


Abstract
Background: Persistent pain after breast cancer surgery affects up to 60% of patients. Early identification of those at higher risk could help inform optimal management. We conducted a systematic review and meta-analysis of observational studies to explore factors associated with persistent pain among women who have undergone surgery for breast cancer.
Methods: We searched the MEDLINE, Embase, CINAHL and PsycINFO databases from inception to Mar. 12, 2015, to identify cohort or case–control studies that explored the association between risk factors and persistent pain (lasting ≥ 2 mo) after breast cancer surgery. We pooled estimates of association using random-effects models, when possible, for all independent variables reported by more than 1 study. We reported relative measures of association as pooled odds ratios (ORs) and absolute measures of association as the absolute risk increase.
Results: Thirty studies, involving a total of 19 813 patients, reported the association of 77 independent variables with persistent pain. High-quality evidence showed increased odds of persistent pain with younger age (OR for every 10-yr decrement 1.36, 95% confidence interval [CI] 1.24–1.48), radiotherapy (OR 1.35, 95% CI 1.16–1.57), axillary lymph node dissection (OR 2.41, 95% CI 1.73–3.35) and greater acute postoperative pain (OR for every 1 cm on a 10-cm visual analogue scale 1.16, 95% CI 1.03–1.30). Moderate-quality evidence suggested an association with the presence of preoperative pain (OR 1.29, 95% CI 1.01–1.64). Given the 30% risk of pain in the absence of risk factors, the absolute risk increase corresponding to these ORs ranged from 3% (acute postoperative pain) to 21% (axillary lymph node dissection). High-quality evidence showed no association with body mass index, type of breast surgery, chemotherapy or endocrine therapy.
Interpretation: Development of persistent pain after breast cancer surgery was associated with younger age, radiotherapy, axillary lymph node dissection, greater acute postoperative pain and preoperative pain. Axillary lymph node dissection provides the only high-yield target for a modifiable risk factor to prevent the development of persistent pain after breast cancer surgery.
Despite a 10-year survival rate of 83%,1,2 between 25% and 60% of surviving patients who have undergone surgery for breast cancer experience persistent postsurgical pain,3–9 which is associated with reduced quality of life and functional impairment.10–13 Systematic reviews summarizing proposed risk factors for persistent pain after breast cancer surgery — including demographic, intraoperative and postoperative factors — have had several limitations, including outdated searches, inadequate attention to risk-of-bias assessment, lack of statistical pooling of measures of association and failure to evaluate the quality of evidence.5,10–14 We conducted a systematic review and meta-analysis of observational studies to identify risk factors for persistent pain after breast cancer surgery, addressing the limitations of previous reviews.
Methods
We completed our systematic review in accordance with the MOOSE statement15 and registered our protocol with PROSPERO (registration CRD42014013338).
Data sources and searches
Our searches, with no language restrictions, encompassed the MEDLINE, Embase, CINAHL and PsycINFO databases from inception to Mar. 12, 2015 (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1), as well as review of reference lists of eligible studies and 6 previous systematic reviews.5,10–14
We included cohort or case–control studies that explored risk factors for persistent pain after breast cancer surgery using an adjusted analysis. We used criteria of the International Association for the Study of Pain (IASP) to define persistent postsurgical pain as pain that develops after surgical intervention and lasts at least 2 months, with exclusion of other potential causes for the pain.16 Studies were ineligible if they included, in all available models, significant associations with variables collected after baseline; in such instances, the status of the predictor may be a result, rather than a cause, of the pain (see Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1). When more than 50% of study populations overlapped between articles, we included only the study with the largest sample size.
Study selection
Ten reviewers (L.W., S.A.K., B.R., H.Y.K., A.K., Y.C., S.C., C.P.B.deA., S.R.P., Z.I.) worked in pairs to screen, independently and in duplicate, the titles and abstracts of identified citations and, subsequently, the full texts of potentially eligible studies. The reviewers resolved disagreements by discussion or with the help of an adjudicator (L.W. or J.W.B.).
