


- © 2007 Canadian Medical Association or its licensors
Abstract
Background: Previous studies have suggested that a patient's sex may influence the provision and outcomes of critical care. Our objective was to determine whether sex and age are associated with differences in admission practices, processes of care and clinical outcomes for critically ill patients.
Methods: We used a retrospective cohort of 466 792 patients, including 24 778 critically ill patients, admitted consecutively to adult hospitals in Ontario between Jan. 1, 2001, and Dec. 31, 2002. We measured associations between sex and age and admission to the intensive care unit (ICU); use of mechanical ventilation, dialysis or pulmonary artery catheterization; length of stay in the ICU and hospital; and death in the ICU, hospital and 1 year after admission.
Results: Of the 466 792 patients admitted to hospital, more were women than men (57.0% v. 43.0% for all admissions, p < 0.001; 50.1% v. 49.9% for nonobstetric admissions, p < 0.001). However, fewer women than men were admitted to ICUs (39.9% v. 60.1%, p < 0.001); this difference was most pronounced among older patients (age ≥ 50 years). After adjustment for admission diagnoses and comorbidities, older women were less likely than older men to receive care in an ICU setting (odds ratio [OR] 0.68, 95% confidence interval [CI] 0.66–0.71). After adjustment for illness severity, older women were also less likely than older men to receive mechanical ventilation (OR 0.91, 95% CI 0.81–0.97) or pulmonary artery catheterization (OR 0.80, 95% CI 0.73–0.88). Despite older men and women having similar severity of illness on ICU admission, women received ICU care for a slightly shorter duration yet had a longer length of stay in hospital (mean 18.3 v. 16.9 days; p = 0.006). After adjustment for differences in comorbidities, source of admission, ICU admission diagnosis and illness severity, older women had a slightly greater risk of death in the ICU (hazard ratio 1.20, 95% CI 1.10–1.31) and in hospital (hazard ratio 1.08, 95% CI 1.00–1.16) than did older men.
Interpretation: Among patients 50 years or older, women appear less likely than men to be admitted to an ICU and to receive selected life-supporting treatments and more likely than men to die after critical illness. Differences in presentation of critical illness, decision-making or unmeasured confounding factors may contribute to these findings.
It is generally believed that access to an intensive care unit (ICU), the care received and subsequent clinical outcomes are determined primarily by need and severity of illness. However, in other areas of health care, sociodemographic characteristics have been found to influence treatment decisions and care delivery.1–6 For example, women are believed to have a lower incidence of coronary artery disease than men;2 however, they are also less likely to undergo intensive evaluation and treatment for this condition and may have a higher rate of early mortality after acute myocardial infarction.7,8 Previous studies from various jurisdictions have suggested that there may be sex-based differences in critical illness and ICU admission patterns,3,4,6,9 although there have been no consistent findings of sex-based differences in the provision of care or clinical outcomes.1,3,4,6,10–12
The Canadian health care system is based on the principle of equal access for all citizens. This presents a unique opportunity to explore sex-related differences in ICU care. We hypothesized that age and sex might be associated with differences in admission practices, processes of care and clinical outcomes for critically ill patients, and we explored these relations over a 2-year period in a diverse sample of hospitals in Ontario.
Methods
Study population
We obtained data on admission demographics, process of care and outcomes from hospitals and ICUs that are part of the Canadian Critical Care Research Network (CCRNet), a collaboration of urban and nonurban primary, secondary and tertiary care facilities.13 This database provided information on all patients admitted to adult ICUs in study hospitals from Jan. 1, 2001, to Dec. 31, 2002. We chose this 2-year period to minimize effects of seasonal variation in disease patterns and longer-term temporal trends and to allow sufficient follow-up. We restricted our cohort to Ontario hospitals to be able to merge the data set with other administrative databases. Of 13 participating centres, 4 were teaching and 9 were community hospitals. The median number of ICU beds was 14 (range 6–30); the median number of hospital beds was 361 (range 177–600).
Information was collected by trained data abstractors, entered into an electronic database and stored in a central repository. All data were examined for accuracy and completeness and were subjected to an iterative process of reconfirmation that has been found to have high interobserver reliability and validity.14
The research ethics board of the Sunnybrook Health Sciences Centre approved this study.
