


Abstract
THIS IS THE FIRST OF 2 ARTICLES EVALUATING cardiac events in patients undergoing noncardiac surgery. In this article, we review the magnitude of the problem, the pathophysiology of these events, approaches to risk assessment and communication of risk. The number of patients undergoing noncardiac surgery worldwide is growing, and annually 500 000 to 900 000 of these patients experience perioperative cardiac death, nonfatal myocardial infarction (MI) or nonfatal cardiac arrest. Although the evidence is limited, a substantial proportion of fatal perioperative MIs may not share the same pathophysiology as nonoperative MIs. A clearer understanding of the pathophysiology is needed to direct future research evaluating prophylactic, acute and long-term interventions. Researchers have developed tools to facilitate the estimation of perioperative cardiac risk. Studies suggest that the Lee index is the most accurate generic perioperative cardiac risk index. The limitations of the studies evaluating the ability of noninvasive cardiac tests to predict perioperative cardiac risk reveals considerable uncertainty as to the role of these popular tests. Similarly, there is uncertainty as to the predictive accuracy of the American College of Cardiology / American Heart Association algorithm for cardiac risk assessment. Patients are likely to benefit from improved estimation and communication of cardiac risk because the majority of noncardiac surgeries are elective and accurate risk estimation is important to allow informed patient and physician decision-making.
Throughout the last few decades noncardiac surgery has made substantial advances in treating diseases (e.g., cancer) and improving patient quality of life (e.g., arthroplasty). As a result, the number of patients undergoing noncardiac surgery is growing worldwide.1 However, such surgery is associated with significant cardiac morbidity, mortality and consequent cost.
This is the first of 2 articles evaluating major perioperative cardiac events in patients undergoing noncardiac surgery. In this article, we review the magnitude of the problem, the pathophysiology of these events, approaches to perioperative risk assessment and the communication of risk. In the second article, we will present evidence regarding monitoring strategies for perioperative myocardial infarction (MI), propose diagnostic criteria for perioperative MI and review the evidence for perioperative prophylactic cardiac interventions.
The breadth of the topics covered in this article prohibited a fully systematic approach to this review. Although this is a narrative review, we did conduct thorough literature searches in each area and contacted the authors of relevant articles when necessary. We sought relevant systematic reviews and have highlighted their findings in our discussion. Our methods and attempt to focus on systematic reviews distinguish our review from several others,2,3,4 which may explain why we often reached different conclusions.
Magnitude of risk of major perioperative cardiac events
Patients undergoing noncardiac surgery are at risk of major perioperative cardiac events (cardiac death, nonfatal MI and nonfatal cardiac arrest). Patients experiencing an MI after noncardiac surgery have a hospital mortality rate of 15%–25%,5,6,7,8 and nonfatal perioperative MI is an independent risk factor for cardiovascular death and nonfatal MI during the 6 months following surgery (hazard ratio 18; 95% confidence interval [CI] 6–57).9 Patients who have a cardiac arrest after noncardiac surgery have a hospital mortality rate of 65%,10 and nonfatal perioperative cardiac arrest is a risk factor for cardiac death during the 5 years following surgery.11
Table 1 presents the proportion of patients undergoing noncardiac surgery who experienced a major cardiac event in prospective cohort studies with samples of more than 300 patients that did not have restrictions as to the type of surgery (e.g., vascular surgery) and that required patients to have at least 1 measurement of a cardiac enzyme or biomarker after surgery.5,6,7,8,12,13,14 We included only studies that required such measurement after surgery because perioperative MI occurs primarily during the first 3 days after surgery,7,15 a period when the majority of patients are receiving narcotic therapy and therefore may not experience cardiac symptoms during their MI.6,7,16
Table 1.
The pooled results from the studies evaluating patients who had or were at risk of cardiac disease5,6,7,8,12,13 suggest that 3.9% (95% CI 3.3%–4.6%) of these patients experience major perioperative cardiac events. The study by Lee and colleagues14 is the only study in Table 1 that included relatively unselected patients (i.e., it was not limited to patients referred to a medical consult service or to patients with or at risk of coronary artery disease). Their findings suggest that major perioperative cardiac events occur in 1.4% (95% CI 1.0%– 1.8%) of adults 50 years of age or older undergoing elective noncardiac surgery requiring hospital admission.