Data extraction and quality assessment
We used criteria from Users’ Guides to the Medical Literature17 to assess risk of bias, including representativeness of the study population, validity of outcome assessment, loss to follow-up and whether predictive models were optimally adjusted (Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1). Using standardized, pilot-tested data extraction forms and a detailed instruction manual, pairs of reviewers extracted data from 10 articles independently and in duplicate. Piloting was accomplished by having each reviewer team extract data from the same 2 articles. After 100% agreement was achieved for these 10 articles, data were extracted from each remaining article by a single reviewer and verified by a second reviewer. Disagreements were resolved by discussion. If a study reported multiple regression models, we used predefined criteria to select 1 model for data extraction (Appendix 4, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1).18
Data synthesis and analysis
We measured inter-rater agreement of full-text screening with the kappa statistic (κ).19 We reported the median and interquartile range (IQR) for intensity of persistent pain across eligible studies, converting all reported measures of pain intensity to a 10-cm visual analogue scale.20 When investigators reported the association of body mass index (BMI) or age as categorical data, we converted to continuous data (Appendix 5, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1).21,22
We pooled all factors assessed for an association with persistent pain that were reported by more than 1 study, and present odds ratios (ORs) and associated 95% confidence intervals (CIs). If a study provided the measure of association as a relative risk, we converted the relative risk to an OR.23 We used random-effects models for all meta-analyses.24
When pooling was not possible, we explored the consistency of association between pooled results and studies reporting the same predictors that could not be pooled. We used the following 3 criteria to identify predictors that were not amenable to pooling and showed promise for future research: a statistically significant association with persistent pain of p ≤ 0.01, a large magnitude of association (OR ≥ 2.0) and a sample size of 500 or more.
To avoid overestimating the strength of association by restricting statistical pooling to predictors that appeared in adjusted regression models, we imputed an OR of 1 for predictors that were tested in bivariable analyses but because of nonsignificance were excluded from adjusted analyses or were included in multivariable analyses with the only information provided being that they were “not significant.” We imputed an associated variance for all such predictors using the hot deck approach.25
To calculate the absolute risk increase for each predictor amenable to meta-analysis, we estimated the baseline risk for persistent postsurgical pain (30% in the low-risk group, who underwent sentinel lymph node biopsy) using data from the study with the largest sample size among studies at low risk of bias.26 We performed all statistical analyses using Stata statistical software version 13.1. All comparisons were 2-tailed, with a threshold p of 0.05.
Publication bias
For meta-analyses with at least 10 studies,22,27 we assessed publication bias by visual assessment of asymmetry of the funnel plot and performed the Begg rank correlation test28 and the Egger test.29
Subgroup analyses, meta-regression and sensitivity analyses
We evaluated heterogeneity for all pooled estimates through visual inspection of forest plots,27 because statistical tests of heterogeneity can be misleading when sample sizes are large and CIs are therefore narrow.30
We generated 4 a priori hypotheses to explain variability between studies, assuming larger association with persistent pain and (1) a high pain threshold (moderate to severe pain v. no to mild pain), (2) trials having greater risk of bias (on a component-by-component basis), (3) longer duration of follow-up and (4) larger proportion of patients lost to follow-up. We did not conduct subgroup analyses if there was only 1 study in a given subgroup. We performed sensitivity analyses examining the effect of imputing data for nonsignificant postulated predictors and of converting categorical data for BMI and age to continuous data.
Quality of evidence
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to summarize the quality of evidence for all meta-analyses.27,31 Given the high baseline risk we found for persistent pain after surgery for breast cancer (30%), we estimated that a 10% increase in the absolute risk would likely be sufficient for clinicians to address modifiable risk factors, which can be directly targeted in an effort to prevent persistent pain. We estimated that an absolute difference in risk of 20% between groups at low and high risk for persistent pain would be sufficient for clinicians to selectively target nonmodifiable risk factors to identify high-risk candidates for intervention. Therefore, we rated down for imprecision if the 95% CI associated with the risk difference included 10% for modifiable risk factors, or 20% for nonmodifiable risk factors.
