


Technology: Anti-inflammatory therapy for the treatment of septic shock
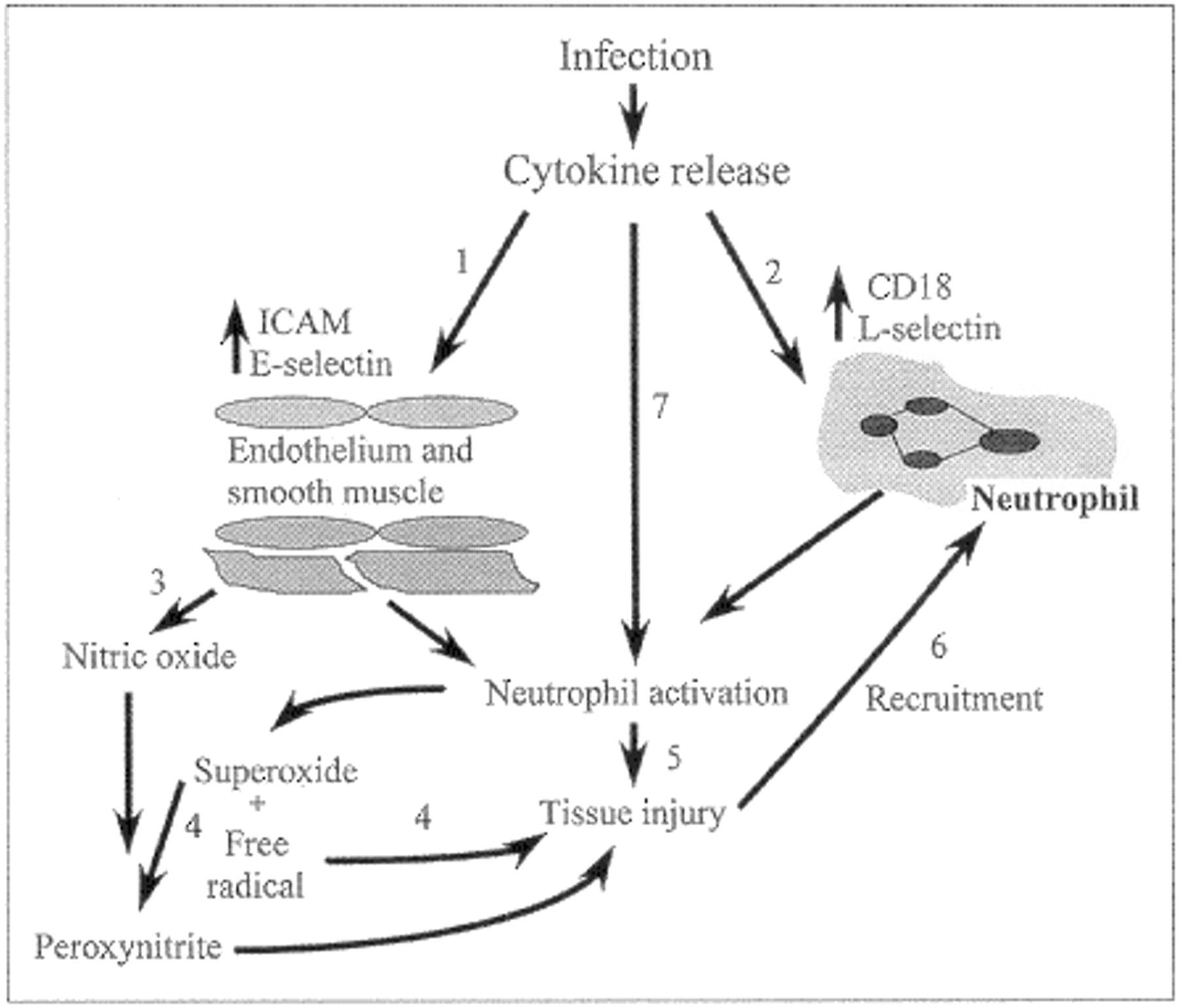
Use: Sepsis or septic shock, which occurs when the host's response to infection is excessive, is the fourth leading cause of long-stay intensive care admissions.1 Death may occur despite antimicrobial therapy2 if the host response to infection is either excessive or insufficient (Fig. 1); in fact, mortality has been reported to be as high as 45% 5 months after the onset of septic shock. Thus, the aim of therapeutic intervention for sepsis is to rebalance the complex series of interrelated inflammatory mediators (Fig. 2). When the initial infection occurs, inflammatory mediators (e.g., IL-6, TNFα) are released; these mediators then upregulate receptors on neutrophils (e.g., CD11, CD18) and endothelial cells (ICAM-1). Concurrently, other effector molecules are released (e.g., peroxynitrite) that cause organ damage and further recruit activated neutrophils to the site of injury. The schema shown in Fig. 2 is not all-inclusive, but outlines various aspects of the inflammatory response in which the down-regulation of mediators might benefit the patient. The ultimate aim is to prevent sepsis-related multiple organ failure, the primary cause of death, and therefore improve both survival rates and quality of life and, incidentally, decrease hospital resource utilization.
