


Abstract
Background: Published decision analyses show that screening for colorectal cancer is cost-effective. However, because of the number of tests available, the optimal screening strategy in Canada is unknown. We estimated the incremental cost-effectiveness of 10 strategies for colorectal cancer screening, as well as no screening, incorporating quality of life, noncompliance and data on the costs and benefits of chemotherapy.
Methods: We used a probabilistic Markov model to estimate the costs and quality-adjusted life expectancy of 50-year-old average-risk Canadians without screening and with screening by each test. We populated the model with data from the published literature. We calculated costs from the perspective of a third-party payer, with inflation to 2007 Canadian dollars.
Results: Of the 10 strategies considered, we focused on three tests currently being used for population screening in some Canadian provinces: low-sensitivity guaiac fecal occult blood test, performed annually; fecal immunochemical test, performed annually; and colonoscopy, performed every 10 years. These strategies reduced the incidence of colorectal cancer by 44%, 65% and 81%, and mortality by 55%, 74% and 83%, respectively, compared with no screening. These strategies generated incremental cost-effectiveness ratios of $9159, $611 and $6133 per quality-adjusted life year, respectively. The findings were robust to probabilistic sensitivity analysis. Colonoscopy every 10 years yielded the greatest net health benefit.
Interpretation: Screening for colorectal cancer is cost-effective over conventional levels of willingness to pay. Annual high-sensitivity fecal occult blood testing, such as a fecal immunochemical test, or colonoscopy every 10 years offer the best value for the money in Canada.
See related commentary by Smith, page 1283, and also research article by Simunovic and colleagues, page 1301
Colorectal cancer is the fourth most common cancer diagnosed in North America and the second leading cause of cancer death. 1,2 An effective population-based screening program is likely to decrease mortality associated with colorectal cancer 3–6 through earlier detection and to decrease incidence by allowing removal of precursor colorectal adenomas. 7,8 Professional societies and government-sponsored committees have released guidelines for screening of average-risk individuals for colorectal cancer by means of several testing options. 9–12 These tests vary in sensitivity, specificity, risk, costs and availability. With no published studies designed to directly compare screening strategies, decision analysis is a useful technique for examining the relative cost-effectiveness of these strategies. 13–21 Previous studies have shown that screening for colorectal cancer is cost-effective at conventional levels of willingness to pay, but no single strategy has emerged as clinically superior or economically dominant. 22 The interpretations of economic evaluations in this area have been limited because investigators have not simultaneously accounted for the positive effects of screening on quality of life, the effect of noncompliance with screening schedules, and the greater efficacy and cost of more modern chemotherapy regimens for colorectal cancer. Furthermore, no study has included all of the strategies recommended in the 2008 guidelines of the US Multi-Society Task Force on Colorectal Cancer. 10
Our objective was to estimate the incremental cost-effectiveness of 10 strategies for colorectal cancer screening, as well as the absence of a screening program. The current study is more complete than earlier studies because we included information on quality of life, noncompliance with screening and the efficacy observed in recent randomized trials of colorectal cancer treatments. The complete model is available in Appendix 1 (available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1). This article focuses on the comparison of no screening and three screening strategies: 1 low-sensitivity guaiac fecal occult blood test, 2 performed annually; fecal immunochemical test, 3 performed annually; and colonoscopy, performed every 10 years. These three tests are currently being used or considered for population-based screening of average-risk individuals in some Canadian provinces.
Methods
Model design
We developed a Markov model using TreeAge DATA Pro (TreeAge Software Inc., Williamstown, Mass.) to estimate the cost-effectiveness of 10 strategies for screening, as well as no screening, in 50-year-old individuals at average risk for colorectal cancer (Table 1). Screening and surveillance continued until 75 years of age, and the analysis continued through the lifetime of the cohort. The length of the model cycle (or, equivalently, the duration over which an individual remained in the same health state before having the opportunity to transition to another health state) was one year. We calculated costs from the perspective of a third-party payer such as a provincial ministry of health and inflated these costs to 2007 Canadian dollars. The model output was quality-adjusted life-years. We discounted costs and effects at 5% annually and used a half-cycle correction to account for these discounts.