There are a number of reasons why the time frames of the studies reported in Table 1 — most were conducted over a decade ago — limit their ability to inform us about the current incidence of major perioperative cardiac events. First, patients with coronary artery disease are now living longer as a result of major medical advances.17 Therefore, patients with high burdens of coronary artery disease are now surviving long enough for other conditions to develop that require surgical consideration, including cancer and severe osteoarthritis of the hip and knee. Second, there has been a shift in practice patterns toward advanced medical care (including surgery) for elderly patients. Third, some surgical interventions have become less invasive.
Despite these limitations, results from the study by Lee and colleagues likely represent a conservative estimate of the current incidence of major perioperative cardiac events among unselected adults undergoing noncardiac surgery that requires hospital admission. We say conservative because of the authors' exclusion of emergent surgical cases and the increasing numbers of elderly people undergoing noncardiac surgery today. Emergent cases represent about 10% of noncardiac surgeries,18 and patients undergoing emergent surgery are at higher risk of major perioperative cardiac events than patients undergoing elective surgery (odds ratio 2.6, 95% CI 1.2–5.6).8
About 100 million adults worldwide undergo noncardiac surgery annually.1 Conservative assumptions suggest that half of these patients are in an at-risk age group1 and that the results from the study by Lee and colleagues14 reflect their cardiac risk. Therefore, each year it is likely that 500 000 to 900 000 patients worldwide experience perioperative cardiac death, nonfatal MI or nonfatal cardiac arrest. This problem is important because of the burden of illness it represents and the health resources it consumes: perioperative cardiac complications prolong hospital stays by a mean of 11 days (95% CI 9–12 days).15
Pathophysiology of perioperative cardiac events
Cardiac death
In studies that examined perioperative cardiac death, authors attributed the cause to MI in 66% of the cases and to arrhythmia or heart failure in 34% (Table 1). However, none of these studies used formal criteria to establish the underlying causes of cardiac death or determined intrarater reliability.5,6,7,8,13 In addition, it is unclear whether ischemia, arrhythmia or a pre-existing cardiomyopathy caused heart failure that resulted in death. Further well-designed studies are needed to determine accurately the frequency with which these events cause perioperative cardiac death and to elucidate other causes.
Cardiac arrest
We identified only 1 study that examined the cause of cardiac arrest in patients undergoing noncardiac surgery.10 Sprung and colleagues evaluated 223 cases of perioperative cardiac arrest that occurred between the start of anesthesia and discharge from the recovery room in patients undergoing noncardiac surgery at a single centre from 1990 to 2000. A committee of staff anesthesiologists, anesthesia chief residents, certified nurse anesthetists and recovery room nurses reviewed all cases and judged the probable cause of each cardiac arrest. The dominant causes were cardiac causes (e.g., MI) and bleeding (Table 2). Confidence in these conclusions will require a multicentre study of all cardiac arrests that occur in the postoperative period (i.e., from the start of surgery to 30 days after surgery).
Table 2.
Myocardial infarction
Arterial thrombosis is the underlying cause of the majority of nonoperative MIs.19 In 64%–100% of patients with nonoperative MIs, coronary artery plaque fissuring occurs,20,21 and in 65%–95% there is an acute luminal thrombus.21,22,23,24,25 The pathophysiology underlying MIs in the operative setting is less clear.