Data collection
We collected data on demographic and physical characteristics (sex, age, height, weight); medical, surgical and specific diagnoses and comorbid conditions (based on International Classification of Diseases, 9th or 10th revision, codes), from which the Deyo adaptation of the Charlson Comorbidity Index15 was calculated; diagnosis on ICU admission; source of ICU admission (e.g., emergency department, operating room, ward, other hospital); acute care variables necessary for the calculation of the APACHE (Acute Physiologic And Chronic Health Evaluation) II and III scores, which indicate severity of illness;16 duration of ICU and hospital stay; and survival status at ICU and hospital discharge. We included patients admitted more than once in the analyses by adjusting for non-independence of observations.
To evaluate critical care provided and to determine long-term health outcomes, we linked each patient's record in the Canadian Critical Care Research Network with 3 population-based administrative databases. The Canadian Institute for Health Information database includes detailed diagnostic and demographic information on all hospital admissions. The Ontario Health Insurance Program database includes billing claims from physicians for such procedures as hemodialysis, pulmonary artery catheterization and mechanical ventilation. Finally, the Registered Persons Database includes demographic and vital statistics on all Ontario residents ever issued a health card. These databases are routinely combined using encrypted health card numbers to study outcomes at the patient level.10,12 We successfully linked these data sets for 21 225 (85.7%) of the critically ill patients in our cohort. There were no substantial differences in the proportion of women and men between the linked (40% women, 60% men) and unlinked (41% women, 59% men) records. Because catchment areas for each study hospital and the corresponding population size and sex distribution are not fixed, we chose to adjust for the known sex-specific population differences in the overall Ontario population and expressed admission rates as per 100 000 of the Ontario population, by sex and age decade.
Statistical analysis
We compared characteristics of patients using Student's t test and the χ2 test. We used multiple logistic regression analysis to examine the relation between sex and admission to the ICU, with adjustment for Charlson Comorbidity Index score, source of ICU admission and diagnosis on ICU admission. We also examined the relation between sex and technological care received (newly instituted mechanical ventilation, pulmonary artery catheterization or hemodialysis), with adjustment for APACHE III score and diagnosis on ICU admission. We used proportional hazards modelling to examine the relation between sex and mortality during ICU and hospital stay and up to 1 year after admission, with adjustment for Charlson Comorbidity Index score, diagnosis on ICU admission, source of ICU admission and APACHE III score. We examined predictor variables and potential confounders for multicollinearity using a correlation matrix to ensure no correlations above 0.80. We confirmed proportional hazards assumptions using log–log survival curves and a goodness-of-fit test. We followed the common practice of considering no more than 1 independent variable for every 10 patients who experienced an event of interest.17 We limited our comparisons to the a priori specified explanatory variables of sex and specific potential confounders or effect modifiers, including age (≥ 50 or < 50 years, which is approximately the mean age of menopause in Canada and corresponds to age groupings in other studies),4 diagnosis on ICU admission, source of ICU admission, Charlson Comorbidity Index score and APACHE III score. All statistical tests were 2-tailed, and we used a p value of 0.05 as the threshold for statistical significance.
Results
Study population
Between Jan. 1, 2001, and Dec. 31, 2002, 466 792 patients were admitted to the study hospitals. Overall, 57.1% of the patients were women and 42.9% were men (p < 0.001) (Table 1). Medical diagnoses accounted for 57.2% of the admissions, surgical diagnoses for 28.8% and obstetric diagnoses for 14.0%. Of the patients admitted for nonobstetric reasons, 50.1% were women and 49.9% men (p < 0.001). The mean age of the patients admitted to hospital was 44.2 (standard deviation [SD] 35.0) years. We observed a greater number of admissions involving women than men among patients 50 years or older.
Table 1.