Results
Of 6863 unique records, 492 English and 48 non-English language articles were potentially eligible; of these, 29 cohort studies26,32–59 and 1 case–control study60 proved eligible for our review (Figure 1). We excluded 5 studies with overlapping populations and 3 studies reporting significant factors that were collected after baseline (Appendix 2). There was near-perfect agreement (κ = 0.86) between reviewers at the full-text review stage. For the 3 studies in which eligibility was unclear, we obtained clarification from the authors.37,38,61 Among 8 studies for which some data needed for our analysis were not included in the published report, we obtained missing data from the authors of 2 studies.59,60

Flow diagram of study selection.
Definitions of persistent pain varied across the studies (Appendix 6, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1). Persistent postsurgical pain was reported at least 3 months after breast cancer surgery (range 3.28–72.50 mo) in all eligible studies. Seven studies reported that other causes of persistent pain had been excluded,32,37,38,42,44,46,52 but only 1 study explicitly used the IASP criteria for defining persistent postsurgical pain.44 The median sample size was 416 (IQR 250–772), and the median duration of follow-up was 24 months (IQR 12–42 mo) (Appendix 7, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1).26,32–60 In 11 (37%) of the 30 studies, regression models included only variables that were significant in bivariable analysis (and thus more vulnerable to chance),32,34,41,42,44,46,48,49,57–59 and 22 (73%) of the 30 studies failed to present data for nonsignificant predictors in their adjusted analysis.32,34,37,39–50,53,55–60
Twenty-three studies reported the prevalence of persistent pain after breast surgery, with a median prevalence of 37.5% (IQR 30%–51%).26,32–38,40–42,44–49,51,52,54,57–59 Twenty studies reported the intensity of persistent postsurgical pain;26,33–40,43–45,47,48,50,52,53,56–58 the median value was 3.22 cm (IQR 2.75–4.12 cm) on a 10-cm visual analogue scale (where values < 4 cm correspond to mild pain, values 4–7 cm correspond to moderate pain, and values > 7 cm correspond to severe pain62).