Interpretation of coronary pathology and angiography data
Two studies of the coronary pathology underlying fatal perioperative MI revealed that two-thirds of the patients had significant left main or 3-vessel coronary artery disease.26,27 These studies also showed that most of the patients did not exhibit plaque fissuring and only about one-third had an intracoronary thrombus. These findings suggest that a substantial proportion of these fatal perioperative MIs may have resulted from an increase in oxygen demand in the setting of fixed coronary artery stenoses.28 In contrast, a study involving patients who underwent coronary angiography before vascular surgery revealed that the majority of nonfatal perioperative MIs occurred in arteries without high-grade stenoses. These findings suggest that the events may have resulted from plaque fissuring and acute coronary artery thrombosis.29 Given the conflicting evidence, further study is needed to establish the pathophysiology of fatal and nonfatal perioperative MIs; this area of investigation would gain important insights from a study in which all patients experiencing perioperative MI underwent acute coronary angiography.
Triggers of perioperative myocardial infarction
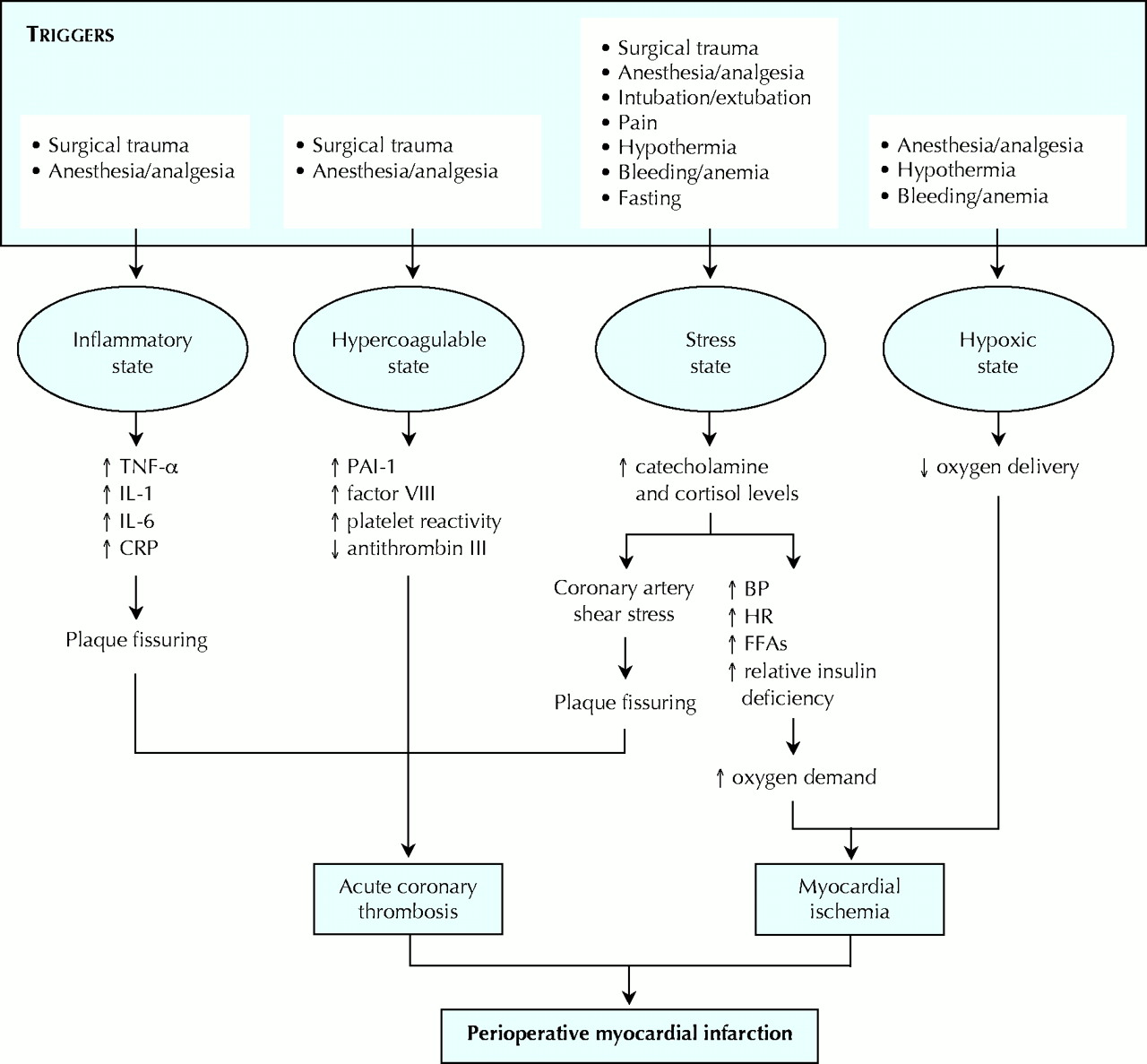
Surgery, with its associated trauma, anesthesia and analgesia, intubation and extubation, pain, hypothermia, bleeding and anemia, and fasting, is analogous to an extreme stress test. Fig. 1 illustrates how these factors initiate inflammatory, hypercoagulable, stress and hypoxic states, which are associated with perioperative elevations in troponin levels, arterial thrombosis and mortality.30,31,32,33,34,35
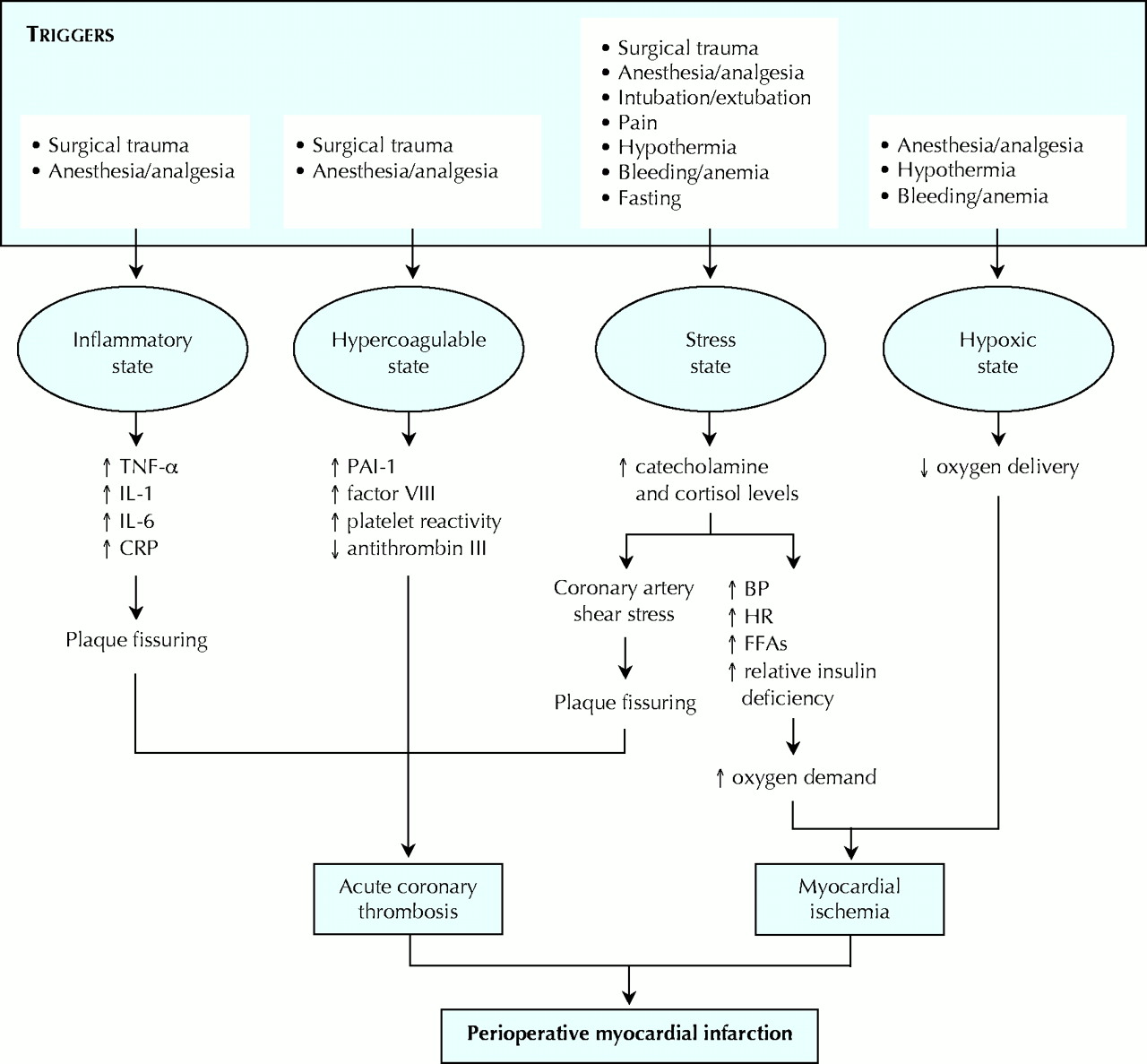
Fig. 1: Potential triggers of states associated with perioperative elevations in troponin levels, arterial thrombosis and fatal myocardial infarction. TNF-α = tumour necrosis factor-α, IL = interleukin, CRP = C-reactive protein, PAI-1 = plasminogen activator inhibitor-1, BP = blood pressure, HR = heart rate, FFAs = free fatty acids.