Table 1: Strategies to screen for colorectal cancer
We simulated the natural history of colorectal cancer (Figure 1). We calibrated the input parameters of incidence and progression of adenoma to colorectal cancer to generate the known age-specific prevalence of adenomas and colorectal cancer (Appendix 2, available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1). We obtained probabilities of transition between health states, utilities and costs from the published literature by searching MEDLINE; reviewing the reference lists of the papers identified in the MEDLINE search; and searching the Surveillance, Epidemiology, and End Results database. We searched publicly available data for costs and other model inputs (including Canadian life tables 23 and the Ontario Health Insurance Plan Schedule of Benefits and Fees 24). The model design and analyses are described in more detail in Appendix 1 (available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1).

Figure 1: Markov states for the natural history of colorectal cancer. Individuals transitioned to different Markov health states (straight arrows) or remained in their current health state (curved arrows). Transitions occurred yearly from age 50 years to death. The Markov model contained three precancer states, three preclinical (undiagnosed) cancer states, three diagnosed cancer states and the absorbing health state of death. After treatment of colorectal cancer, individuals entered a surveillance health state with the opportunity for development of further adenomas and cancer. The 10 screening strategies were superimposed on the natural history model.
Analyses
We estimated the incremental cost-effectiveness ratios for each strategy. The numerators were the differences in costs for each strategy relative to the preceding strategy (ranked in order of effectiveness), and the denominators were the differences in quality-adjusted life-years in hypothetical cohorts of 100 000 individuals undergoing screening. We used deterministic and probabilistic sensitivity analyses to assess uncertainty associated with the input parameters. We also calculated net health benefits, which are presented in cost-effectiveness acceptability curves. 25,26
Results
Base-case analysis
In the base case (50-year-old individuals at average risk for colorectal cancer participating in one of the screening strategies or no screening), the mean number of life-years ranged from 31.08 for no screening to 31.47 for colonoscopy every 10 years. After adjustment for the utility and discount on future life-years, the mean number of discounted, quality-adjusted life-years ranged from 15.20 for no screening to 15.32 for colonoscopy every 10 years, with the mean discounted cost of screening for and treating colorectal cancer ranging from $783 for no screening to $1529 for colonoscopy every 10 years (Table 2). All 10 screening strategies for colorectal cancer increased the number of quality-adjusted life years and were more costly than not screening (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1).
Table 2: Results from the base-case analysis*
Of the three screening tests currently used in Canada, colonoscopy every 10 years was both the most effective and the most costly strategy (Figure 2). The cost of annual performance of the fecal immunochemical test was slightly more than the cost of annual performance of the low-sensitivity guaiac fecal occult blood test and yielded a higher quality-adjusted life expectancy. The incremental cost per quality-adjusted life-year gained for colorectal cancer screening ranged from $611 with annual fecal immunochemical testing through $6133 for colonoscopy every 10 years to $9159 for annual low-sensitivity guaiac fecal occult blood testing.

Figure 2: Cost-effectiveness plane for not screening and for three strategies for colorectal cancer screening. The graph plots the cost of the various strategies against average discounted quality-adjusted life expectancy.
Table 3 shows the decrease in incidence and mortality associated with colorectal cancer in hypothetical cohorts of 100 000 average-risk persons starting each strategy at age 50 years. In the cohort not undergoing screening, colorectal cancer was diagnosed in 6257 individuals during their lifetimes, and 3814 died of this disease. In cohorts undergoing screening, the decrease in mortality rate associated with colorectal cancer ranged from 55% for annual low-sensitivity guaiac fecal occult blood test to 83% for colonoscopy every 10 years, and the decrease in incidence of colorectal cancer raned from 44% for annual low-sensitivity guaiac fecal occult blood test to 81% for colonoscopy every 10 years. The cost (in 2007 Canadian dollars) to screen 100 000 individuals ranged from about $63 million to about $76 million dollars over the lifetime of the cohort.