Risk of bias
Reported protection against bias among studies exploring predictors of persistent pain was limited, with 26 (87%) of the 30 studies not meeting at least 1 of our risk-of-bias criteria (Appendix 8, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1).32, 34–52, 54 – 57,59,60 All but 3 studies55,57,60 (90%) reported adequately adjusted regression models. We detected no evidence of publication bias (Table 1; funnel plots available by request to the authors).
GRADE evidence profile: predictors of persistent pain after breast cancer surgery
Predictors of persistent pain
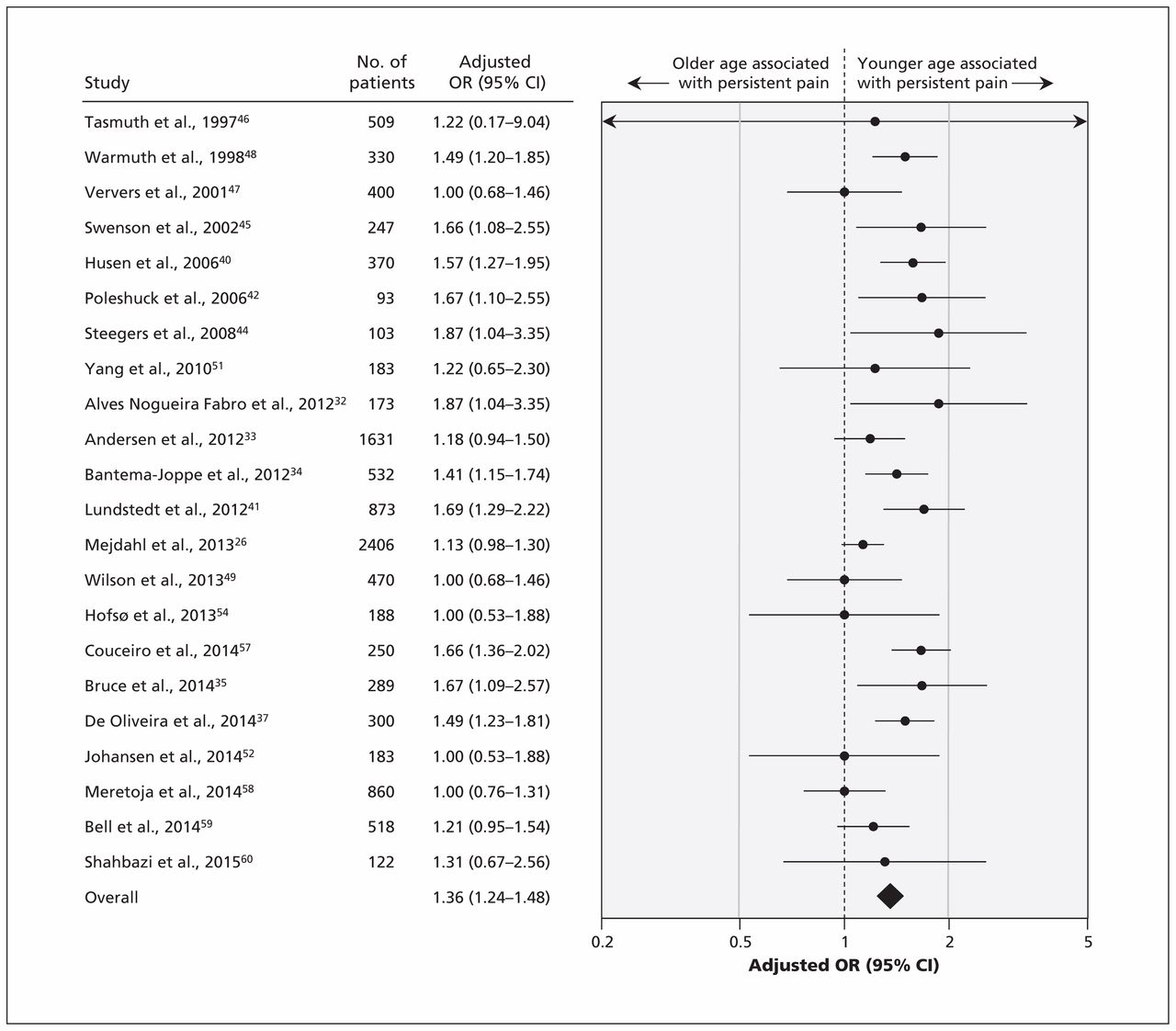
The 30 studies, involving a total of 19 813 patients, reported the association of 77 factors with the development of persistent pain. On the basis of our criteria, we conducted meta-analyses for 9 predictors of persistent pain. High-quality evidence showed a significant association between persistent pain after breast cancer surgery and 2 nonmodifiable factors (Table 1): younger age (OR for every 10-yr decrement 1.36, 95% CI 1.24–1.48 [Figure 2]; absolute risk increase 7% [95% CI 5%–9%] for every 10-yr decrement from age 70) and radiotherapy (OR 1.35, 95% CI 1.16–1.57 [forest plot available by request to the authors]; absolute risk increase 7%, 95% CI 3%–10%). We found a significant association between persistent pain and 3 modifiable factors (Table 1): axillary lymph node dissection (OR 2.41, 95% CI 1.73–3.35, high-quality evidence by GRADE [Figure 3]; absolute risk increase 21%, 95% CI 13%–29%), greater acute postoperative pain (OR for every 1-cm increment on a 10-cm visual analogue scale 1.16, 95% CI 1.03–1.30, high-quality evidence by GRADE [forest plot available by request]; absolute risk increase 3% [95% CI 1%–6%] for every 1-cm increment on a 10-cm visual analogue scale) and presence of preoperative pain (OR 1.29, 95% CI 1.01–1.64, moderate-quality evidence by GRADE [forest plot available by request]; absolute risk increase 6%, 95% CI 0%–11%).