Increasing grades of surgical trauma and general anesthesia can initiate inflammatory and hypercoagulable states.31,36,37,38,39 The inflammatory state involves increases in tumour necrosis factor-α, interleukin (IL)-1, IL-6 and C-reactive protein; these factors may have a direct role in initiating plaque fissuring and acute coronary thrombosis.38,40,41,42 The hypercoagulable state involves increases in plasminogen activator inhibitor-1, factor VIII and platelet reactivity, as well as decreases in antithrombin III; all of these factors can lead to acute coronary thrombosis.31,43,44
The stress state involves increased levels of catecholamines (epinephrine and norepinephrine) and cortisol. Perioperative catecholamine and cortisol levels increase with general anesthesia, anesthetic reversal, extubation, increasing pain scores, increasing grades of surgical trauma, anemia, fasting and hypothermia.45,46,47,48,49,50 Increased stress hormone levels result in increases in blood pressure, heart rate, coronary artery sheer stress, relative insulin deficiency and free fatty acid levels.33,50,51 Coronary artery shear stress may trigger plaque fissuring and acute coronary thrombosis.50 The other factors increase oxygen demand and can result in perioperative myocardial ischemia, which is strongly associated with perioperative MI.13,52,53
Factors that can initiate a hypoxic state include anemia, hypothermia (through shivering), and anesthesia and analgesia (through suppression of breathing).54,55,56 Perioperative hypoxia can result in myocardial ischemia in the setting of a hemodynamically significant coronary artery stenosis.
Further research is needed to determine which of these potential triggers are independent risk factors for perioperative MI and to assess other potential triggers. To determine whether suppression of these triggers will prevent perioperative MIs will require large randomized trials.
Preoperative cardiac risk assessment
Although no research has documented its benefits, preoperative cardiac risk assessment may serve an important function. The majority of noncardiac surgeries are elective, and an accurate estimate of risk would facilitate informed patient and physician decision-making. For example, if an elderly woman with multiple risk factors undergoing hip arthroplasty for osteoarthritis were accurately informed that her risk of a major perioperative cardiac event was 10%– 12%, she might decide to delay surgery and live with her suboptimal quality of life until her granddaughter graduates in 1 year. Further, accurate risk estimates provide guidance for perioperative management, including the choice of surgical techniques and the location and intensity of postoperative care.
