


Abstract
Background: Diverse health care leadership teams may improve health care experiences and outcomes for patients. We sought to explore the race and gender of hospital and health ministry executives in Canada and compare their diversity with that of the populations they serve.
Methods: This cross-sectional study included leaders of Canada’s largest hospitals and all provincial and territorial health ministries. We included individuals listed on institutional websites as part of the leadership team if a name and photo were available. Six reviewers coded and analyzed the perceived race and gender of leaders, in duplicate. We compared the proportion of racialized health care leaders with the race demographics of the general population from the 2016 Canadian Census.
Results: We included 3056 leaders from 135 institutions, with reviewer concordance on gender for 3022 leaders and on race for 2946 leaders. Reviewers perceived 37 (47.4%) of 78 health ministry leaders as women, and fewer than 5 (< 7%) of 80 as racialized. In Alberta, Saskatchewan, Prince Edward Island and Nova Scotia, provinces with a centralized hospital executive team, reviewers coded 36 (50.0%) of 72 leaders as women and 5 (7.1%) of 70 as racialized. In British Columbia, New Brunswick and Newfoundland and Labrador, provinces with hospital leadership by region, reviewers perceived 120 (56.1%) of 214 leaders as women and 24 (11.5%) of 209 as racialized. In Manitoba, Ontario and Quebec, where leadership teams exist at each hospital, reviewers perceived 1326 (49.9%) of 2658 leaders as women and 243 (9.2%) of 2633 as racialized. We calculated the representation gap between racialized executives and the racialized population as 14.5% for British Columbia, 27.5% for Manitoba, 20.7% for Ontario, 12.4% for Quebec, 7.6% for New Brunswick, 7.3% for Prince Edward Island and 11.6% for Newfoundland and Labrador.
Interpretation: In a study of more than 3000 health care leaders in Canada, gender parity was present, but racialized executives were substantially under-represented. This work should prompt health care institutions to increase racial diversity in leadership.
Race and gender-based disparities in health care leadership1–4 may negatively affect the health of marginalized patients.5,6 Diverse leadership is an integral step in establishing equitable health care institutions that serve the needs of all community members.7 Many barriers prevent racialized people, women and gender nonbinary individuals from attaining leadership positions, including reduced access to networking opportunities, 8–10 discrimination from patients and colleagues2,11–13 and an institutional culture that views white, male leaders as most effective. 14,15 The intersectional effects of discrimination may intensify these barriers for racialized women and nonbinary people.16,17 Fundamentally, diversity and inclusion in our institutions is important on the basis of basic human rights for all people.18
Health care leadership in Europe and the United States is thought to lack gender and racial diversity.19–22 The degree to which these imbalances exist across Canadian health care institutions is not clear. Despite past evidence that men hold a disproportionate number of health care leadership positions in Canada,23,24 a recent study noted gender parity among leaders of provincial and territorial ministries of health.25 Among university faculty26,27 and administration, 28 racialized individuals appear to be under-represented, suggesting that a similar trend may exist in health care leadership.
Race and gender can be studied in many ways.29 Perceived race is a measure of “the race that others believe you to be,” and these assessments “influence how people are treated and form the basis of racial discrimination including nondeliberate actions that nonetheless lead to socioeconomic inequities.”29 Similarly, perceived gender refers to an observer’s assumptions about a person’s gender, which can lead to differential and unfair treatment. 30 Assessing perceived race and gender provides crucial insights into the ways in which social inequalities are informed and produced.29 In this study, we sought to identify the perceived race and gender of hospital executive leaders in Canada and of nonelected leaders of the provincial and territorial health ministries. Furthermore, we wanted to analyze how the perceived racial composition of health care leadership compares with the racial composition of the population in the geographic areas that these leaders serve.
Methods
Study design
We conducted a cross-sectional study comparing the diversity of health care leadership with that of the general population in Canada. We collected hospital and health ministry data from Apr. 7, 2021, to July 10, 2021. We report this study in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.31
Data sources
We used the most recent Canadian Institute for Healthcare Information (CIHI)’s list of hospital beds staffed and in operation (2018 to 2019) to determine the 200 largest hospitals in Canada.32 For each hospital on this list, we collected executive leadership information via publicly accessible institutional websites. Of note, no hospitals on this list were located in the 3 territories. The health leadership structures differed among provinces, and as a result, some hospitals on the CIHI list did not have their own executive teams. Health leadership in Alberta, Saskatchewan, Nova Scotia and Prince Edward Island is organized such that a single, province-wide leadership team oversees all hospitals. British Columbia, New Brunswick and Newfoundland and Labrador are divided into several health regions, with a different executive team assigned to the hospitals in each region. In Manitoba, Ontario and Quebec, executive teams serve each individual hospital site or, less commonly, hospital networks in a given region. For provincial or territorial ministries of health, we collected executive team information from the organizational structure chart or the leadership team list on each province and territory’s Ministry of Health website.