Table 3: Cost and effectiveness of three strategies for screening for colorectal cancer over the lifetime of 100 000 individuals who commence screening at age 50 years, relative to not screening
Sensitivity analysis
The one-way and probabilistic sensitivity analyses and net benefits analysis comparing all 10 colorectal cancer screening strategies and no screening are available in Appendix 1 (available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1). In the one-way sensitivity analysis, the model was sensitive to variations in sensitivity of the test to detect advanced adenoma, cost of the test, compliance with screening and cost of cancer care.
In general, as the sensitivity of the test to detect advanced adenomas rose, the cost of the strategy decreased and its effectiveness increased. For instance, if the sensitivity for advanced adenomas was greater than 56% for the fecal immunochemical test or less than 17% for the lowsensitivity guiaic fecal occult blood test, then the annual fecal immunochemical test dominated. If the cost of the fecal immunochemical test rose beyond $36, then this strategy was dominated by colonoscopy performed every 10 years. In contrast, colonoscopy costing less than $360 dominated the other strategies. Under no circumstances was colonoscopy every 10 years dominated by one of the other strategies.
Decreased compliance with screening was associated with a decrease in the cost and effectiveness of a strategy. Table 4 shows the one-way sensitivity analysis of each screening test while the compliance of the other tests was held constant at 73% (the base-case value derived from the literature). When compliance with the fecal immunochemical test was less than 71% or compliance with the low-sensitivity guaiac fecal occult blood test was greater than 77%, the annual fecal immunochemical test was less costly than and dominated the annual low-sensitivity guaiac fecal occult blood test.
