


Abstract
BACKGROUND: Kingella kingae has been increasingly identified in patients with osteoarticular infections. Our main objective was to evaluate the association between carriage of K. kingae in the oropharynx of preschool children and osteoarticular infections.
METHODS: We conducted this prospective case–control study in 2 tertiary care pediatric hospitals (Canada and Switzerland) between 2014 and 2016. Potential cases were children aged 6 to 48 months with a presumptive diagnosis of osteoarticular infection according to the treating emergency physician. Confirmed cases were those with diagnosis of osteomyelitis or septic arthritis proven by positive findings on technetium-labelled bone scan or magnetic resonance imaging or identification of a microorganism in joint aspirate or blood. For each case, we recruited 4 age-matched controls from among children presenting to the same emergency department for trauma. The independent variable was presence of oropharyngeal K. kingae DNA identified by a specific polymerase chain reaction assay. We determined the association between oropharyngeal carriage of K. kingae and definitive osteoarticular infection.
RESULTS: The parents of 77 children admitted for suspected osteoarticular infection and 286 controls were invited to participate and provided informed consent. We identified K. kingae in the oropharynx of 46 (71%) of 65 confirmed cases and 17 (6%) of 286 controls; these results yielded an odds ratio of 38.3 (95% confidence interval 18.5–79.1).
INTERPRETATION: Detection of oropharyngeal K. kingae was strongly associated with osteoarticular infection among children presenting with symptoms suggestive of such infection.
Acute osteoarticular infection is an important problem in the pediatric population, potentially threatening both life and limb.1,2 Historically, such infections have largely been attributed to Staphylococcus aureus, Streptococcus pyogenes and Haemophilus influenzae type b,3,4 but most series have reported a high proportion (23% to 70%) of culture-negative infections.4–6 Recent European studies reported substantial proportions of cases with K. kingae infection, ranging from 15% to 75%.7–9 Although these high proportions may be related to increasing prevalence of the pathogen, they are more likely related to improvements in detection techniques, including a K. kingae–specific polymerase chain reaction (PCR) assay.10,11
Diagnosing K. kingae infections of the bones and joints is difficult for 2 reasons. First, the clinical presentation is often subtle, and the results of paraclinical investigations may remain within normal ranges.7,12 Second, K. kingae is a fastidious microorganism that is difficult to grow on solid media,13 which may explain the high proportion of negative culture results for joint aspirates from children with symptoms highly suggestive of infection.
The pathogenesis of osteoarticular infection related to K. kingae remains unclear, but there is evidence that the bacterium initially colonizes the oropharynx before penetrating the bloodstream and invading distant organs.14 Recent studies from Europe and Israel have suggested a strong association between oropharyngeal carriage of K. kingae and the risk of osteoarticular infection in young children.14–16 However, this relation has never been shown in North America.
In this multicentre study, we sought to evaluate the association between osteoarticular infection and detection of oropharyngeal K. kingae by PCR in young children.
Methods
Study design
This prospective, multicentre case–control study involved a convenience sample of children visiting 2 tertiary care pediatric hospitals. We recruited participants at the emergency departments of Geneva University Hospitals (Geneva, Switzerland) and the Centre hospitalier universitaire Sainte-Justine (Montréal) between August 2014 and June 2016. Both sites are university-affiliated hospitals, and the annual emergency department census is about 30 000 and 80 000, respectively. We chose these sites because 1 member of the study team (S.M.) has worked at both locations, both sites have good clinical research infrastructure, and there was previous collaboration on another study.17
Study population
We recruited 2 populations of participants, aged 6 to 48 months: cases and controls. Potential cases were children with clinical suspicion of osteoarticular infection, according to the treating physician. These children presented to the emergency department for joint pain, limp or decreased limb movement without trauma, with or without fever. After identifying a potential case, the treating physician contacted a research assistant, who invited the family to participate in the study.