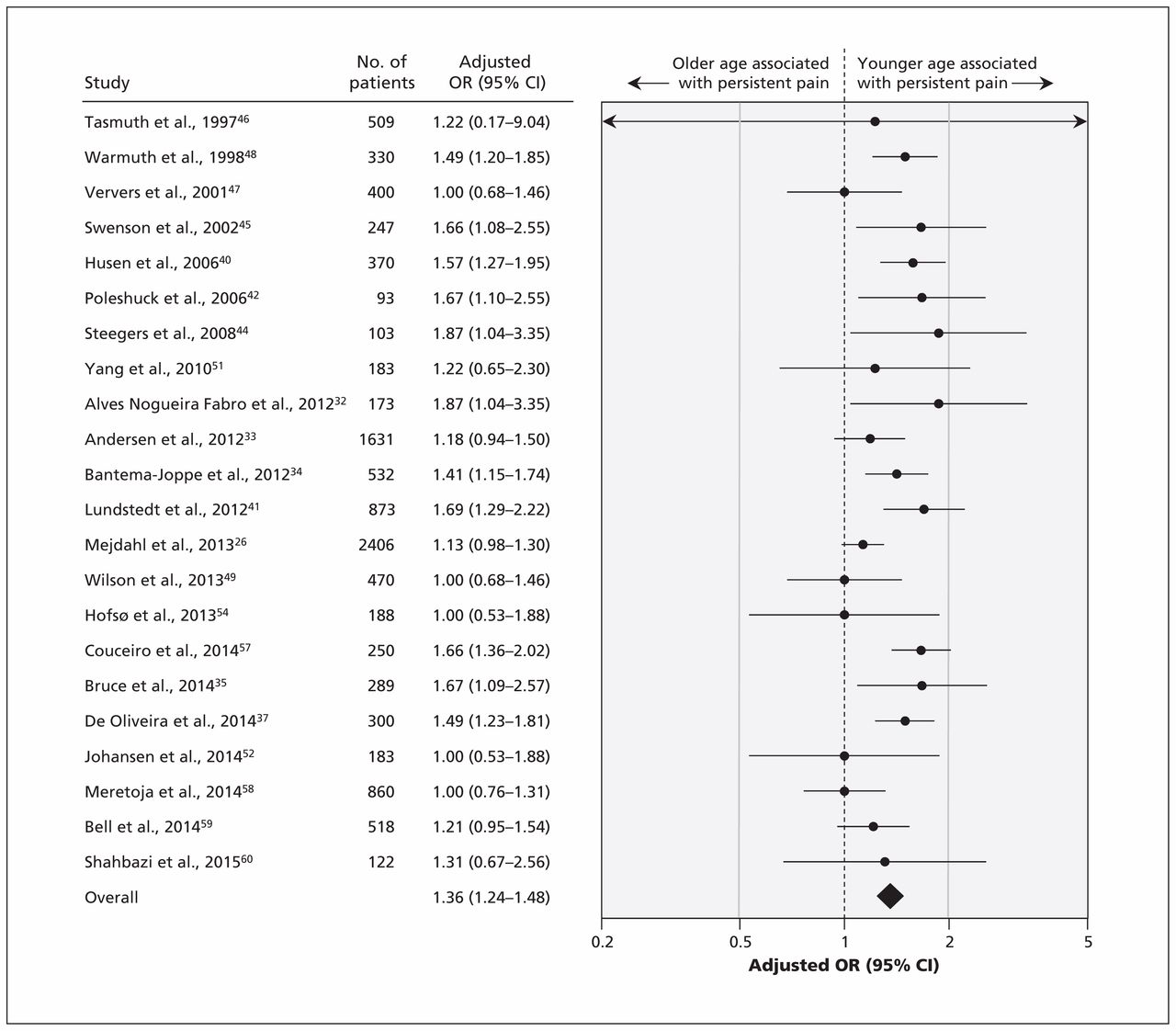
Meta-analysis of the association between persistent pain and age (per 10-year decrement). CI = confidence interval, OR = odds ratio.