Clinical indices
Two types of clinical indices — generic and Bayesian — exist to estimate the risk of a major perioperative cardiac event in patients undergoing noncardiac surgery. The various published generic indices (Lee, Goldman, Larsen and Gilbert indices) estimate a patient's risk through determination of how many predictors of risk (e.g., history of angina, diabetes, emergent surgery) the patient has.14,57,58,59 The published Bayesian risk indices (Kumar and Detsky indices) modify the hospital's average cardiac event rate for a specific surgery (pretest probability) through use of a patient's individual index score (likelihood ratio), which is based on how many predictors of risk (e.g., history of angina, diabetes) the patient has; this results in an estimate of the patient's risk of a perioperative cardiac event (post-test probability).8,12
Although several studies have compared the predictive accuracy of the generic and Bayesian risk indices,8,12,14,59,60 only 2 have used contemporary pretest probabilities based on data from the hospitals studied at that time.8,12 These 2 studies revealed superior prediction capabilities of the Bayesian risk indices.8,12 Although these studies fulfill the methodologic criteria of a clinical prediction rule study,61 only the Detsky index has shown consistent results in a separate setting, although this validation is limited to 1 high-quality single-centre study.8 However, the current predictive accuracy of the Detsky index is uncertain, because no high-quality studies have established contemporary complication rates for individual surgeries, and it is unknown whether contemporary complication rates at one institution are generalizable to others. Because of the limitations of the available data (e.g., most of the studies occurred at single university hospitals, and most did not focus on composite outcomes with more or less equally important components), determining the optimal risk index to predict major perioperative cardiac events will require a multicentre study that includes several university and nonuniversity hospitals.
Until more definitive research becomes available, clinicians require a practical clinical index to facilitate perioperative cardiac risk estimation. The Lee index is the best validated and most accurate predictive generic risk index, and it is simple to use in clinical practice.14 It consists of 6 equally weighted cardiovascular risk factors: high-risk surgery (intraperitoneal, intrathoracic or suprainguinal vascular surgery), history of ischemic heart disease, history of congestive heart failure, history of cerebrovascular disease (stroke or transient ischemic attack), use of insulin therapy for diabetes and a preoperative serum creatinine level of more than 175 μmol/L (> 2.0 mg/dL). Table 3 shows the estimated risk of a major perioperative cardiac event based on the number of risk factors met. Although there are many positive aspects of the Lee index, the study that derived and validated it had limitations (it excluded emergent surgeries and surgical cases with an expected length of stay of less than 2 days during the years 1989–1994).
Table 3.
Noninvasive testing
Table 4 presents the results from a recent meta-analysis that evaluated the prognostic accuracy of 6 noninvasive tests for predicting perioperative cardiac death or nonfatal MI in patients undergoing vascular surgery.62 The results suggested a trend toward superior prognostic accuracy with dobutamine stress echocardiography compared with the other tests, but this trend was statistically significant only in comparison with myocardial perfusion scintigraphy. These results warrant cautious interpretation for the following reasons: the majority of studies included in the meta-analysis used weak methods (e.g., retrospective design, failure to blind individuals interpreting the test results to the clinical predictors of risk, and failure to blind the outcome assessors to the test results); the cumulative event rate for most of the tests was low; there was significant heterogeneity across the study results for individual tests; and test results were analyzed using a single threshold (i.e., results were dichotomized as positive or negative).
Table 4.
The relevance of this last limitation is highlighted in another recent meta-analysis that evaluated semiquantitative dipyridamole myocardial stress perfusion imaging for predicting perioperative cardiac death or nonfatal MI in patients undergoing vascular surgery.63 This meta-analysis included 9 studies evaluating 1179 patients, of whom 82 experienced cardiac death or nonfatal MI. Rather than considering test results as positive or negative, variation in the likelihood ratios were shown based on the extent of reversibility of myocardial defects (Table 5). In the setting of a diagnostic study, many would not consider variations in likelihood ratios of 0.42 to 2.9 of much relevance. In evaluating prognostic information, however, a patient or physician may value the ability to distinguish between a perioperative risk of a major cardiovascular outcome of 3%, 7% or 18%, so to them the test and its results are relevant (Table 5). Narrowing the confidence intervals for these results, and determining more precisely the number of patients who are likely to have the various proportions of reversible myocardial defects, will require further high-quality research.
Table 5.
The limitations of the studies evaluating the ability of noninvasive cardiac tests to predict perioperative risk leaves considerable uncertainty concerning the role of these popular tests before noncardiac surgery. Until investigators undertake further research, some physicians may want to consider noninvasive cardiac testing in patients who have severe exercise restrictions (e.g., patients with severe claudication) that limit the clinical assessment of symptoms suggestive of coronary artery disease.