Admissions to intensive care units
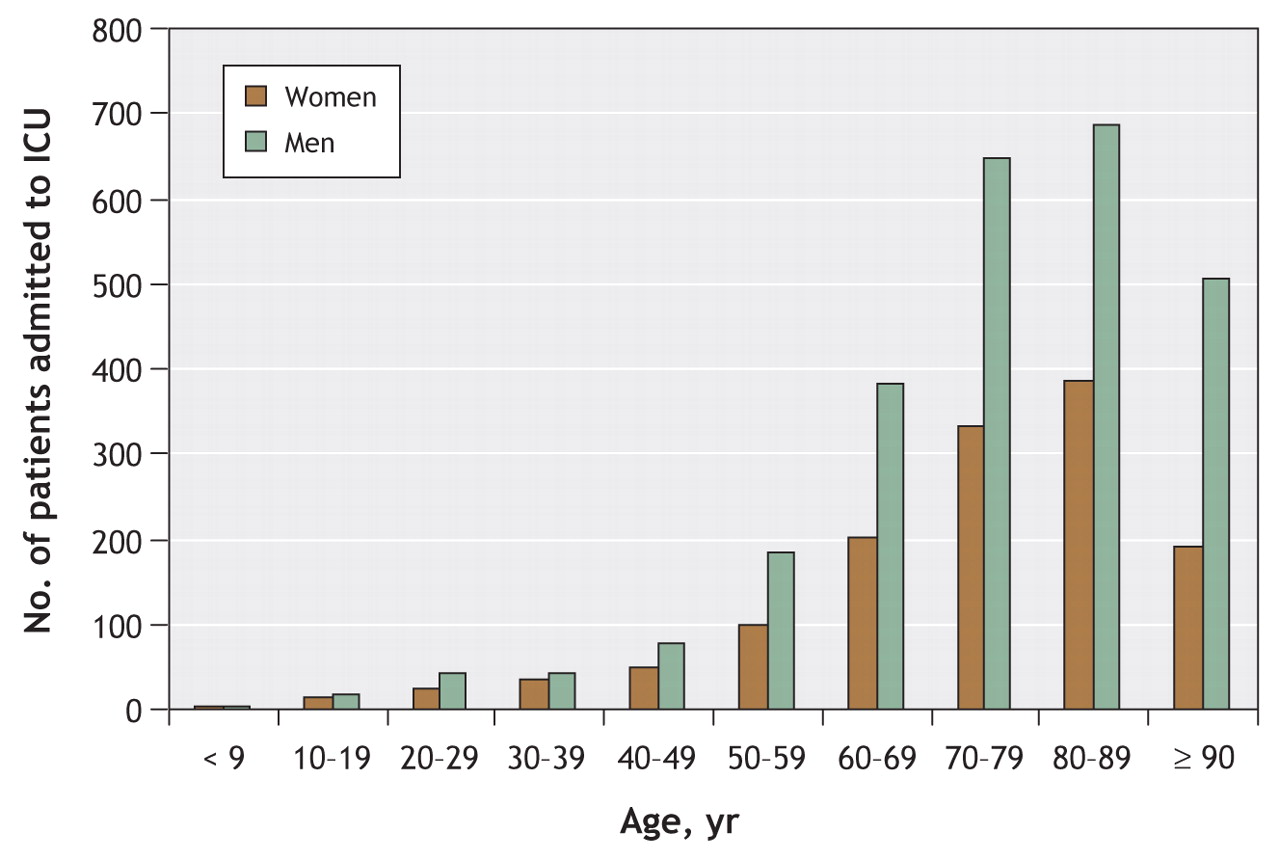
There were 24 778 consecutive admissions to ICUs during the study period. At the time of hospital admission, the mean Charlson Comorbidity Index score was the same for men and women (Table 2). Although men accounted for about half (49.9%) of the nonobstetric hospital admissions, they accounted for 60.1% of the admissions to ICUs. This difference was more pronounced with increasing age (Figure 1).