Meta-analysis of the association between persistent pain and axillary lymph node dissection (ALND). CI = confidence interval, OR = odds ratio, SLNB = sentinel lymph node biopsy.
High-quality evidence showed no association between persistent pain and BMI (OR for every 5-point increment 1.11, 95% CI 0.99–1.24), type of breast surgery (breast-conserving surgery v. mastectomy or modified radical mastectomy, OR 1.08, 95% CI 0.90–1.30), chemotherapy (OR 1.12, 95% CI 0.98–1.29) or endocrine therapy (OR 1.07, 95% CI 0.94–1.22) (Table 1; forest plots available by request). The results from the 7 studies37,39,42,50,53,55,56 that reported 1 or more of the 9 predictors that we subjected to meta-analysis but whose data could not be pooled were consistent with our pooled analyses (Appendix 9, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1).
Appendices 10 and 11 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1) present the associations with persistent pain for the 68 factors that were not amenable to meta-analysis. Two of these factors (overall comorbidity and radiotherapy dosage) met our criteria as promising for future study.
Subgroup analyses, meta-regression and sensitivity analyses
We found no evidence to support a difference in associations with predictive factors when considering different thresholds for defining persistent pain, representativeness of the study population, whether a validated measure to capture pain was used, duration of follow-up or the proportion of patients lost to follow-up (Appendix 12, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1). The finding that predictive power did not differ across thresholds for defining persistent pain was strengthened by 2 cohort studies that used separate regression models for both high and low thresholds of persistent pain and reported similar associations across predictors.26,35 Whether or not we incorporated missing data for nonsignificant predictors or converted categorical data for age and BMI to continuous data (Appendix 13, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.151276/-/DC1) did not appreciably influence the results.
Interpretation
We found high-quality evidence that younger age, radiotherapy, axillary lymph node dissection and greater acute postoperative pain were associated with persistent pain after breast cancer surgery, and we found moderate-quality evidence for an association with preoperative pain. The strongest of these associations was with axillary lymph node dissection, with an absolute increase in risk of persistent pain of 21%. High-quality evidence showed that BMI, type of breast surgery, chemotherapy and endocrine therapy were not associated with persistent pain (Table 1). Investigators have tested 68 additional predictors that could not be statistically pooled (Appendices 10 and 11). Preliminary evidence suggested that 2 of these predictors may warrant additional study: overall comorbidity and radiotherapy dosage.
The most recent systematic review that explored risk factors for persistent pain after breast cancer surgery identified 8 studies that met our eligibility criteria.5 That review presented a qualitative synthesis concluding that axillary lymph node dissection and radiotherapy appeared to be risk factors for persistent pain.5 We have confirmed and quantified these associations through meta-analyses, and we have established 3 additional risk factors: younger age, the presence of preoperative pain and greater acute postoperative pain. We also identified high-quality evidence that BMI, type of breast cancer surgery, chemotherapy and endocrine therapy are not important predictors.