To identify definitive cases, 2 of the investigators (J.G., C.R.) reviewed the medical charts of all recruited potential cases at the end of the study. They were blinded to the oropharyngeal swab results and to each other’s reviews assessing the probability of osteoarticular infection. The assessors classified each of these cases as impossible, possible, highly probable or confirmed. Children with a classification of “impossible” had another confirmed diagnosis (e.g., leukemia or fracture). Those with a classification of “possible” had abnormal findings on analysis of joint aspirate, but no growth of microorganisms. Those with a classification of “highly probable” had positive findings on technetium-labelled bone scanning or magnetic resonance imaging, but no growth of microorganisms. Children with a classification of “confirmed” had suspicious imaging findings and identification of a microorganism in the joint aspirate or blood. For purposes of the analysis, children with classification of “highly probable” or “confirmed” were considered to represent definitive cases.
The control group consisted of a convenience sample of children visiting the same emergency departments for benign trauma, matched for age (within 3 mo). The charts for all of these children were reviewed to ensure that osteoarticular infection did not develop during the week following recruitment.
Exposure
The primary independent variable of interest was the presence of K. kingae, as detected by PCR from an oropharyngeal swab sample, as described below.
All participants underwent clinical and paraclinical evaluations at the discretion of the treating physician. In all cases, these evaluations included blood sampling (for complete blood count, erythrocyte sedimentation rate, C-reactive protein and culture) and various imaging investigations, depending on the clinical presentation and the treating physician.
After a parent provided written informed consent, an oropharyngeal sample was obtained using a dry swab (ESwab Liquid Amies nylon flocked applicator, Copan Diagnostics) for PCR identification of K. kingae. For patients with suspected septic arthritis, a joint aspirate was obtained for analysis and culture, including Gram staining and PCR assay specific to K. kingae. Aerobic blood culture and synovial fluid culture (using blood bottles and plates) were performed according to standard protocols to identify the most common aerobic bacteria. For a few patients with suspected bone infection, a bone aspirate was obtained for analysis and culture, including Gram staining and PCR testing for K. kingae.
All oropharyngeal samples from the Montréal site were kept frozen at –20°C until batch shipment of 25 samples to the central laboratory in Geneva, Switzerland. Samples from Geneva were analyzed in the 24–48 hours after recruitment. The oropharyngeal samples were analyzed with a real-time PCR assay designed to detect 2 gene targets from the K. kingae RTX toxin locus, rtxA and rtxB.18 To evaluate the analytical sensitivity of these assays, we used a range of serially diluted K. kingae genomic DNA. The assay exhibited a sensitivity of 30 colony-forming units, which is 10 times more sensitive than a previously published semi-nested, broad-range assay for the 16S rRNA gene, as described previously.18 DNA was extracted with a MagNAPure LC instrument using the MagNAPure LC DNA isolation kit II (Roche Molecular Biochemicals) according to the manufacturer’s instructions. TaqMan Universal PCR Master Mix reagent with AmpErase UNG (uracil N-glycosylase; Applied Biosystems) was used, with 5 μL of input DNA and nuclease-free water (Promega). Each PCR analysis was performed in duplicate, with blinding as to the type of participant (case or control). A PCR-positive sample collected from a culture-proven K. kingae sample was used as a positive control.
For each participant, a standardized chart review form was completed by a research assistant, with baseline demographic characteristics, information about the disease and results of paraclinical investigations. For all participants, the treating physicians and research personnel were blinded to the results of oropharyngeal swab testing.
Statistical analysis
Baseline demographic characteristics and types of infection were described for both the hospitals and the types of participants. The primary analysis included definitive cases and controls, to measure the association between oropharyngeal carriage of K. kingae and osteoarticular infection. We constructed a 2 × 2 table showing the numbers of positive oropharyngeal samples for cases and controls and then calculated odds ratios (ORs). We calculated 95% confidence intervals (CIs) for all measurements.
Previous studies suggested that the prevalence of K. kingae was as high as 75% among young children with osteoarticular infection15 and was 5% to 10% among controls.13,19,20 We estimated that recruitment of 32 cases would yield 90% power to identify a difference of 25% in the prevalence of K. kingae between the 2 groups, with an α value of 0.05. Therefore, we recruited 4 controls for each case.