Inclusion and exclusion criteria
For hospital leadership teams, we included individuals listed on the senior executive team on each website. To maximize reproducibility, we included all individuals listed as executive leadership or a synonymous heading. Given their influential role in selecting leaders and involvement in administrative decision-making, we also included members of the board of directors on each hospital website. We excluded hospital foundation members and administrative assistants unless they were explicitly listed as members of the leadership team. For provincial and territorial health ministries, we included all positions at or above the level of assistant deputy minister listed on the ministry’s website. We excluded individuals who were publicly elected and those who did not have a colour photo available online.
Data management and extraction
Six reviewers conducted screening and data extraction using a standardized form, which enabled uniform data extraction. All information was extracted in duplicate. Reviewers were assigned a list of health care institutions via a random number generator. Variables collected were type of health care organization, hospital postal code, executive role, full listed name, perceived race, perceived gender and hyperlinks to the institutional website and to the online photo. Categories for perceived race from which reviewers could choose included “Indigenous,” “South Asian,” “Southeast/East Asian,” “Middle Eastern,” “Latinx,” “Black” and “White,” as defined in recent Canadian guidelines on reporting race in research.33 Categories for perceived gender were “Man” and “Woman.” The conflict resolution process for paired data collection is outlined in Appendix 1, Supplementary Method 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211340/tab-related-content.
Perceived race and gender
Reviewers used the names and photos on institutional websites to determine perceived race and gender. In cases where photos were not available on organization sites, professional websites (e.g., LinkedIn, university profiles) or media articles were used to obtain photos corresponding to the relevant names on the institutional website.
We asked reviewers to code an individual’s perceived gender and race based only on the photo and name to best approximate the way an individual would be perceived upon first introduction. First impressions, or assumptions made rapidly and often unconsciously on the basis of external appearance, strongly affect valuation of a person.34 As such, perception of a person’s physical appearance and name is an important way to study the social impacts of racialization and gendering.29,35–37 We used perceived race and gender measures to understand how individuals applying for health leadership roles would be initially viewed by a selection committee. This study was designed by a diverse research team that included South Asian, Indigenous, Middle Eastern, Latinx, and South East Asian individuals. The race and gender of reviewers are presented in Appendix 1, Supplementary Table 1. Definitions of race and gender, and additional information on our perceived race and gender methodology, are presented in Appendix 1, Supplementary Method 2.
We acknowledge that perceived race and gender do not always align with self-identity,29,37 particularly for Indigenous Peoples, who may be incorrectly perceived as white.38 Data on self-identified gender and race were not available because, to our knowledge, they have not been collected systematically.
Statistical analysis
To determine inter-rater reliability, we calculated the Cohen κ statistic and percent agreement for perceived race and gender between reviewers. We calculated the number and proportion of leaders by perceived race and gender category for overall data, ministry data and by province or territory. We also incorporated a “racialized” category that included all individuals who were not perceived as white. We excluded individuals for whom reviewers could not reach a consensus on race or gender for that specific category only (e.g., if perceived race was listed as “unsure,” by 1 reviewer, but gender was agreed upon by both reviewers, then that individual would not be counted in the race analysis, but would be counted in the gender analysis). If reviewers agreed that an individual was not white but could not agree on a specific racial category, the individual was included in the “racialized” category, but not for any specific racial group. To minimize identifiability, we chose to report data as fewer than 5, where applicable, in accordance with the small cell reporting practices used by groups such as ICES.39 We do present cell sizes equal to 0, as this does not risk individual identification.
To compare the racial diversity in leadership positions with the population at large, we conducted exact binomial tests and compared leadership data with population race demographics from the 2016 Canadian Census at the local, provincial and national levels. Methods for comparison of hospital leadership with the population of surrounding areas are detailed in Appendix 1, Supplementary Method 3. We merged certain Census categories to be comparable to the perceived race categories, as outlined in Appendix 1, Supplementary Table 2.