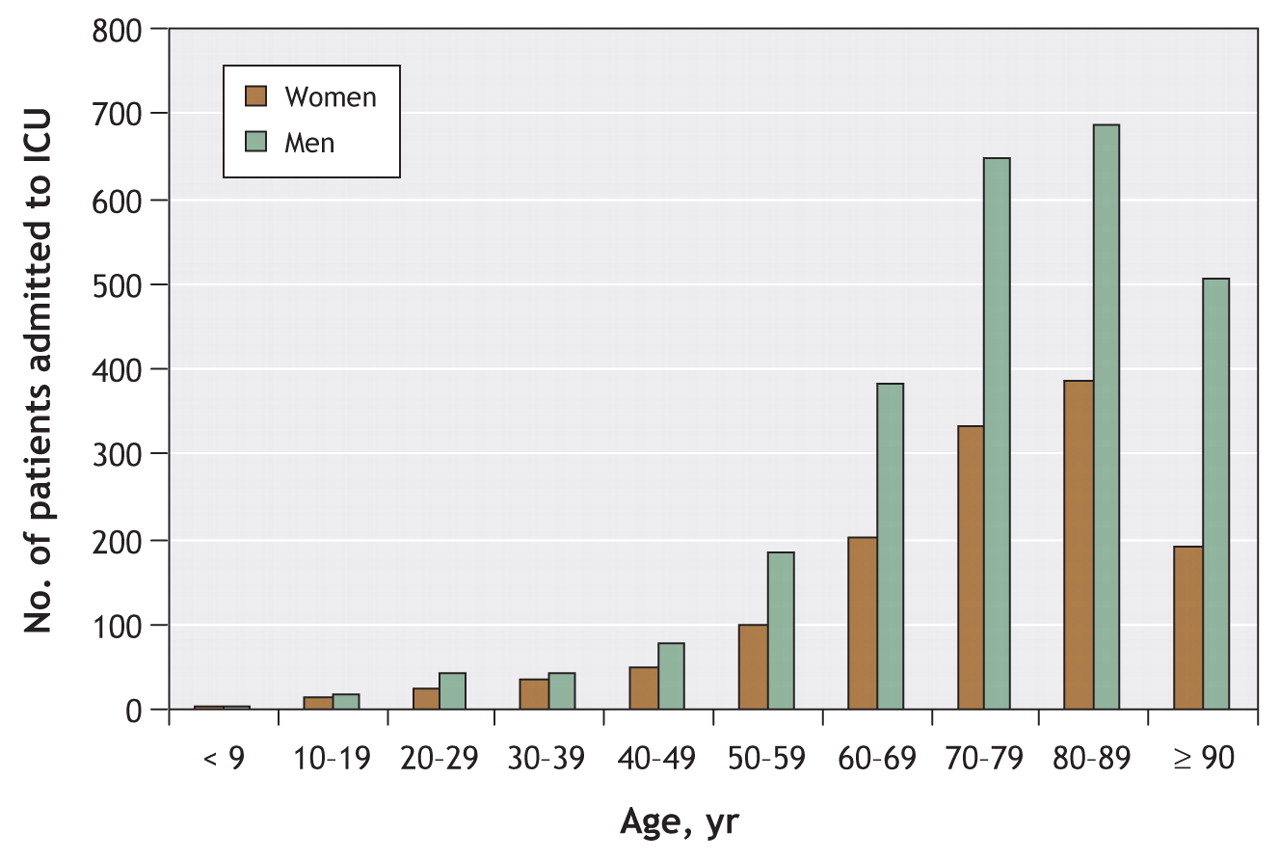
Figure 1: Age and sex distribution of 24 778 patients admitted to intensive care units at study hospitals in Ontario between Jan. 1, 2000, and Dec. 31, 2001. Figures were adjusted for known sex-specific population differences in the overall Ontario population and are expressed as admission rates per 100 000 of the Ontario population, by sex and age decade.
Table 2.
At the time of ICU admission, the male and female patients were of comparable age and had similar severity of illness, as measured by the APACHE II and III scores (Table 2). Compared with men, women were more frequently admitted to ICU from an emergency department, hospital ward or other hospital. A higher proportion of women than of men were admitted because of a medical illness; the reverse was true for admissions after elective surgery, with more men than women being admitted.
