


- © 2004 Canadian Medical Association or its licensors
A 47-year-old man was admitted with a 2-month history of left pleuritic chest pain, shortness of breath on exertion, occasional night sweats and a 7-kg weight loss. Examination and a chest radiograph revealed a large pleural effusion on the left side. Vital signs were normal except for an arterial oxygen saturation of 94%. Laboratory workup was significant only for an erythrocyte sedimentation rate of 97 mm/h. Pleural fluid aspiration yielded an exudate consistent with both tuberculosis and malignant disease (pH 7.12, glucose level 8 mg/dL, leukocyte count 2.06 х 103/μL with 90% mononuclear cells, lactate dehydrogenase level 1824 IU/L) and negative results on microbiological and cytological staining. A Mantoux test gave a positive result (11 mm of induration). Sputum was negative for acid-fast bacilli. A CT scan revealed a large pleural effusion on the left, with abnormal and uneven thickening of adjacent pleura and no axillary or mediastinal lymph node enlargement. Pleural biopsy revealed tumour cells consistent with malignant mesothelioma, epithelioid type. The patient recalled working as a constructor of asbestos roofs over 20 years ago, an established risk factor in mesothelioma.
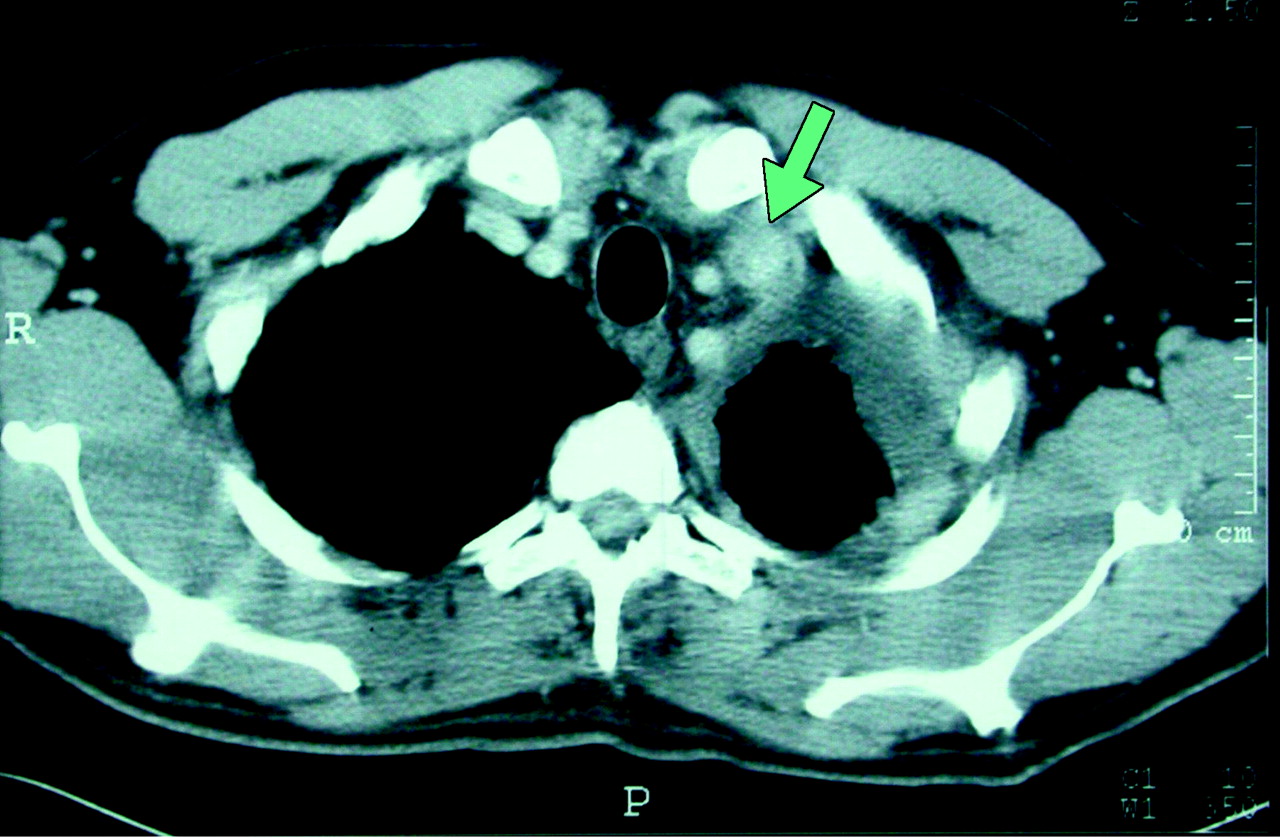
Two days later the patient developed left supraclavicular fullness, which was tender to palpation and associated with erythema of the overlying skin (Fig. 1). A duplex ultrasound of the area showed extensive thrombosis of the left jugular and subclavian veins. On review, the original CT scan did reveal the venous thrombosis (then subclinical) (Fig. 2, arrow). The patient was treated with heparin and referred for surgical consultation. He underwent left pneumonectomy, hemipericardiectomy and hemidiaphragmectomy; however, he had extensive lymphatic metastases and unfortunately died 3 months after first presenting.


Supraclavicular or neck swelling is a common but frequently unrecognized sign of internal jugular vein thrombosis.1 Subclavian vein thrombosis is often associated.2 Thus, the appearance of supraclavicular swelling is an important clinical sign. Most common causes of internal jugular vein thrombosis are central venous catheters or intravenous drug abuse, but oropharyngeal infections (Lemierre syndrome)3 and hypercoagulable states are also important causes.4 Hypercoagulability associated with malignant disease is well recognized and causes predominantly venous thrombosis and occasionally arterial thromboembolism.5 Virchow's triad identifies epithelial injury, blood flow abnormalities and hypercoagulable state as predisposing factors to intravascular thrombosis.5,6 Thus, although venous thrombosis in patients with mesothelioma is rare, this incident may be explained by the proximity of the tumour to the veins involved. The treatment of choice for internal jugular venous thromboembolism is the use of low-molecular-weight heparin followed by long-term oral warfarin therapy.
Ami Schattner Natasha Kozack Kaplan Medical Centre Rehovot and Hebrew University Hadassah Medical School Jerusalem, Israel
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