Ethics approval
Ethics approval was waived by the Unity Health Toronto Research Ethics Board as the information collected is publicly available.
Results
We initially included 3333 hospital or health ministry executives from 135 institutions across Canada (Appendix 1, Supplementary Figure 1). Photographs were identified for 3056 (91.6%) of these executives, which constituted the sample used for this analysis. Overall inter-rater reliability was high, with a 96.4% match rate for perceived race (Cohen κ = 0.81) and a 98.9% match rate for perceived gender (Cohen κ = 0.98) (Appendix 1, Supplementary Table 3). Inter-rater reliability varied between perceived racial categories of health care leaders (κ range 0.30–0.88).
Concordance on perceived gender was achieved for 3022 individuals (98.9%). Reviewers perceived gender as “woman” for 37 (47.4%) of 78 leaders at the ministry level, 36 (50.0%) of 72 leaders in provinces with centralized hospital systems (Alberta, Saskatchewan, Prince Edward Island, Nova Scotia) and 120 (56.1%) of 214 leaders in provinces with regional hospital systems (BC, New Brunswick, Newfoundland and Labrador) (Table 1). In Manitoba, Ontario and Quebec, where leadership exists at the individual hospital level, 1326 (49.9%) of 2658 executives were perceived as women (Table 1).
Perceived gender and race of hospital and health ministry executives
Race was concordantly perceived in 2946 individuals (96.4%). At the ministry level, fewer than 5 (< 7%) of 80 leaders were perceived as racialized (Table 1). Five (7.1%) of 70 leaders in centralized hospital provinces, 24 (11.5%) of 209 leaders in regional hospital provinces and 243 (9.2%) of 2633 leaders in individual hospital provinces were perceived as racialized (Table 1). Perceived race by category is presented in Appendix 1, Supplementary Table 4.
Across the country, no leaders in health ministry positions were perceived as racialized women, and this group comprised 5% or fewer of hospital leaders in all provinces, with the exception of BC (Table 1). Where estimates of race and gender were not limited by sample size, we did not see a consistent pattern of further proportional limitations for racialized women. Specifically, in provinces with regional hospital systems, the proportion of leaders perceived as racialized was 11.5%, and 7.2% of leaders were perceived as both racialized and women; in provinces with individual hospital leadership, these proportions were 9.2% and 3.8%, respectively.
Across Canada, 5 (41.7%) of 12 deputy ministers and 61 (51.7%) of 118 hospital presidents or chief executive officers (CEOs) were identified as women (Table 2). Individuals perceived as racialized held 7 (5.9%) of the 118 highest-level hospital leadership roles in the country, and those coded as both racialized and women held fewer than 5 of these roles (Table 2). No deputy ministers were perceived as racialized.
Perceived race and gender of deputy ministers and hospital presidents or chief executive officers (CEOs) across Canada*
At the provincial level, the gap between hospital executives perceived as racialized compared with the self-identified racialized population was 14.5% for BC (23.3% v. 37.8%), 27.5% for Manitoba (8.4% v. 35.9%), 20.7% for Ontario (12.7% v. 33.4%), 12.4% for Quebec (3.4% v. 15.8%), 7.6% for New Brunswick (0.0% v. 7.6%), 7.3% for Prince Edward Island (0.0% v. 7.3%) and 11.6% for Newfoundland and Labrador (0.0% v. 11.6%) (Table 3). The percentage of racialized leadership was not significantly affected by the size of the leadership team (Appendix 1, Supplementary Table 5).