Ethics approval
The study was approved by the research ethics boards of the Centre hospitalier universitaire Sainte-Justine and the Geneva University Hospitals. For inclusion in the study, each child’s legal guardian had to provide written informed consent. Assent from the children was deemed unnecessary because of their young age.
Results
From August 2014 to June 2016, the parents of 77 children admitted for suspected osteoarticular infection and of 286 controls were invited to participate and provided written informed consent to be included in the study (Figure 1). Of the 77 potential cases, 69 had a definitive diagnosis of osteoarticular infection, according to the 2 chart reviewers (100% agreement between reviewers). Four cases were excluded because no oropharyngeal sample was obtained. As a result, 65 definitive cases and 286 controls were included in the final analysis.
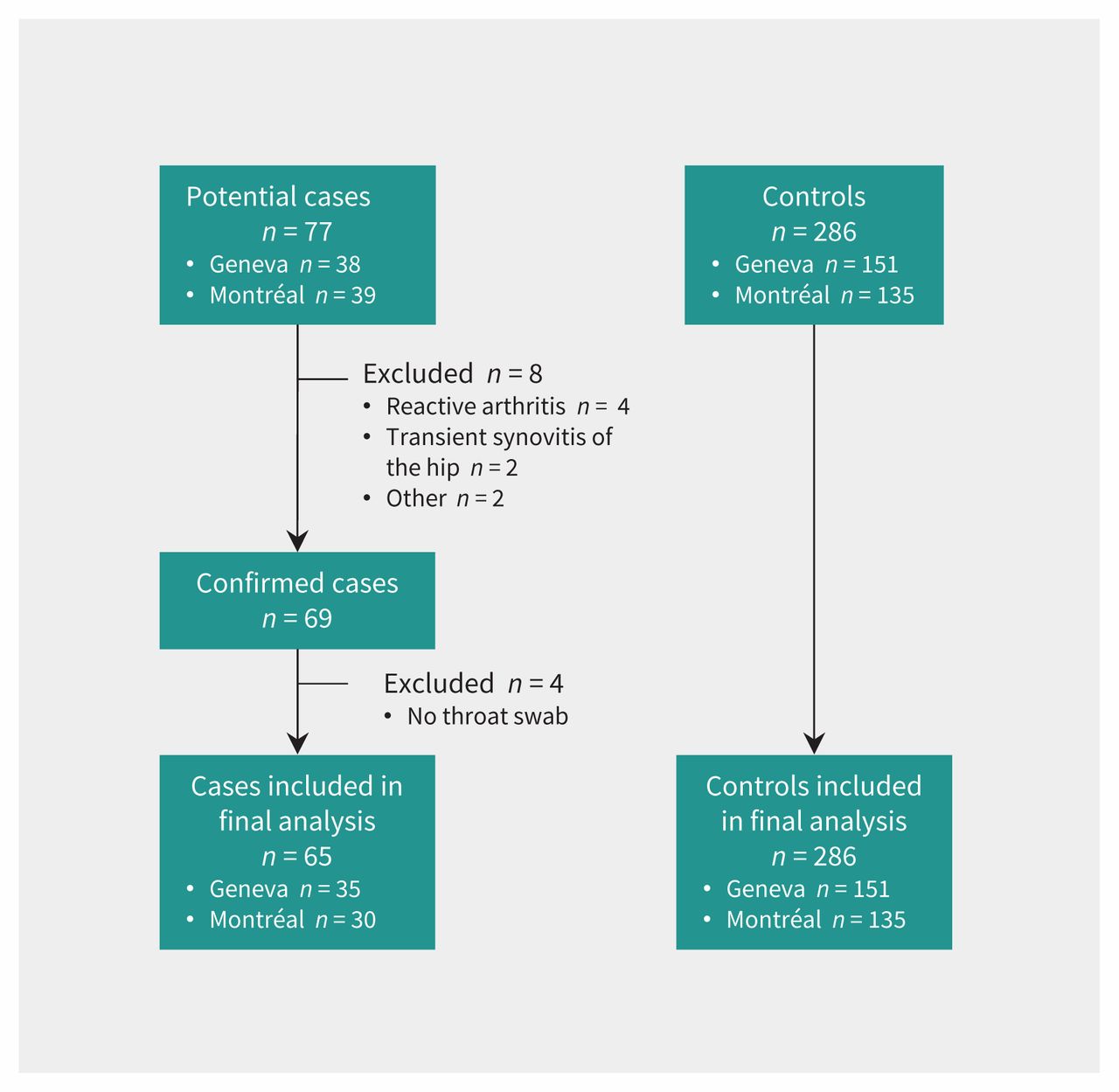
Flow chart for cases and controls included in a study of the association between oropharyngeal carriage of Kingella kingae and osteoarticular infection.
