


Statins (HMG-CoA reductase inhibitors) have been used for the treatment of hypercholesterolemia and coronary artery disease for more than a decade. Their efficacy and safety have been well documented in a number of large primary and secondary clinical trials.1,2,3,4 Their mechanism of action is the inhibition of the rate-limiting enzyme of cholesterol synthesis, namely, HMG-CoA reductase.5 In addition to their well-known cholesterol-lowering properties, other effects of statins have been noted. These were recently reviewed by Davignon and Laaksonen.6
Mundy and colleagues7 were the first to report that incubation of cultured mouse or human bone cells with statins enhanced the expression of bone morphogenetic protein-2 (BMP-2) mRNA. Incubation with 2.5 μmol simvastatin increased the production of the protein by 2.7 times in human bone cells. BMP-2 is an important mediator in osteoblast differentiation and bone formation. In subsequent experiments, Mundy and coworkers added various statins to neonatal mouse calvarial bones in organ culture. Each statin that was tested increased new bone formation by approximately 2–3 times. They confirmed these results in vivo in mice: a course of 3 subcutaneous injections per day over 5 days over the calvaria produced an increase of about 50% in new bone formation. Similarly, 35-day oral administration of simvastatin (5–50 mg/kg per day by gastric gavage) to both intact and ovariectomized rats resulted in increases of 39%–94% in trabecular bone volume.7 A parallel increase in bone formation rates was noted, indicating significant anabolic effects of the statin treatment. These anabolic effects were associated with a decrease in osteoclast numbers.7 These provocative experimental findings paved the way for observational studies of the association between statin use and quality of bone in both men and women.8,9,10,11,12
Meier and colleagues8 enrolled a total of 3940 subjects with fractures and 23 379 control subjects from the UK-based General Practice Research Database in a nested case–control study to determine whether lipid-lowering treatment was associated with a reduced risk of fractures. This study showed that current use of statins, but not other lipid-lowering agents, was associated with a significant reduction in fracture risk (adjusted odds ratio [OR] 0.55). It is of interest that this beneficial effect of statins was also observed after a relatively short course of treatment of a few weeks to a few months.
Another large observational study was carried out by Wang and coworkers9 of elderly patients. In this case–control study, the use of statins was associated with a significant reduction in the risk of hip fracture in 1222 case subjects who had undergone surgical repair of a hip fracture compared with 4888 control subjects. Such an association was not observed with other lipid-lowering agents. Moreover, this study showed a clear relationship between the degree of reduction in risk of fracture and the extent of statin use. Similarly, postmenopausal women with a minimum of 13 or more statin prescriptions had a significantly decreased risk of nonpathological fracture (adjusted OR 0.48) compared with controls.10
Chung and colleagues11 studied the effects of 3 statins (lovastatin, pravastatin, simvastatin) on bone mineral density (BMD) in a total of 69 patients with type 2 diabetes (33 controls and 36 treated). After 15 months, the treated subjects showed a statistically significant increase in BMD of the femoral neck, femoral Ward's triangle, femoral trochanter and total hip. This increment in BMD remained significant after adjustment for age and body mass index. Similarly, Bauer and coworkers12 also reported increased hip BMD, along with reduced fracture risk (relative risk 0.53, 95% CI 0.07–3.82), in association with statin use in elderly women.