Proportion of leaders perceived as racialized compared with the proportion of the general population that self-identified as racialized
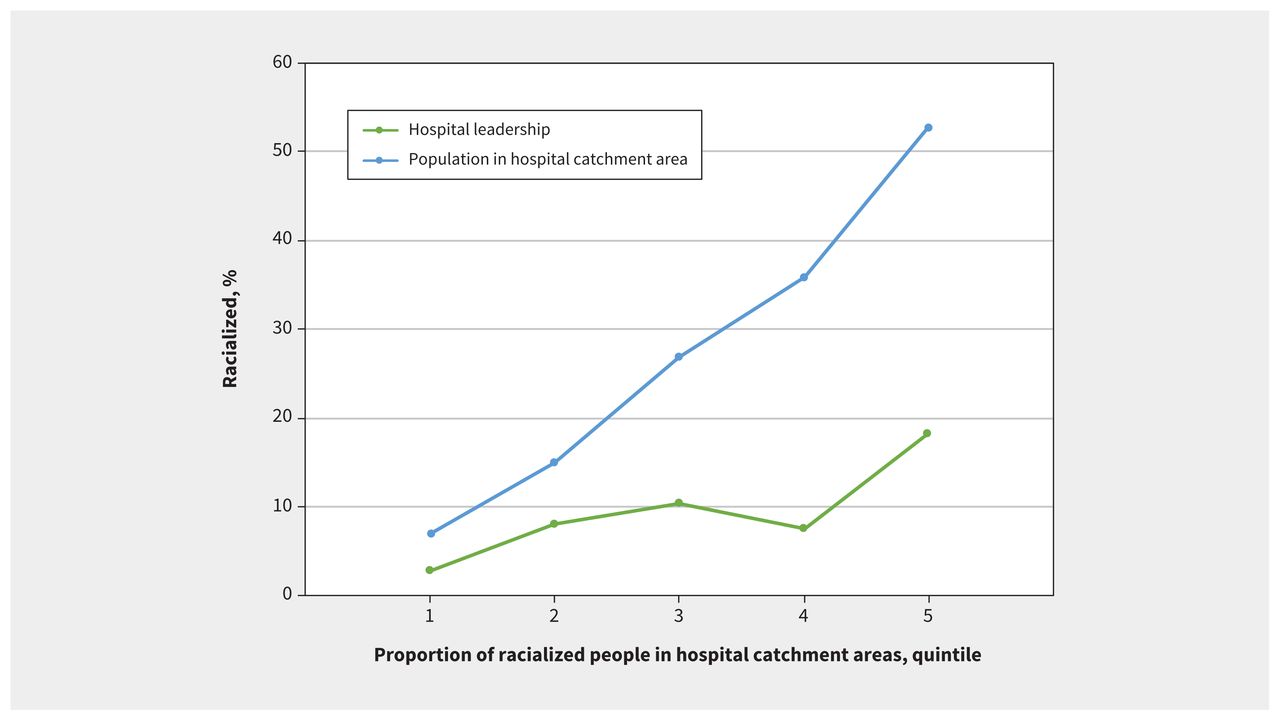
In Manitoba, Ontario and Quebec, we analyzed the gap in racial diversity between hospital leadership and the municipal population (Figure 1). The gap in representation increased from 4.2% in cities or towns with the lowest proportion of racialized residents to 34.5% in areas with the highest proportion of racialized residents. The trend was similar when geographic catchment areas were narrowed using alternate definitions (Appendix 1, Supplementary Table 6).
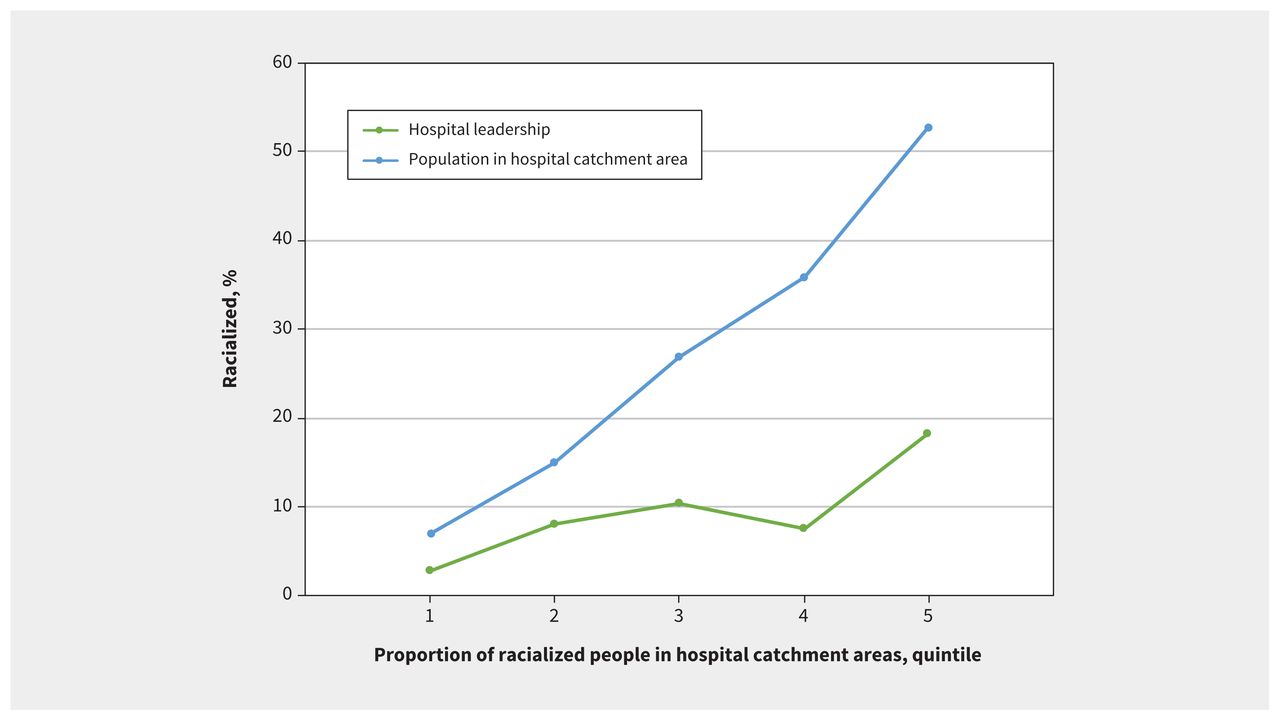
Proportion of hospital leadership perceived as racialized compared with proportion of local population that self-identified as racialized, by municipality in Manitoba, Ontario and Quebec. Municipality is defined by Census subdivision catchment area. Quintiles divide hospitals and their surrounding municipalities equally into 5 categories based on the proportion of racialized population in the area, from lowest (in quintile 1) to highest (in quintile 5).
Interpretation
In a national study of more than 3000 health care leaders in Canada, we found gender parity among ministry and hospital leaders, but substantial disparities between racial diversity of health care leaders and the diversity of the communities they serve. Comparison with provincial and national population demographics revealed that racialized individuals are considerably under-represented in health care leadership across the country. In provinces where leadership exists at the individual hospital level, we found that these gaps were wider in more racially diverse neighbourhoods. Very few leaders perceived as racialized have attained the highest-ranking positions of CEO or deputy minister in Canadian health care systems.
The gap in racial representation among leadership is likely influenced by several factors. Fewer racialized individuals may attain leadership positions owing to a proportionally smaller number of racialized people in the hiring pool, decreased access to mentorship opportunities and discriminatory hiring practices. Previous literature and numerous public examples suggest that racism is deeply embedded in our health care institutions.40,41 Racialized groups in Canada, most notably Black and Indigenous people, have worse health outcomes than the general population. 42,43 A lack of diverse representation in health care leadership may exacerbate health disparities for racialized patients.3,7