Table 1 describes the baseline demographic characteristics of the study participants. The 2 sites recruited similar numbers of participants. Median age and sex were similar for the cases from the 2 hospitals and the control group. Blood culture results were available for 62 (95%) of the participants with confirmed osteoarticular infection.
Baseline characteristics of the participants
In 34 cases, K. kingae infection was identified in the joint or bone aspirate (4 by culture and 30 by PCR), and in 8 cases, another microorganism was identified in the blood (n = 2), in a joint (n = 5) or both (n = 1). After K. kingae, the most common bacterial species was S. aureus (4 cases); 2 cases had S. pyogenes, 1 case had Salmonella typhi, and 1 case had Escherichia coli. The proportion of cases with K. kingae infection was similar at the 2 sites: 17 (49%) of 35 cases in Geneva and 17 (57%) of 30 cases in Montréal. The proportion of cases with another bacterium was also similar for both sites (5 [14%] in Geneva and 3 [10%] in Montréal). In the remaining 23 cases, no bacteria were identified in blood, bone or joint, including the 13 cases for which no culture of joint or bone aspirate was performed; of these 23 cases, oropharyngeal K. kingae was identified in 14.
The PCR assays detected K. kingae in the oropharyngeal samples of 46 of the 65 cases (71%, 95% CI 59%–80%) (Table 2). This proportion increased to 31 of the 34 cases with proven osteoarticular infection caused by K. kingae (91%, 95% CI 77%–97%). Among the 8 patients with growth of another bacterial species, oropharyngeal K. kingae was identified in only 1 patient. Kingella kingae was identified in 17 of the 286 controls (6%, 95% CI 4%–9%). The OR for the association between oropharyngeal carriage of K. kingae and the risk of osteoarticular infection was 38.3 (95% CI 18.5–79.1).
Presence of oropharyngeal Kingella kingae
The presence of oropharyngeal K. kingae was strongly associated with proven osteoarticular infection by K. kingae (OR 158, 95% CI 44–568). A subanalysis identified a higher prevalence of oropharyngeal carriage of K. kingae among the controls at the Geneva site (14/151 [9%]) than among controls at the Montréal site (3/135 [2%]), a difference of 7 percentage points (95% CI 1.5–13 percentage points). However, this difference had no effect on the association between oropharyngeal carriage of K. kingae and risk of osteoarticular infection at each site: for Geneva, OR 33 (95% CI 12–86), and for Montréal, OR 76 (95% CI 19–297). Finally, 31 of the 34 cases with K. kingae infection involved children younger than 23 months.
Interpretation
Using a highly sensitive PCR-based assay designed to detect 2 gene targets from K. kingae DNA, the current study showed that oropharyngeal carriage of this bacterial species was strongly associated with osteoarticular infection among young children presenting with symptoms suggestive of this diagnosis.
The association between oropharyngeal carriage of K. kingae and osteoarticular infection was first reported in a case series documenting 3 children with invasive K. kingae infection in Israel, published in 2009.14 A subsequent prospective study, published in 2013, found that K. kingae was the causative agent for osteoarticular infection in 75% of 40 Swiss children aged 6 to 48 months.15 More important, the oropharyngeal swabs from all 30 of the K. kingae cases yielded positive results. Finally, a French study published in 2012 similarly reported positive throat culture results for K. kingae for 8 of 12 children with confirmed K. kingae joint infection.16
Although determining the frequency of pathogens was not an objective of this study, the most common pathogen responsible for osteoarticular infection among young children in our study was K. kingae. It was present in 17 of the 30 cases in Montréal, while another pathogen was identified in only 3 other cases. Overall, K. kingae represented 85% of the Montréal cases in which bacteria were identified. Previous studies conducted in North America21–23 have suggested a lower prevalence of K. kingae, leading to the belief that K. kingae is a European problem that is not present in North America.