Typically, investigators present associations with predictors of persistent breast cancer pain as relative measures (e.g., OR, relative risk). However, it is the absolute risk increase that must guide clinical decision-making. Most efforts to reduce persistent postsurgical pain have focused on pharmacologic approaches to reduce preoperative or acute postoperative pain. Recent systematic reviews have found no compelling evidence to support the prevention of persistent postsurgical pain by perioperative administration of intravenous ketamine, oral gabapentin, oral pregabalin, nonsteroidal anti-inflammatory drugs, intravenous steroids, oral N-methyl-d-aspartate blockers, oral mexiletine, intravenous fentanyl, intravenous lidocaine, oral venlafaxine or inhaled nitrous oxide.63,64 Given that the absolute increase in chronic pain associated with preoperative or greater postoperative pain is modest (Table 1), any reduction in persistent pain achieved through pharmacologic reduction of perioperative pain will likely be obscured by the random error from all other determinants of long-term pain. In other words, it would require a very large (and thus implausible) reduction of perioperative pain to result in detectable effects in randomized trials examining the impact on chronic postoperative pain.
We found one association in which the absolute increase would be sufficient to suggest targeted interventions. Women who underwent axillary lymph node dissection experienced a 21% increase in the absolute risk of chronic postoperative pain. Although axillary staging is associated with persistent pain, the risks of omitting axillary nodal sampling include increasing the number of patients who are understaged and undertreated and who experience reduced survival.65 Thus, omission of axillary staging is not an appropriate approach to modifying pain risk. However, modification of surgical procedures related to axillary dissection constitutes a promising stand-alone target for risk reduction. Preliminary evidence suggests that sentinel lymph node biopsy, rather than standard axillary treatment,66 may reduce the risk of chronic pain after breast cancer surgery. Moreover, preservation of intercostobrachial nerves during axillary lymph node dissection reduces the incidence of postmastectomy pain syndrome after surgery67,68 and reduces the risk of sensory deficits after axillary clearance.69 Accordingly, the American Society of Clinical Oncology now recommends sentinel lymph node biopsy for patients with early-stage breast cancer, followed by dissection only if the biopsy result is positive,70 because this approach is associated with less pain and equivalent rates of axillary relapse compared with axillary dissection.71
Awareness of nonmodifiable risk factors could influence management by allowing identification of women at high risk of postoperative pain who might then be targeted for interventions — for example, psychotherapy or interventions such as paravertebral blocks in addition to general anesthesia, for which preliminary evidence suggests possible benefit.72 We postulated that increases of absolute risk of 20% or more would be required to warrant targeting a high-risk population: none of the individual nonmodifiable associations that we identified met this threshold (Table 1). However, a combination of risk factors might serve to identify a population warranting special attention.
Strengths and limitations
The strengths of our review include explicit eligibility criteria and a comprehensive search with no language restrictions, which identified 23 cohort studies that were not included in previous systematic reviews.5,10–14 We assessed the risk of bias in individual studies and used the GRADE approach to appraise the quality of evidence. We converted the intensity of persistent postsurgical pain to a 10-cm visual analogue scale across studies to optimize the interpretation of our findings. We have presented statistical pooling of associations between predictive factors and the risk of persistent pain. Our approach included imputing data for missing nonsignificant predictors (to avoid overestimating associations), and we conducted subgroup and sensitivity analyses that confirmed robust associations. Finally, we have presented not only relative but also absolute risk increases, which greatly strengthens inferences about the importance of the associations and possible implications for clinical care.
Our study had some limitations. We were unable to pool data for predictors from studies that used different continuous outcome measures to assess persistent pain in linear regression models.36,39,43,50,53,55,56 However, the results from these studies were consistent with the results from studies amenable to pooling. We used the IASP criteria for the definition of persistent pain in this review; however, 14 of the included studies did not report whether their assessment of persistent postsurgical pain excluded other causes of pain;26,33–36,43,45,47,48,50,51,54,56,58 as such, they may have overestimated the prevalence of persistent pain.
Conclusion
Development of persistent pain after breast cancer surgery was associated with younger age, radiotherapy, axillary lymph node dissection, greater acute postoperative pain and preoperative pain. Axillary lymph node dissection provided the only high-yield target for a modifiable risk factor, and no single nonmodifiable risk factor changed risk sufficiently to define a target population for an intervention to prevent persistent pain. Future research should establish the association between overall comorbidity, radiotherapy dosage and persistent postsurgical pain, and determine whether axillary nerve-sparing techniques are effective for reducing chronic pain after breast surgery.