Racial diversity in leadership can be beneficial for several reasons. People from racially marginalized groups can share insights to inform perspectives on racial inequity and invoke empathy among health care leaders.12,44 A racially diverse leadership executive may be more likely to promote culturally sensitive care by addressing discriminatory policies, creating inclusive spaces for patients and fostering a culture of antiracism among staff.7,45,46 Diverse leadership is thought to improve patient experiences and may improve clinical outcomes.6,7 Further, evidence suggests that when patients see their race represented in their health care providers, they are more likely to have positive care experiences47 and agree to essential preventive care.48 To avoid tokenism,49,50 institutions must ensure inclusion alongside diversity and ensure that racialized leaders not only have a seat at the table, but also have an equal voice in decision-making within executive leadership.51
The observed gender balance between men and women in health care leadership provides a marked contrast to the under-representation of racialized people. Gender diversity in leadership can enhance patient outcomes and cultivate creativity in addressing complex health care challenges.52 We found that women and men hold equal numbers of hospital CEO positions across the country. This finding is welcome progress considering the large body of evidence highlighting the difficulties that women face in advancing in their careers,53,54 but it does not discount the ongoing effects of gender-based discrimination in health care that require continued advocacy.
Limitations
This study is limited in its measurement of perceived race and gender. Self-identified and observed characteristics can differ,29,37 and misclassification is particularly harmful to Indigenous communities in Canada.55–57 Self-identification is a central concept for Indigenous people, rather than having Indigeneity determined by others who are not Indigenous and who may uphold colonial constructions of Indigenous Peoples. Systemic and interpersonal misclassification of Indigenous people as white continues,58,59 and this process denies Indigenous Peoples their identity, culture and history.38 Incorrectly assuming a person’s gender in a binary classification system can be similarly damaging to gender-diverse people.60,61 Our perception-based coding method may lead to a falsely low representation of racialized and Indigenous groups, and of nonbinary people, in executive positions.