Table 4: Results of one-way sensitivity analysis
Increasing the cost of cancer care increased the cost of each strategy. Because of the similar costs of the fecal tests, a relatively larger increase in the cost of annual low-sensitivity guaiac fecal occult blood test led to this strategy being dominated by annual fecal immunochemical test. More informatively, when the cost of treating localized cancer was increased, the cost of strategies with a higher sensitivity for detecting advanced adenoma rose less, as a result of cancer being prevented. This effect was not seen when the cost of treating regional or distant colorectal cancer was varied.
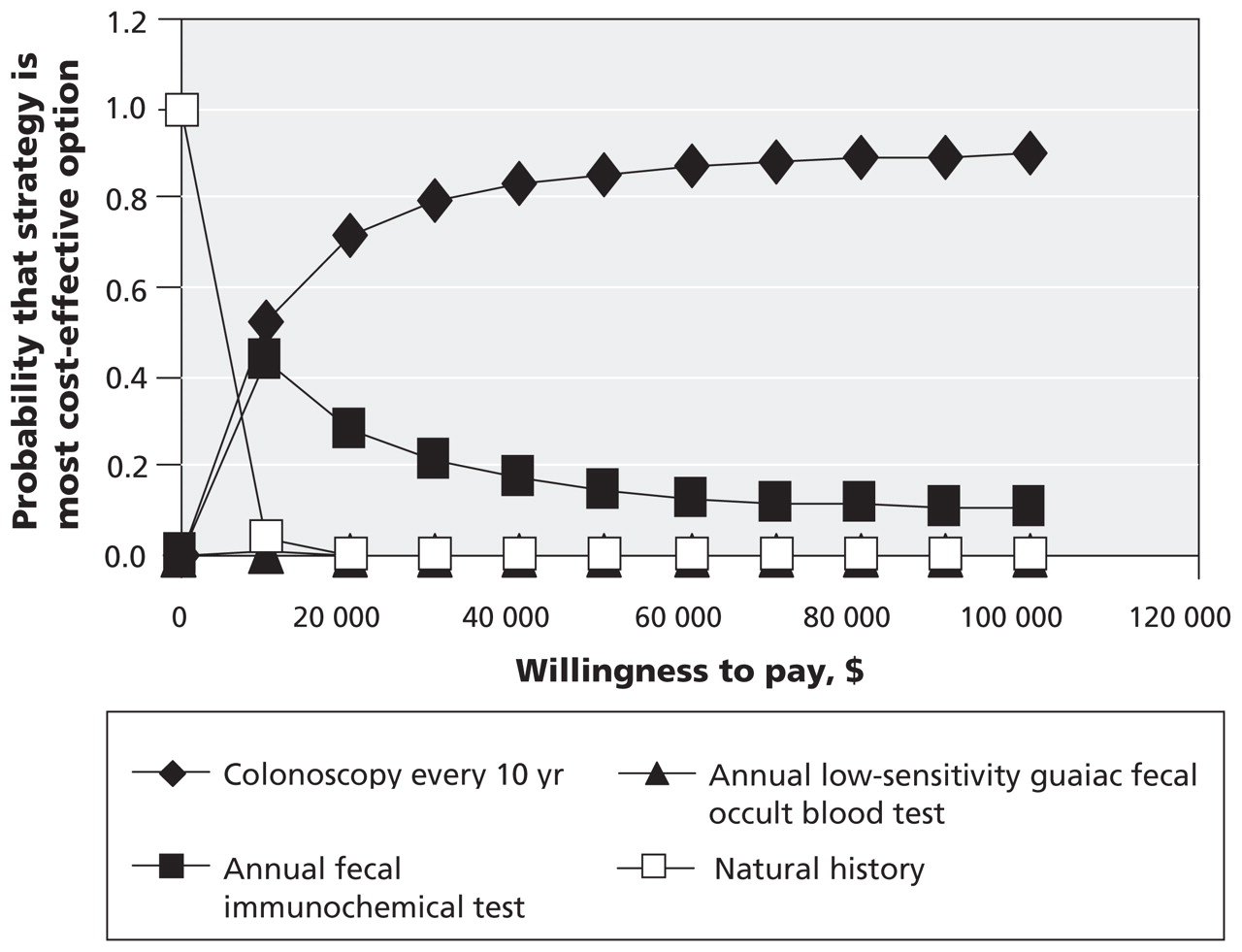
The probabilistic sensitivity analysis did not change the ranking of strategies, and no strategy was dominant (Table 5). The difference in incremental cost-effectiveness ratios from the base-case analysis (Table 3) was due to changes in the effectiveness of annual low-sensitivity guaiac fecal occult blood test, which reflected the large degree of uncertainty about test performance. At a willingness-to-pay of $50 000 per quality-adjusted life-year gained, the likelihood of the strategies being cost-effective was 85% for colonoscopy every 10 years and 15% for annual fecal immunochemical test (Figure 3). Annual low-sensitivity guaiac fecal occult blood test contributed less than 1% over a range of willingness-to-pay up to $100 000 per quality-adjusted life-year gained.
Table 5: Results from the probabilistic sensitivity analysis

Figure 3: Cost-effectiveness acceptability curve. The gain in quality-adjusted life years estimated with each strategy was adjusted for the cost and a hypothetical payer’s willingness to pay. The probability that a strategy is cost-effective (y axis) relative to alternative strategies is shown for a range of willingness to pay, up to $100 000 per quality-adjusted life-year gained (x axis).