Recent review articles have generally suggested S. aureus as the most common pathogen for osteoarticular infection.1,24 Studies conducted in California,21 Tennessee22 and Texas23 have reported S. aureus as the most common pathogen of osteoarticular infection in children, with proportions ranging from 40% to 85%. However, in contrast to those earlier studies, we used a highly sensitive technique to identify K. kingae in the joint aspirate samples. In addition, we primarily identified K. kingae in children younger than 23 months. It is possible that the younger age of our study population accounts for the difference in reported pathogens, relative to earlier studies.
The strong association between oropharyngeal carriage of K. kingae and osteoarticular infection has several clinical implications. First, given the important OR value, detection of K. kingae in the oropharynx might be useful to confirm a potential diagnosis of osteoarticular infection. Second, oropharyngeal swabbing could be useful to suggest the pathogen in many young children with suspected bone infections, from whom bone aspirate is more complicated to obtain and for whom blood culture frequently yields negative results.23 In this clinical situation, detection of oropharyngeal K. kingae could help to establish the presumptive causative microorganism. This approach was suggested in a recent study reporting K. kingae infection in 10 children with culture-negative spondylodiskitis.25 However, this possibility must be considered with caution because our study reported oropharyngeal K. kingae in 1 of 8 children with osteoarticular infection and presence of another bacterial species. Identification of oropharyngeal K. kingae may help to guide antibiotic treatment, given that resistance to β-lactams and high-level resistance to clindamycin have been reported for K. kingae. In the current study, 14 of the 23 cases in which no pathogen was identified by culture had oropharyngeal K. kingae identified by PCR. It could be inferred that this was the pathogen causing the osteoarticular infection. PCR-based assays could also reduce the time for bacterial identification from days to hours, relative to current culture standards.26
Limitations
This study had limitations, many inherent to the case–control design. We attempted to mitigate selection bias by conducting case determination and identifying oropharyngeal K. kingae in a blinded fashion. Also, all potential cases were reviewed by 2 co-investigators, who were blinded to the oropharyngeal results in determining the diagnosis. Despite involvement of 2 centres, the sample size was small. Although the magnitude of the association between oropharyngeal carriage of K. kingae and osteoarticular infection was large, the prevalence of oropharyngeal carriage should be validated in multiple North American cities. Finally, the delay and conditions of transport from Canada to Switzerland for the oropharyngeal swabs may have reduced the ability of swab testing to identify K. kingae. However, the observed association was similar at the 2 sites.
Conclusion
This study showed a strong association between oropharyngeal K. kingae detected by PCR and osteoarticular infection among preschool children presenting with symptoms suggestive of this diagnosis. In light of these results, investigation for oropharyngeal K. kingae by a PCR assay should be considered for children with clinical suspicion of osteoarticular infection. Identification of the pathogen in the oropharynx should orient the presumptive diagnosis toward this pathogen. The prevalence and natural evolution of oropharyngeal carriage of K. kingae among healthy children should be evaluated by means of multicentre studies.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Jocelyn Gravel, Dimitri Ceroni and Sergio Manzano conceived the study and completed the initial study protocol. Jocelyn Gravel, Dimitri Ceroni, Laurence Lacroix, Christian Renaud, Guy Grimard and Sergio Manzano obtained funding for the study. All of the authors contributed to the design and provided suggestions to improve the study. Jocelyn Gravel and Sergio Manzano were responsible for data collection in their respective settings. Jocelyn Gravel analyzed the data. Jocelyn Gravel drafted the manuscript, and all of the authors contributed to the revisions. All of the authors approved the final version for publication and agreed to act as guarantors of the work.
Funding: This study was financially supported by the Réseau mèreenfant de la Francophonie (Mother and Child French Network).
- Accepted March 29, 2017.
References
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

