


Serological surveillance (serosurveillance) provides estimates of population-level immunity against vaccine-preventable diseases using cross-sectional studies of antibody prevalence. Seroepidemiology is important for evaluating the impact of vaccination programs, as these programs change the immunity of populations, both vaccinated and unvaccinated.1
Seroepidemiology networks test sera from multiple jurisdictions to estimate age- and sex-specific seroprevalences for specific regions. Despite a strong evidence-based immunization policy, Canada does not have a seroepidemiology network to measure the impact of its vaccination programs. Evidence-informed vaccination policy is more important than ever when one considers the rising costs of new vaccines, waning immunity against select vaccine-preventable diseases, increasing numbers of new Canadians who may be susceptible to vaccine-preventable diseases and an aging population whose immune response following vaccination is less predictable.
The monitoring of vaccine-preventable disease in Canada currently consists of surveillance of reportable diseases, adverse events following immunization and immunization coverage. Notifications of reportable disease are important for monitoring trends and detecting outbreaks, but they are known to underestimate incidence and provide little information about the probability of future outbreaks.2 When combined with mathematical modeling, seroepidemiologic data can show the gradual accumulation of susceptible people, changes in the age-specific risk of infection and the potential for outbreaks. This data can be used to evaluate the impact of vaccination programs and inform decisions concerning vaccine policy, including establishing “catch-up” vaccination programs to help mitigate the risk of outbreaks.
National serosurveillance programs are well-established in many countries (Table 1).1,3–15 The European seroepidemiology program coordinates serosurveillance across 18 European countries despite national differences in methods for serum collection, disease epidemiology and immunization schedules. Although the Canadian Health Measures Survey will examine the sero-prevalence of viral hepatitis,16–18 a comprehensive approach to the seroepidemiology of vaccine-preventable diseases does not exist in Canada. This review describes the rationale for establishing a seroepidemiology network in Canada.
Examples of national seroepidemiology programs
Why seroepidemiology is important for Canada
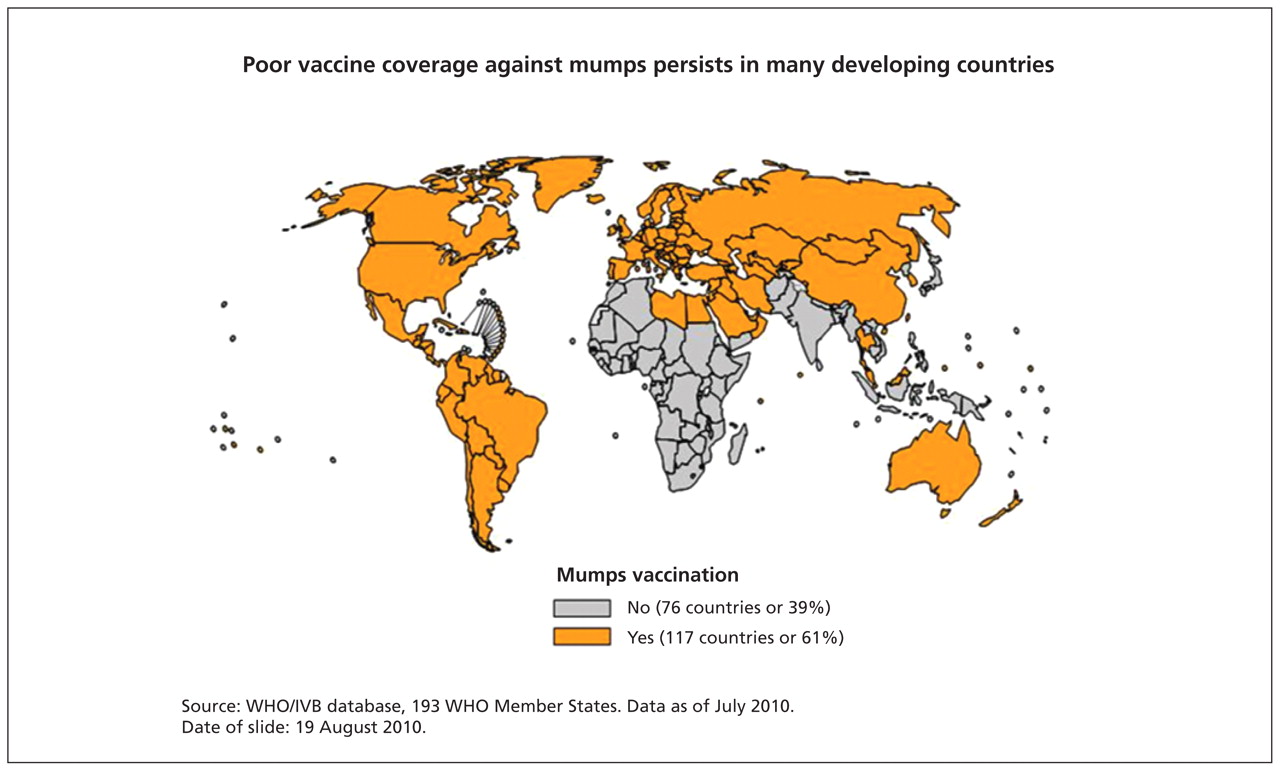
Canada has 13 distinct immunization programs that differ by province/territory, each of which has information systems of variable quality documenting vaccine coverage. In addition, the country’s growing immigrant population challenges our ability to predict future outbreaks of vaccine-preventable disease, since current national data on immunization coverage are survey-based with small sample sizes and focus largely on childhood immunization. Since 2000, 50% of the more than 250 000 newcomers who enter Canada each year come from regions that have no vaccine program for rubella or mumps (Figures 1 and 2).19–23 A sero-prevalence study involving adult immigrants and refugees in Montréal, Quebec, found that 36% were nonimmune to at least one of measles, mumps or rubella (MMR).21 Aboriginal populations in Canada are another important group for whom susceptibility to vaccine-preventable diseases may differ from that of the general population,24,25 and for whom immunization coverage is challenging to ascertain.