Interpretation
Comparison with other studies
The current analysis is consistent with earlier studies 22 in demonstrating that screening for colorectal cancer is cost-effective relative to not screening, according to the conventionally accepted benchmark of willingness-to-pay of $50 000 per life-year gained. 27,28 Furthermore, the proportion of cancer cases prevented was comparable to that reported in previous studies. 22 In addition, the current model produced reductions in mortality and incidence of colorectal cancer similar to those reported from a microsimulation model of colorectal cancer 29 used to inform the 2008 US Preventive Task Force recommendations for colorectal cancer screening. 12
Limitations
This study was subject to important limitations. Model-based economic evaluation depends on the data available in the medical literature, which is constantly evolving. As new information becomes available, the results of the current analysis will have to be updated. The natural history of colorectal cancer is based on assumptions regarding the progression from adenoma to carcinoma and the transition time from a low-risk polyp to a malignant neoplasm. We did not include the possibility of regression of polyps. 30 We also did not model malignancies arising from lesions other than polyps, as quantitative estimates of this phenomenon have not been published, and some screening tests may detect nonpolypoid dysplasia. Other limitations were related to incorporating the following untested assumptions: characteristics of test performance would remain constant on repeat testing, incidence of adenoma would be unaffected by screening and compliance with testing was random. The potential impact of these limitations on the results and interpretations is reported in Appendix 1 (available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1). The model did not incorporate the costs of establishing the infrastructure to implement population-based screening for colorectal cancer. The model was developed from the perspective of a third-party payer, such as a provincial ministry of health, the organization that decides on funding for a provincial screening program for colorectal cancer. For this reason, lost productivity costs, which are necessary to determine the societal perspective, were not incorporated.
Although our results reflect a Canadian perspective, the observations and interpretation may be relevant to other jurisdictions with similar health care systems. However, direct comparisons may be limited by differences in costs of the screening tests and of newer chemotherapy agents. For example, in the United States, which has high-quality cost data, the costs of screening tests for colorectal cancer, 20,21 as well as the costs of cancer care, 31 are higher than in Canada. In the present study, the range of the sensitivity analysis did incorporate published US costs of screening tests and chemotherapy (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090845/DC1).
Conclusion
Screening of average-risk individuals for colorectal cancer is a cost-effective measure, even with less-than-perfect compliance. Recognizing that decisions about screening for colorectal cancer depend on local resources and individual patient preferences, either an annual high-sensitivity fecal test, such as a fecal immunochemical test, or colonoscopy every 10 years offer good value for money in Canada.
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: Adrian Levy is a shareholder in Oxford Outcomes Ltd., a consultancy specializing in contract research for a wide range of clients in the life sciences industry, including public sector organizations and pharmaceutical and other private companies. Jennifer Sambrook received consulting fees for model development from Oxford Outcomes Ltd. Denise Zou is employed by Oxford Outcomes, which was hired to work on this project. None declared for Jennifer Telford and Robert Enns.
Contributors: All authors contributed to the study design. Jennifer Telford performed the analyses. Jennifer Telford, Adrian Levy and Robert Enns contributed to the analysis and interpretation of the results and drafted the manuscript. All the authors reviewed the manuscript and approved the final version for publication.
Funding: This study was funded in part by an unrestricted, competitive grant from the Canadian Society of Intestinal Research.
Acknowledgements: The authors thank Dr. Sharlene Gill of the British Columbia Cancer Agency for providing data on chemotherapy costs and Greta Lozano-Ortega of Oxford Outcomes Ltd. for statistical support related to development of the model.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Socioeconomic Disparity Trends in Cancer Screening Among Women After Introduction of National Quality Indicators
- Performance of a quantitative fecal immunochemical test in a colorectal cancer screening pilot program: a prospective cohort study
- Recommendations on screening for colorectal cancer in primary care
- Use of hospital resources in the Finnish colorectal cancer screening programme: a randomised health services study
- Effect of Payment Incentives on Cancer Screening in Ontario Primary Care
- A Randomized Controlled Trial to Improve Colon Cancer Screening in Rural Family Medicine: An Iowa Research Network (IRENE) Study
- Hepatitis B Virus Screening Before Chemotherapy for Lymphoma: A Cost-Effectiveness Analysis
- Long-Term Risk of Colorectal Cancer After Negative Colonoscopy
- Fighting colorectal cancer with information technology
- Mathematical models and cost-effective screening strategies for colorectal cancer
More in this TOC Section
Similar Articles