When considering which noninvasive cardiac test to order, physicians may want to consider the following: the results of the relevant meta-analyses, and their limitations; the uncertain utility of noninvasive tests in patients undergoing nonvascular, noncardiac surgery; what tests and expertise are available at their hospital; what test a patient can undertake (e.g., patients with severe claudication are probably unable to complete an exercise electrocardiographic stress test); and the likelihood of an important change in risk estimation (e.g., physicians using the Lee index should use a noninvasive test to refine the risk estimate only if the refined risk estimate, based on the potential test results, would be interpreted by the patient or physician as important). To illustrate the last point, if the results of the meta-analysis evaluating semiquantitative dipyridamole myocardial stress perfusion imaging in patients undergoing vascular surgery (Table 5) are applicable to other types of surgery, use of this noninvasive test in patients undergoing nonvascular, noncardiac surgery with no risk factors on the Lee index (i.e., a risk estimate of 0.4% [Table 3]) may result in a refined risk estimate of less than 0.01% or 5%; for patients with 3 risk factors on the Lee index (i.e., a risk estimate of 5.4% [Table 3]), the refined risk estimate may be 2% or 14%.
American College of Cardiology / American Heart Association algorithm for preoperative cardiac risk assessment
Some authors have recommended that physicians use the American College of Cardiology / American Heart Association (ACC/AHA) algorithm to stratify patients undergoing noncardiac surgery according to their perioperative cardiac risk.64,65 It should be noted that this algorithm was not derived from a prospective study; rather, it was derived from the interpretation of data from various studies and the judgments of the committee members.66 The few studies that have evaluated the reliability of the ACC/AHA algorithm have limitations: they had few cardiac events; they failed to demonstrate that the algorithm is effective in stratifying cardiac risk across the 3 strata proposed in the algorithm; and they did not compare the predictive accuracy of the ACC/AHA algorithm with the most accurate clinical risk indices (i.e., the Lee and Detsky indices).67,68 The recommendations in the ACC/ AHA algorithm regarding noninvasive testing ignore the issue of patient and physician values. As mentioned earlier, noninvasive testing is relevant only if patients or physicians would value the potential magnitude of changes in predicted risk.
How do clinicians define and communicate perioperative cardiac risk?
A recent survey of 104 general internists performing a high volume of preoperative consultations (mean of 17 per month) provides insights into how physicians communicate and define perioperative cardiac risk.69 Of the respondents, 96% indicated that they informed patients of their perioperative cardiac risk, but 77% of these respondents indicated that they communicated the risk subjectively (i.e., simply telling patients that they were at low, moderate or high risk). When asked what they meant by low, moderate and high risk, respondents provided 8, 27 and 12 different definitions, respectively. The range of values provided by the respondents for the definitions demonstrated marked variation: from less than 1% to less than 20% for low risk, 1% to 50% for moderate risk, and more than 2% to more than 50% for high risk.
Given the variety of definitions used for low, moderate and high risk, physicians should avoid these terms to prevent misunderstandings. Instead, physicians can tell patients and surgeons the percentage risk of cardiac death, nonfatal MI or nonfatal cardiac arrest or the expected event rate among 100 or 1000 similar patients. Given the uncertainty around the risk estimation data, physicians may also want to present the range of risk consistent with the 95% CI. For example, a 50-year-old man receiving insulin therapy who is scheduled to undergo a bowel resection would have 2 risk factors according to the Lee index (Table 3); a consultant could convey to the patient and surgeon that the patient's risk of cardiac death, nonfatal MI or nonfatal cardiac arrest is 1.5% to 3.5%.
Conclusion
Noncardiac surgery is associated with substantial cardiac mortality, morbidity and consequent cost. Perioperative MIs likely result from triggers that initiate inflammatory, hypercoagulable, hypoxic and stress states. Because the majority of noncardiac surgeries are elective, accurate estimation of risk of perioperative cardiac events is important to allow informed patient and physician decision-making. The Lee index is a practical clinical risk index that physicians can use to facilitate risk estimation. There is significant uncertainty regarding the predictive accuracy of preoperative noninvasive cardiac tests and the ACC/AHA algorithm for cardiac risk assessment. Physicians informing a patient or surgeon about the patient's risk of a major perioperative cardiac event should provide specific risk estimates and avoid assumptions associated with subjective classifications of risk.