Although the proportion of admissions due to specific diagnoses varied according to sex, greater numbers of men than of women were admitted to an ICU with a medical diagnosis or a nonobstetric surgical diagnosis (Table 2). After adjusting for Charlson Comorbidity Index score, source of ICU admission, medical or surgical diagnosis and each of the 50 most common diagnoses for hospital admission, we found that older women (age 50 years or more) were significantly less likely than older men to be admitted to an ICU (odds ratio [OR] 0.68, 95% confidence interval [CI] 0.66–0.71; p < 0.001). This finding persisted after we excluded patients with an obstetric–gynecologic diagnosis.
Diagnostic and therapeutic services provided
We found that significantly more critically ill men than women received mechanical ventilation (57.8% v. 52.3%; p < 0.001) and pulmonary artery catheterization (29.8% v. 20.3%; p < 0.001); we found no significant difference for hemodialysis (Table 3). These findings persisted after we adjusted for severity of illness by APACHE III score (odds of women receiving mechanical ventilation: OR 0.91, 95% CI 0.81–0.97, p = 0.005; pulmonary artery catheterization: OR 0.80, 95% CI 0.73–0.88, p < 0.001; and hemodialysis: OR 0.87, 95% CI 0.67–1.12, p = 0.28). Similar differences were found for both medical and surgical diagnoses and among both teaching and community hospitals. Because the differences may have been due to sex-discrepant practices of a small number of high-volume centres, we compared procedure rates between men and women at centres with high and low volumes but found generally consistent patterns.
Table 3.
Clinical outcomes
Despite men and women 50 years or older having similar severity of illness on ICU admission, women received ICU care for a slightly shorter duration yet had a longer length of stay in hospital (mean 18.3 v. 16.9 days; p = 0.006) (Table 4).
Table 4.
Among all of the patients admitted to hospital, we found that the in-hospital and 1-year rates of death were slightly yet significantly higher among men than among women (Table 4). However, among critically ill patients, we observed the opposite: despite critically ill men and women 50 years or older having similar severity of illness, mortality was higher among women than among men in the ICU (15.4% v. 