Acknowledgements
For screening the full texts of non-English articles, the authors thank Toshiaki A. Furukawa, Department of Health Promotion and Human Behavior and Department of Clinical Epidemiology, Kyoto University Graduate School of Medicine and School of Public Health, Kyoto, Japan; Sun Makosso-Kallyth, Michael G. DeGroote Institute for Pain Research and Care, McMaster University, Hamilton, Ont.; Inge H.F. Reininga, Department of Trauma Surgery, and Sandra Brouwer, Department of Health Sciences, Community and Occupational Medicine, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands; Behnam Sadeghirad and Nigar Sekercioglu, Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ont.; Dmitry Shiktorov, Canadian Centre for Clinical Trials, Vaughan, Ont.; and Kari Tikkinen, Departments of Urology and of Public Health, Helsinki University Hospital and University of Helsinki, Helsinki, Finland. The authors thank Qi Zhou and Diane Heels-Ansdell, Department of Clinical Epidemiology and Biostatistics, McMaster University, for statistical advice. They also thank Robin Bell and Penelope Robinson, School of Public Health and Preventive Medicine, Monash University, Monash, Australia; Sayed Hossein Davoodi, Cancer Research Center, and Roghayeh Shahbazi, National Institute and Faculty of Nutrition and Food Technology, Shahid Beheshti University of Medical Sciences, Tehran, Iran; and Lena Engqvist Boman, Department of Learning, Informatics, Management and Ethics, Karolinska Institutet, Stockholm, Sweden, for providing supplementary information or answering queries regarding their studies. No financial compensation was provided to any of these individuals.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Data sharing: The relevant data in this study are available from the authors.
Contributors: Li Wang and Jason Busse conceived the study design; Li Wang, Sean Kennedy, Beatriz Romerosa, Henry Kwon, Alka Kaushal, Yaping Chang, Samantha Craigie, Carlos de Almeida, Rachel Couban, Shawn Parascandalo and Zain Izhar acquired the data; Li Wang performed the data analysis; Li Wang, Gordon Guyatt, Susan Reid, James Khan, Michael McGillion and Jason Busse interpreted the data and findings. Gordon Guyatt and Jason Busse provided methodological support and study supervision. Li Wang and Jason Busse drafted the manuscript, and all of the authors revised the manuscript for important intellectual content. In addition, all of the authors approved the final version for publication and agreed to act as guarantors of the work. Li Wang and Jason Busse have full access to all of the study data and had final responsibility for the decision to submit for publication.
Funding: No funds were received for the preparation of this manuscript. Li Wang is supported by a Michael G. DeGroote Postdoctoral Fellowship. The funding organization had no role in the design and conduct of the study; in the collection, analysis or interpretation of the data; or in the preparation, review or approval of the manuscript.
- Accepted March 24, 2016.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Predictors of fatal and nonfatal overdose after prescription of opioids for chronic pain: a systematic review and meta-analysis of observational studies
- Optimising psychological treatment for pain after breast cancer: a factorial design study protocol in Denmark
- Pre- and post-operative psychological interventions to prevent pain and fatigue after breast cancer surgery (PREVENT): a randomized controlled trial
- The serratus plane block for postoperative analgesia in breast and thoracic surgery: a systematic review and meta-analysis
- Risk factors for severe acute pain and persistent pain after surgery for breast cancer: a prospective observational study
- EduCan trial: study protocol for a randomised controlled trial on the effectiveness of pain neuroscience education after breast cancer surgery on pain, physical, emotional and work-related functioning
- Improving the therapeutic window of conventional opioids: novel differential signaling modulators
More in this TOC Section
Similar Articles
Collections

