


A 76-year-old woman presented with difficulty swallowing solid food and with shortness of breath. Her symptoms had developed over several months. She did not have odynophagia, had not experienced weight loss and did not drink alcohol or smoke. Her physical exam was unremarkable.
Barium esophagography showed a posterior oblique indentation of the proximal esophagus slightly above the level of the aortic arch, suggestive of an aberrant right subclavian artery compressing the esophagus (Figure 1A). The diagnosis was confirmed by a contrast-enhanced computed tomography scan, which showed an aneurysmatic right subclavian artery originating as the last branch of the aortic arch. The artery followed a retroesophageal course to cross the midline, resulting in a prominent compression and shift of the patient’s esophagus. This aberrant anatomy was clearly visible in computed tomography images reconstructed 3-dimensionally using a volume-rendering technique (Figure 1B).
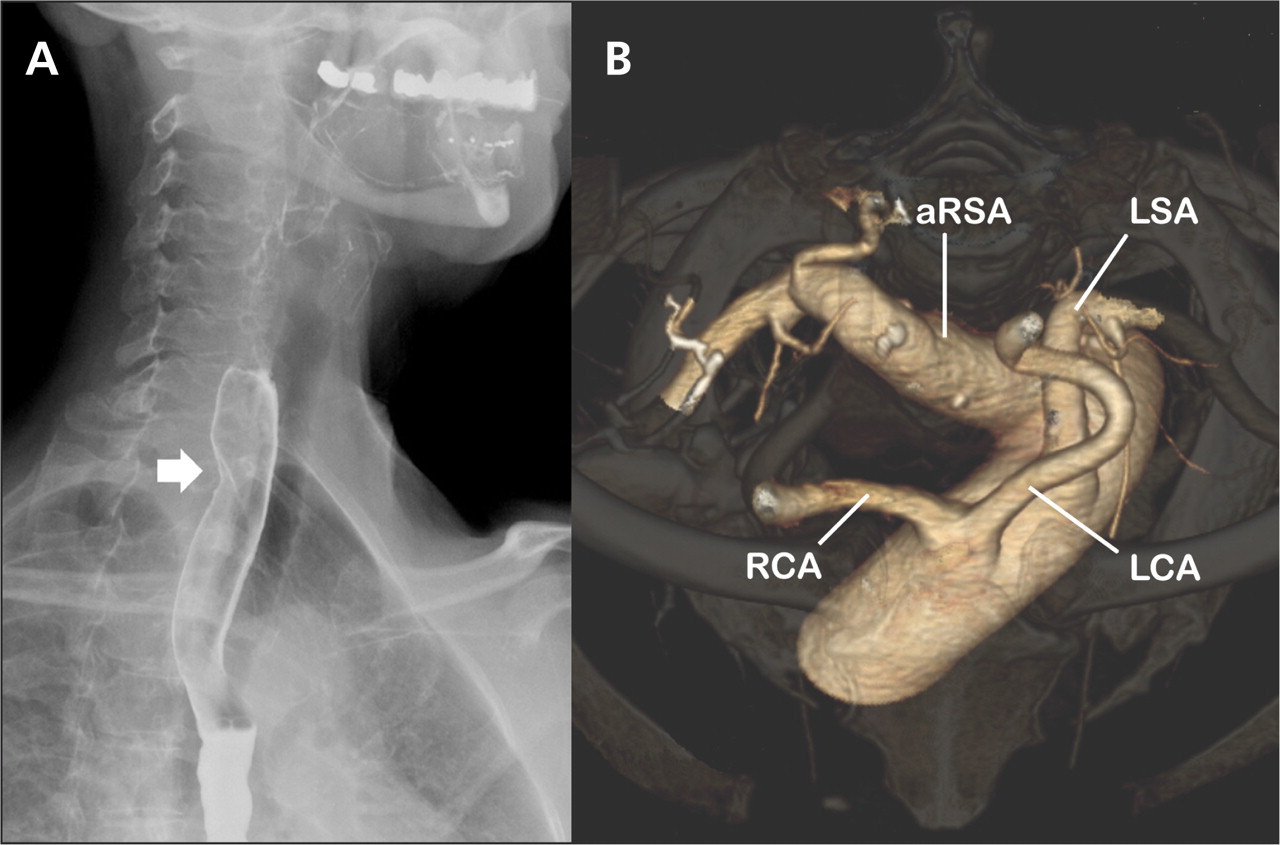
Figure 1: (A) A barium esophagogram (lateral projection) of a 76-year-old woman, showing an oblique indentation of the posterior esophageal wall (arrow) that suggests extrinsic compression of the esophagus by an aberrant right subclavian artery. (B) Volume-rendered, 3-dimensional computed tomography scan (cranial view) of the aortic arch. The right subclavian artery arises as the last branch from the aortic arch distal to the origin of the left subclavian artery. Notice the aneurysmal origin of the aberrant right subclavian artery. RCA = right common carotid artery, LCA = left common carotid artery, LSA = left subclavian artery, aRSA = aberrant right subclavian artery.
An aberrant right subclavian artery is a relatively common congenital anomaly. It has a prevalence of up to 1.8%. About a third of people with this anatomic variant experience symptoms. Dysphagia is experienced in 90% of such cases, whereas dyspnea, as in our patient, is less common. 1 Dysphagia secondary to extrinsic esophageal compression by an aberrant right subclavian artery is known as dysphagia lusoria. This term dates back to the first description of the condition in 1794 by David Bayford, who called it “lusus naturae,” meaning “freak or jest of nature.” 2
‘The late-onset presentation in our patient is not uncommon. Contributing factors for the development of symptomatic dysphagia in elderly persons include decreased flexibility of the esophagus itself associated with aging, and increased esophageal compression caused by progressive aneurysmal dilatation of the aberrant artery or arteriosclerosis-induced rigidity of the vessel wall. 3 Our patient’s dyspnea was likely related to external tracheal compression by the aberrant artery or compression of the pulmonary artery. The latter is common in patients with an aneurysmal dilatation of the aberrant right subclavian artery associated with a Kommerell diverticulum. We performed a right caroticosubclavian bypass. Our patient reported complete resolution of her pulmonary symptoms and dramatic improvement of her dysphagia after the surgery.
Footnotes
-
Previously published at www.cmaj.ca
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