12.7%; p < 0.001) and in hospital (22.3% v. 18.9%; p < 0.001) (Table 4). When we examined mortality by age decade and by 20-year increments, we also found that mortality was significantly higher among critically ill older women than men (see Appendix 1). Mortality did not differ significantly between younger critically ill women and men. We were able to determine the 1-year mortality for 85.7% of the critically ill patients: it remained higher among women than among men (28.6% v. 25.2%; p < 0.001) at 12 months after admission to ICU owing to a significantly higher rate of death among older women than among older men (Table 4, Appendix 1).
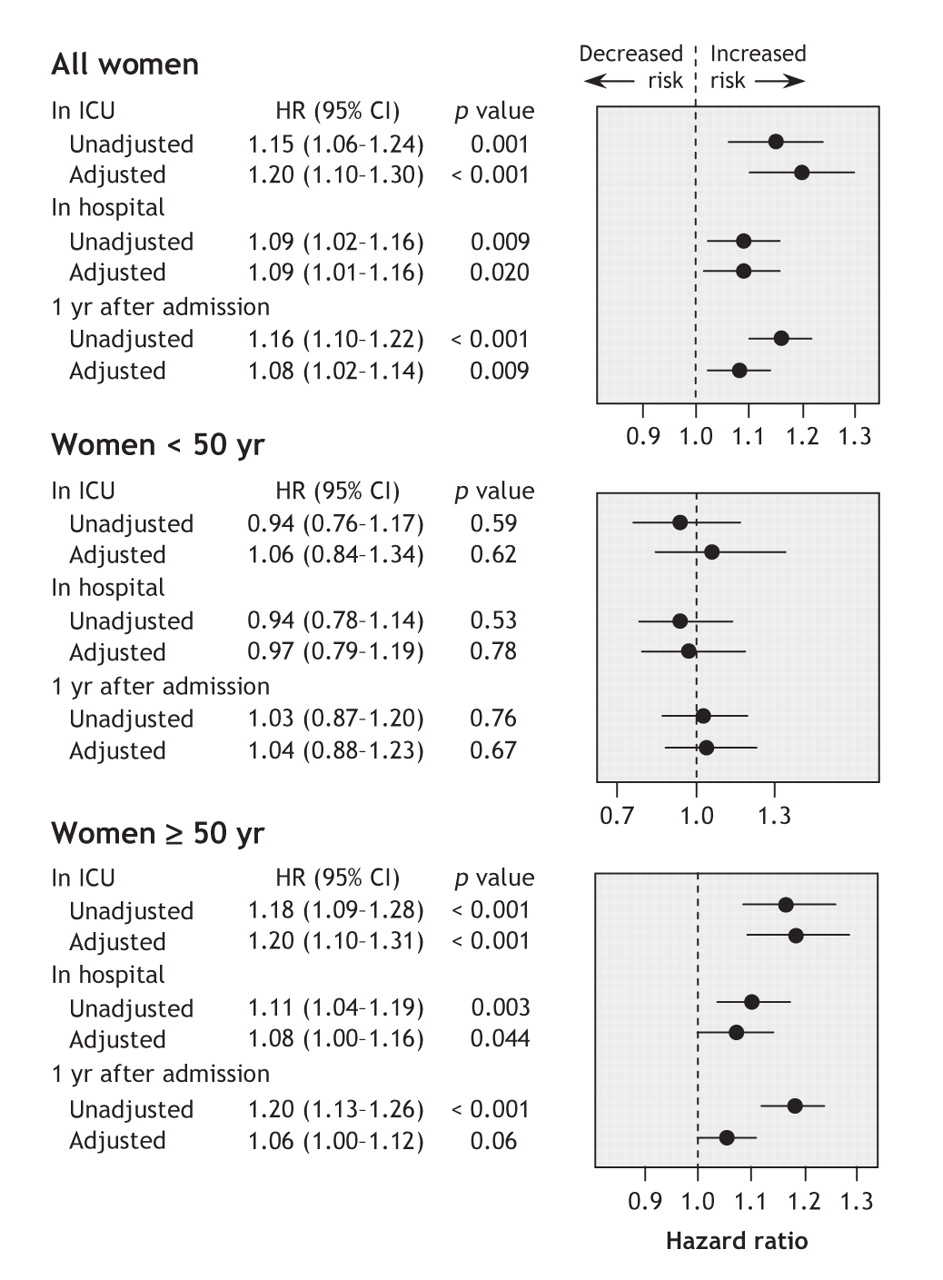
To investigate how sex-related differences might depend on age, we prospectively chose a cutoff for age of 50 years. We found that there was an interaction between age and sex and that the chosen cutoff for age was appropriate, since differences generally increased after this age. A multiple logistic regression model that had in-ICU death as the outcome and included age, sex, APACHE III score (severity of illness) and all 2-way interactions revealed an expected interaction between age and severity of illness (p = 0.002). Therefore, we used separate models for patients less than 50 years old and those 50 years or older. We used proportional hazards modelling to examine the relation between sex and time to death, adjusting for APACHE III score, Charlson Comorbidity Index score, each of the 50 most common diagnoses and source of ICU admission. We found no effect of sex among patients less than 50 years. However, after adjusting for all other factors, we found a significant effect (p < 0.001) among older patients (Figure 2). Among older patients, being female was associated with a 20% increased risk of death in ICU (hazard ratio [HR] 1.20, 95% CI 1.10–1.31), an 8% increased risk of death in hospital (HR 1.08, 95% CI 1.00–1.16) and a 6% (nonsignificant) increased risk of death over 1 year (HR 1.06, 95% CI 1.00–1.12).

Figure 2: Unadjusted and adjusted hazard ratios for risk of death among critically ill women (v. men) admitted to intensive care units (ICUs). (Adjustments were for Charlson Comorbidity Index score, APACHE III score [severity of illness], source of ICU admission and diagnosis on ICU admission.)