Footnotes
This article has been peer reviewed.
Contributors: P.J. Devereaux was responsible for the conception of the manuscript and analysis of the data and wrote the first draft. He and Lee Goldman were responsible for data acquisition. All of the authors contributed to the manuscript's design and interpretation of the data, provided critical revisions to the manuscript and approved the final version.
Acknowledgements: P.J. Devereaux is supported by a Senior Research Fellowship Award from the Canadian Institutes of Health Research. Deborah Cook is a Chair of the Canadian Institutes for Health Research.
Competing interests: None declared.
References
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- PerIoperative iNflammatory reSponse assessment In hiGH-risk patienTs undergoing non-cardiac surgery (INSIGHT): study protocol of a prospective non-interventional observational study
- Postoperative mortality in hip fracture patients stratified by the Revised Cardiac Risk Index: a Swedish nationwide retrospective cohort study
- Pathway for Enhanced Recovery after Spinal Surgery-A Systematic Review of Evidence for use of Individual Components
- Effects of beta-blocker therapy on mortality after elective colon cancer surgery: a Swedish nationwide cohort study
- Should we stop aspirin before noncardiac surgery?
- Derivation and Validation of a Geriatric-Sensitive Perioperative Cardiac Risk Index
- Cardiovascular and Ventilatory Consequences of Laparoscopic Surgery
- External validation of the Revised Cardiac Risk Index and update of its renal variable to predict 30-day risk of major cardiac complications after non-cardiac surgery: rationale and plan for analyses of the VISION study
- Cardiac Risk of Noncardiac Surgery
- Improving Operating Room Efficiency, Part 1: General Managerial and Preoperative Strategies
- Kidney Function Alters the Relationship between Postoperative Troponin T Level and Death
- Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study
- Assessment of Perioperative Cardiac Risk of Patients Undergoing Noncardiac Surgery Using Coronary Computed Tomographic Angiography
- Perioperative Beta Blockade in Noncardiac Surgery: A Systematic Review for the 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines
- Perioperative Beta Blockade in Noncardiac Surgery: A Systematic Review for the 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines
- Need for Elective PCI Prior to Noncardiac Surgery: High Risk Through the Eyes of the Beholder
- Surgery Casualties: Do Not Leave Hearts Behind Enemy Lines
- Pre-Operative Risk Assessment With Cardiac Computed Tomography: All Dressed Up And Nowhere to Go
- Risk of Elective Major Noncardiac Surgery After Coronary Stent Insertion: A Population-Based Study
- The coronary CT angiography vision protocol: a prospective observational imaging cohort study in patients undergoing non-cardiac surgery
- Coronary Calcium Score as an Adjunct to Nuclear Myocardial Perfusion Imaging for Risk Stratification Before Noncardiac Surgery
- Effects of {beta}-blockers in patients undergoing noncardiac surgery
- Non-invasive cardiac stress testing before elective major non-cardiac surgery: population based cohort study
- Preoperative NT-proBNP and CRP predict perioperative major cardiovascular events in non-cardiac surgery
- Is a Pre-Operative Brain Natriuretic Peptide or N-Terminal Pro-B-Type Natriuretic Peptide Measurement an Independent Predictor of Adverse Cardiovascular Outcomes Within 30 Days of Noncardiac Surgery?: A Systematic Review and Meta-Analysis of Observational Studies
- Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data
- Preoperative Risk Stratification Using Gated Myocardial Perfusion Studies in Patients with Cancer
- Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery
- Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies
- Assessing and Reducing the Cardiac Risk of Noncardiac Surgery
- Surveillance and prevention of major perioperative ischemic cardiac events in patients undergoing noncardiac surgery: a review
More in this TOC Section
Similar Articles