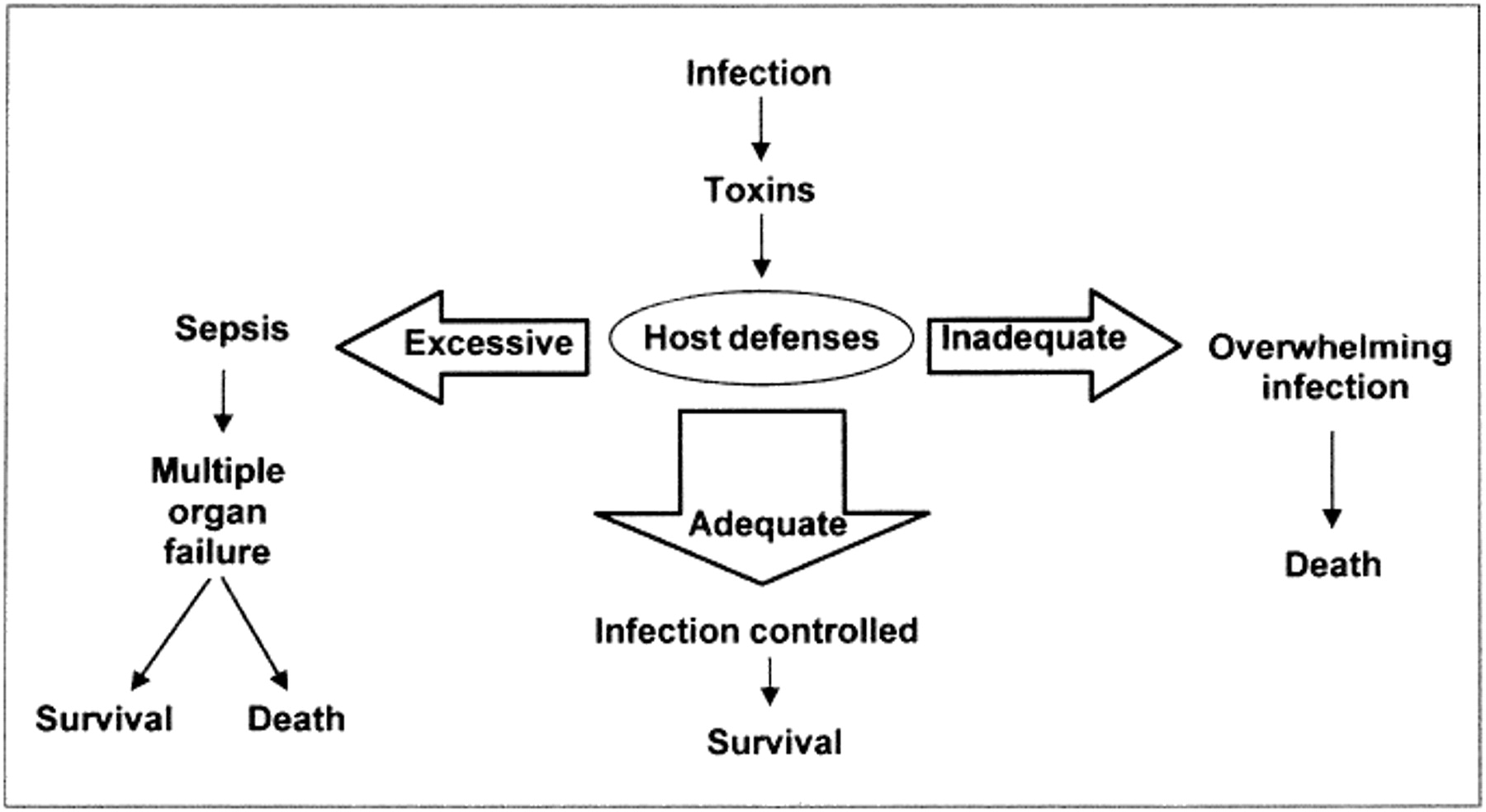
Fig. 1: The delicate balance for an appropriate host response to infection. Either an excessive or an insufficient response may lead to death or disability.