Interpretation
In this large cohort of patients admitted to hospitals and ICUs in Ontario over a 2-year period, we found sex-and age-related differences in admissions to ICU and receipt of specific life-supporting interventions, as well as in short-and long-term outcomes. Women represented more than half of the patients admitted to hospital during the study period, a distribution similar to that of patients admitted to all Canadian hospitals during 2000–2001 (58.0% v. 42.0%).18,19 The distribution of women and men admitted for nonobstetric reasons corresponded to the slight predominance of women in the Ontario (51.1%) and Canadian (51.0%) general populations during 2001.20 As well, the greater number of women than men among patients 50 years or older who were admitted to hospital corresponded to the slight female predominance in the general population that increases with age and to the proportion of patients admitted to other Canadian hospitals who were 50 years or older.18
However, despite more women than men 50 years or older being admitted to hospital, women were significantly less likely than men to receive care in an ICU. Moreover, although men and women had similar severity of illness at the time of ICU admission, women were less likely than men to receive mechanical ventilation and pulmonary artery catheterization for medical and surgical diagnoses. In addition, we found that, after adjusting for comorbidities, diagnosis on ICU admission and severity of illness, the rates of death in ICU and in hospital were higher among critically ill women 50 years or older than among their male counterparts.
As age increased, men were increasingly more likely than women to be admitted to ICU regardless of whether their diagnosis was medical or surgical and despite the fact that there are more women in the general population, that more women than men were admitted to the study hospitals and that severity of illness at the time of ICU admission was similar for men and women. This difference might be because in-hospital illness progresses differently for men and women. Although we accounted for the 50 most common diagnoses for hospital admission and used a well-validated comorbidity index to account for the possibility of different comorbidity-based severity of illness at the time of hospital admission, we found that older men were still more likely than older women to be admitted to an ICU. This makes any sex-related differences in population-based disease prevalence less likely to be the sole explanation for our findings. Other epidemiologic studies have observed similar sex-related differences.3,4,21
Our finding that critically ill women were less likely than critically ill men to receive mechanical ventilation and pulmonary artery catheterization is consistent with findings from other studies that showed men being more likely than women to receive invasive therapies.1,3 Although we found that men with acute renal failure more commonly received hemodialysis than did women, the difference was not significant. Similar observations have been reported in other acute care populations.5
Older men are known to have a higher risk of death than older women after admission to hospital.22 However, we found the opposite among critically ill patients: older women who were critically ill were more likely to die than critically ill men of similar age. This age–sex relation is consistent with findings from smaller studies.4,23 In previous studies, sex-related differences in outcomes among critically ill patients receiving mechanical ventilation were attenuated after adjustment for severity of illness;3,24 however, we found important residual sex-and age-related associations after making such adjustments.
Gender bias has been reported to affect treatment decisions in other fields and may also influence decisions about ICU admission.1,4,25 Sex-related differences may be due to differences in decision-making or preferences of the patients, their surrogate decision-makers or the health care team. For example, in a study of differences between men and women in the rate of hip and knee arthroplasty, women were found to have a greater need than men for joint replacement therapy, but despite equal willingness to undergo the procedure, they were less likely than men to discuss surgery with their physician, which led to less frequent recommendation for surgery.26 These differences increased with age. The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments — a large multicentre observational study and clinical trial that examined critical care delivery at the end of life — similarly found that physician–patient communication regarding preferences for aggressiveness of care was suboptimal and pronounced among older patients.27,28 In Canada, women are generally both younger and have a longer life-expectancy than their spouses, which leads to elderly women more frequently assuming a role as caregiver or supporter of their older male partner. In contrast, at end of life, women are older than men and more likely to be widowed. This different social context may lead to different decisions about aggressiveness of end-of-life care by men and women or their families. Although previous studies have not found sex to be independently associated with the decision to withdraw specific life-supporting therapies, such as mechanical ventilation, there may be substantial differences in the decision process concerning initiation versus withdrawal of specific forms of ICU therapies.29,30 Even though such invasive therapies do not necessarily improve clinical outcomes,31 our findings suggest that differential care strategies may exist among older men and women.
There may also be plausible biological explanations for the differences in mortality we found between critically ill older men and women. Sex has been found to influence the expression, progression and outcome of many common medical conditions and can influence pharmacokinetics and responses to therapy.32,33 It may also influence susceptibility to immunologic disorders and responses to severe infections and sepsis.23,34 These factors may explain differential outcomes of critical illness. However, a consistent relation between critical illness and sex, immunologic response and clinical outcomes has not been established.23,35,36 Different estrogen or other sex-related hormone levels and unique cytokine responses among younger and older men and women may explain in part the difference in mortality we observed.37 However, critical illness comprises a broad range of complex underlying conditions, and it is unlikely that a single or even a few simple sex-related biological differences apply equally and in all circumstances.
