References
In this issue
Article tools






Jump to section
Related Articles
Cited By...
- Predictors of High-grade Squamous Intraepithelial Lesion treatment failure
- Primary care provider interventions for addressing cancer screening participation with marginalised patients: a scoping review protocol
- Joint modeling HIV and HPV using a new hybrid agent-based network and compartmental simulation technique
- Characteristics of patients diagnosed with cervical cancer in Brazil: preliminary results of the prospective cohort EVITA study (EVA001/LACOG 0215)
- The epidemiology and direct medical costs of diseases associated with human papillomavirus infection among men in Manitoba, Canada
- Cervical Abnormalities in South African Women Living With HIV With High Screening and Referral Rates
- Sociodemographic Inequalities in Sexual Activity and Cervical Cancer Screening: Implications for the Success of Human Papillomavirus Vaccination
- Recommendations on screening for cervical cancer
- Comparison of the Hybrid Capture 2 and cobas 4800 Tests for Detection of High-Risk Human Papillomavirus in Specimens Collected in PreservCyt Medium
- Is unhealthy substance use associated with failure to receive cancer screening and flu vaccination? A retrospective cross-sectional study
- Are women with psychosis receiving adequate cervical cancer screening?
- Diagnostic accuracy of self collected vaginal specimens for human papillomavirus compared to clinician collected human papillomavirus specimens: a meta-analysis
- Human papillomavirus and HIV coinfection and the risk of neoplasias of the lower genital tract: a review of recent developments
- Role of the human papilloma virus in the development of cervical intraepithelial neoplasia and malignancy
- The causal relation between human papillomavirus and cervical cancer
- The merits of new alternatives to the Papanicolaou test
- The merits of new alternatives to the Papanicolaou test
More in this TOC Section
Similar Articles