This study focused on identifying disparities among perceived racial groups, but it is important to acknowledge that differences within perceived racial groups may also exist. The groups included within the “racialized” category in our study, as well as individuals within specific racial groups, have distinct experiences of racism and discrimination. For example, first-generation immigrants who speak with an accent deemed as “other” are more likely to experience race-based discrimination in the workplace.62,63 We were unable to collect data pertaining to immigration status, though evidence suggests that it may be particularly difficult for first-generation immigrants to attain leadership positions.64,65 Transparent reporting of the self-reported race, country-of-origin and gender composition of health leadership teams by Ministries of Health and large health care organizations would enable more nuanced research. This demographic reporting could track the progress of interventions aimed at achieving more diverse leadership. 66,67 However, as previously argued, perceived race and gender remain important measures in evaluating social outcomes.
Given the differing structures of leadership teams across Canada, our study is limited in sample size for provinces with regional or provincially structured hospital executives. In these cases, the comparison between the leadership team(s) and the population they serve is more difficult to interpret. The lack of congruence between measures of perceived race of leaders, which is subject to misclassification, and self-identified race for the general population may overestimate or minimize gaps in representation. However, when taken together, our findings provide a consistent story regarding gaps in representation of racialized groups across Canada.
The use of publicly available websites to quantify leadership team characteristics may reduce reproducibility as these sources are subject to change. This method required that we exclude individuals without an online photo. It is possible that racialized individuals, women and nonbinary people are more or less likely than others to choose to display their photo online. Reproducibility and validity may also be affected by the reviewers’ own race and gender, which may affect perception of the race and gender of others,68,69 though our duplicate coding process mitigates this area of bias. In future studies, this limitation could be addressed further by including Black and Indigenous reviewers.
Conclusion
Our study showed gender parity but substantial under-representation of racialized individuals in Canadian health care leadership. Given calls to address systemic racism in Canada’s health care systems, increasing racial diversity and inclusion in leadership teams and improving data collection to support this aim are clear ways for institutions to take action.
Footnotes
Competing interests: Dan Werb reports grants from the Canadian Institutes of Health Research and St. Michael’s Hospital Foundation, as well as a pending patent for a drug-checking device, outside the submitted work. Gillian Hawker is supported as the Sir John and Lady Eaton Professor and Chair of Medicine. Amol Verma reports salary support from the AMS Healthcare Fellowship in Compassion and Artifical Intelligence and the St. Michael’s Hospital Clinician–Surgeon Scientist Stipend Award, as well as part-time employment with Ontario Health as Provincial Clinical Lead for Quality Improvement in General Internal Medicine. Fahad Razak holds a salary award as the Graham Farquharson Knowledge Translation Fellow from the PSI Foundation and is an employee of Ontario Health. All competing interests exist outside the submitted work. No other competing interests were declared.
Contributors: Anjali Sergeant, Arti Dhoot, Dan Werb, Nazlee Maghsoudi, Lisa Richardson, Gillian Hawker, Arjumand Siddiqi, Amol Verma and Fahad Razak conceived and designed the study. Anjali Sergeant, Sudipta Saha, Anushka Lalwani, Anand Sergeant, Avery McNair, Elias Larrazabal, Kelsey Yang and Orly Bogler contributed to data acquisition, analysis and interpretation. Anjali Sergeant and Sudipta Saha drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study did not receive any funding.
Data sharing: To enable similar research in the future, the authors created a repository of all institutions and their corresponding websites. Individuals who are interested in accessing data for research purposes may contact the corresponding author.
- Accepted December 17, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article extras
Article tools



Jump to section
Related Articles
Cited By...
- "To tell you the truth Im tired": a qualitative exploration of the experiences of ethnically diverse NHS staff
- The Creating Brave Spaces workshop: a report on simulation-based faculty development to disarm microaggressions
- Gender and racialisation of pharmaceutical sector leaders in Canada: a cross-sectional study
- Representation and reconciliation--Indigenous leadership for health in Canada
More in this TOC Section
Similar Articles
Collections