The strengths of our study include its large sample, the diverse nature of participating ICUs and patients, a detailed knowledge of severity of illness and comorbidities, and long-term outcome data. We were able to adjust for differences in acute physiology and chronic illnesses, as well as surgical versus medical admission diagnoses. We were also able to examine differences in the delivery of life-supporting care and determine the long-term outcomes for a large proportion of patients.
Our study had several limitations. Because it was observational, we were unable to establish causal relations. We also were unable to determine population prevalence rates for all ICU admission diagnoses and, thus, could not explore reasons for different admission rates among men and women for all conditions. Similarly, information was not available for all critically ill patients in all ICUs in Ontario. However, we used a broad spectrum of teaching and community hospitals and ICUs within a research network well known for its ability to capture valid and detailed information at the patient level. There may have been variables that we were unable to measure that had important effects on the reported associations. Finally, our results may not be generalizable to other jurisdictions, although patient demographics in our cohort are similar to those at other Canadian hospitals and our findings are consistent with reports of admission patterns and care received in other health care systems.4,5
In conclusion, we have shown that there may be important sex-and age-related differences in the provision of critical care and outcomes of critical illness within a health care system founded on the principle of equal access and opportunity for all patients. Further research is needed to determine whether these findings are due to sex-related differences in prevalence or response to critical illness, differences in preference for or access to intensive care, or other differences in the provision of care to critically ill patients.
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/177/12/1513/DC1
This article has been peer reviewed.
Contributors: All of the authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; drafted the article or revised it critically for important intellectual content; and gave final approval of the version to be published.
Acknowledgements: We are grateful for the contributions of the participating hospitals and members of the Canadian Critical Care Research Network as well as staff of the Institute of Clinical and Evaluative Sciences for their dedication to the betterment of population and patient care through research. We acknowledge the thoughtful review of the project methods and manuscript by Drs. Peter Dodek, Andreas Laupacis, Don Redelmeier and Eva Shimaoka. We dedicate this manuscript to the memory of Dr. William J. Sibbald: his passion was to understand critical illness, to improve critical care delivery and to mentor others to do the same.
Grant support was received from the Canadian Institutes of Health Research. Robert Fowler is a Career Scientist of the Ontario Ministry of Health and Long-term Care.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Core socioDemographic data variables in ICU Trials (CoDe-IT): a protocol for generating core data variables using a Delphi consensus process
- Sex and gender-based analysis and diversity metric reporting in acute care trials published in high-impact journals: a systematic review
- Evaluating Prognostic Bias of Critical Illness Severity Scores Based on Age, Gender, and Primary Language in the USA: A Retrospective Multicenter Study
- Prevalence and Intensive Care Bed Use in Subjects on Prolonged Mechanical Ventilation in Swedish ICUs
- Impact of physicians sex/gender on processes of care, and clinical outcomes in cardiac operative care: a systematic review
- Demographics, management and outcome of females and males with acute respiratory distress syndrome in the LUNG SAFE prospective cohort study
- The association of female sex with application of evidence-based practice recommendations for perioperative care in hip fracture surgery
- Because Womens Lives Matter, We Need to Eliminate Gender Bias
- How Patient Demographics, Imaging, and Beliefs Influence Tissue-Type Plasminogen Activator Use: A Survey of North American Neurologists
- Sex and Mortality of Hospitalized Adults After Admission to an Intensive Care Unit
- Incidence and predictors of critical events during urgent air-medical transport
- Approaches to diversity in family medicine: "I have always tried to be colour blind"
- The effect of patients' sex on physicians' recommendations for total knee arthroplasty
- Equal for whom? Addressing disparities in the Canadian medical system must become a national priority
- Sex matters: gender disparities in quality and outcomes of care
More in this TOC Section
Similar Articles