{kind=link}
{kind=link}
Fig. 2: Selected aspects of the inflammatory response to infection. The opportunities to regulate specific steps of the inflammatory cascade are numbered as follows: 1, inhibition of endothelial-adhesion receptors; 2, inhibition of neutrophiladhesion receptors; 3, inhibition of excess nitric oxide production; 4, free radical and superoxide scavengers; 5, blockade of neutrophil proteases; 6, prevention of further neutrophil recruitment; 7, blockade of upstream cytokine activation. ICAM = intercellular adhesion molecule-1.
History: The use of anti-inflammatory agents for the symptomatic relief of infection dates back to the use of ASA to reduce fever. One of the early randomized controlled clinical trials conducted to evaluate the effect of an anti-inflammatory agent on the severity and incidence of sepsis in a high-risk population3 concluded that methylprednisilone was associated with a poorer outcome and increased mortality rates when compared with placebo. Many other anti-inflammatory agents, ranging from intravenous ibuprofen4 to an inhibitor of the pro-inflammatory cytokine TNFα,5 have since been evaluated for the treatment of septic shock, but none have proved to be successful therapeutic interventions to date.
Promise: When multiple organ failure is established, extensive medical support is required until the excessive inflammatory response dampens. These supportive therapies may include mechanical ventilation (for acute lung injury), intravenous pressors or fluids (for cardiac failure), hemodialysis (for acute renal failure), total parenteral nutrition (for acute gut injury) or sedation (for acute brain dysfunction). It is hoped that early intervention with selective anti-inflammatory therapy or with a combination of the appropriate agents at different times (according to the severity of sepsis) will reduce inflammation, preserve organ function and result in an increase in survival rates and a decrease in the utilization of hospital resources.
Problems: Our knowledge of the complex interactions that occur during an inflammatory response to infection is still lacking. Issues still to be addressed include how to achieve the appropriate balance between an inadequate response (which may result in death) and an excessive one (which can lead to sepsis and death) and when and to what extent the interaction between the infecting organism and the host should be manipulated. For example, should the inflammatory response associated with streptococcal toxic shock and with gram-negative bacteremia be down-regulated to the same extent? In addition, patients with sepsis are diagnosed and treated at different times in the course of their illness. Anti-inflammatory therapy may be similar to other time-sensitive treatments (e.g., thrombolysis for acute myocardial infarction and stroke), where only a finite window of time exists in which a specific treatment will be therapeutic.
Prospects: Cloned proteins and monoclonal antibodies are among the new therapeutic agents being developed that may regulate specific steps of the inflammatory response. Bedside tests to rapidly measure specific elements of the inflammatory cascade (e.g., IL-6) are also under development. Thus, it may become possible to adjust anti-inflammatory therapy in response to specific biochemical changes in the cascade. The ultimate extension of this approach would see patients with septic shock receiving moment-to-moment titration of specific anti-inflammatory agents, with the type and amount of medication administered based on continuous bedside measurements of inflammatory mediators.
Competing interests: None declared.
Acknowledgments
CMAJ reaches more Canadian GPs than any other medical journal
In this issue
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
Similar Articles