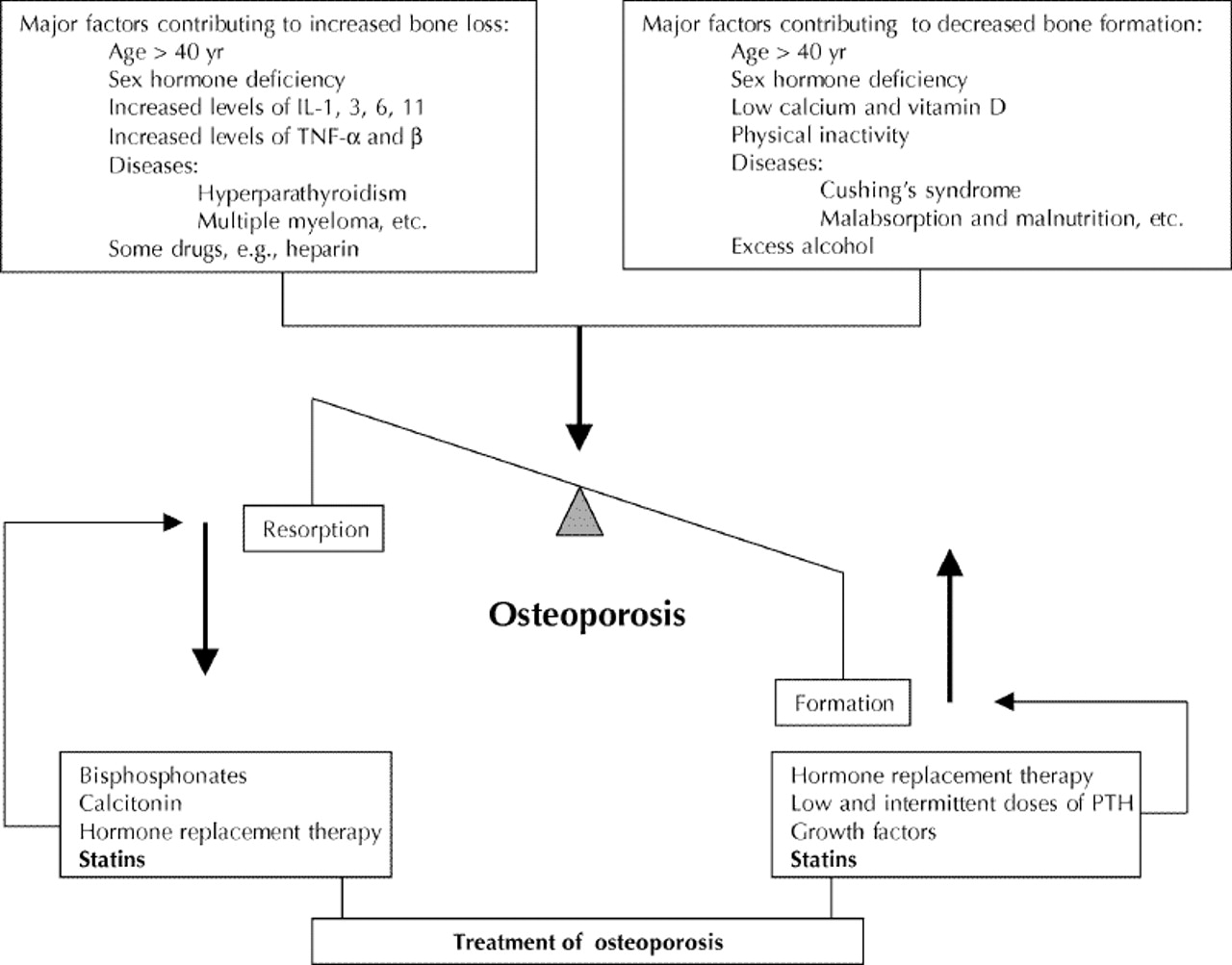
At least 20% of women older than 50 years suffer from osteoporosis; bone fractures due to osteoporosis occur in approximately 1.5 million individuals in the United States annually.13 Several pharmacological interventions are currently used to modulate the rate of bone remodelling in osteoporosis.14,15,16,17,18 The concept of bone remodelling and current interventions are summarized in Fig. 1. Among therapeutic agents, both nitrogen-containing bisphosphonates (N-BPs) and statins interfere with the mevalonate cholesterol biosynthesis pathway, albeit at 2 different points. In addition, N-BPs can directly induce apoptosis of osteoclasts through a number of intracellular mechanisms,19 whereas statins, as previously discussed, induce an increase in expression of BMP-2 mRNA and protein.7,20 Thus, as well as inhibiting the mevalonate pathway, statins and N-BPs may produce dual benefits in the prevention of bone fracture by stimulation of bone formation and inhibition of bone resorption.7,19,20,21,22

{kind=link}
Fig. 1: Excessive osteoclastogenesis and inadequate osteoblastogenesis are the primary reasons for osteoporosis. Agents with antiresorptive and anabolic properties are ideal for restoring the physiological remodelling cycle. Preliminary evidence shows such potential for statins, which act by increasing bone formation and inducing osteoclast apoptosis. IL = interleukin, TNF = tumour necrosis factor, PTH = parathyroid hormone.
Yet another interesting possibility exists to explain statin effectiveness. In a population-based longitudinal study of 720 postmenopausal women, Hak and colleagues23 showed that the progression of atherosclerotic calcification was associated with bone loss. The authors speculate that inflammatory agents involved in atherosclerosis may contribute to bone resorption. Thus, we may further speculate that statins by their antiatherosclerotic and anti-inflammatory effects may also modulate the redistribution of calcium between arteries and bones.24
In conclusion, several observational studies indicate that statins reduce the risk of bone fracture. This significant unanticipated effect appears to be independent of cholesterol lowering, because it was not observed with other cholesterol-lowering agents. However, it should be noted that the findings of observational studies may not be always reproducible in prospective, randomized trials. Therefore, recommendations for the use of statins in the prevention of bone fractures must await the outcome of well-designed, large-scale, prospective, randomized trials. Appropriate studies are also needed to determine for how long statin treatment should continue and who benefits the most. Because statins do not accumulate significantly in bones, several pharmacokinetic features of currently available statins such as their formulations, route of administration and dosing may be modified to enhance their efficacy in improving the rate of bone remodelling, without compromising their other beneficial effects. The mode of action of statins and the nature of the newly formed bone tissues merit full investigation, as do the effects of statins on bone strength and fracture healing. Finally, the potential advantages of statins over other approaches with regard to their efficacy, safety, cost-effectiveness and patient compliance will have to be evaluated.
Footnotes
-
Contributors: Both authors contributed equally to the writing of this article.
Competing interests: None declared for Dr. Moghadasian. Dr. Frohlich has served as a consultant to all companies dealing with lipid-lowering agents and has occasionally accepted compensation for himself or for his department's trust fund.
References
In this issue
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