Countries using rubella vaccine in their national immunization schedules in 1996 and in 2008.22 From: www.who.int/immunization_monitoring/diseases/rubella_map_age.jpg (accessed 2011 Aug. 26). Reprinted with the permission of the World Health Organization.

Countries using mumps vaccine in their national immunization schedules in 2009.23 From: www.who.int/immunization_monitoring/diseases/mumps_map_schedule.jpg (accessed 2011 Aug. 26). Reprinted with the permission of the World Health Organization.
Applying seroepidemiology data
Estimating the burden of vaccine-preventable disease
Understanding the burden of disease is critical in evaluating whether vaccines should be included in immunization programs.26 Seroepidemiologic data can help clarify trends in the burden of vaccine-preventable diseases where notifications may be incomplete or nonrepresentative. Investigators from the Netherlands found that serologic evidence of recent pertussis in people 9 years of age and older more than doubled over a 10-year period. This was consistent with data on notifications and admissions to hospital, suggesting that the increase in pertussis cannot be fully explained by improvements in diagnostics and reporting.27 Conversely, Australian investigators found serologic evidence of recent pertussis increased among adults between 1997–98 and 2002, despite a relatively low and stable rate of notification for the disease (Figure 3).28 Such evidence suggests that the burden of disease in this age group was underestimated.
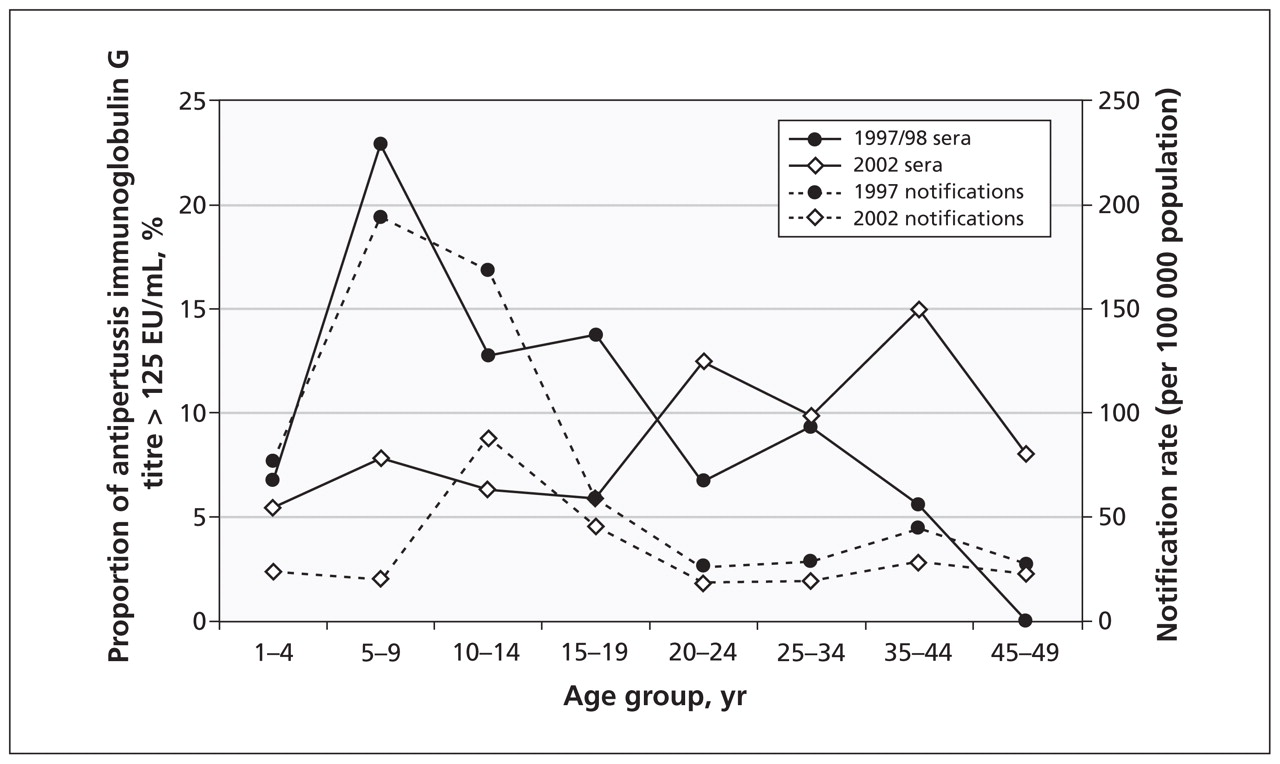
Age-specific trends in pertussis infection in Australia using both reportable disease notifications and population-based serosurveillance. From: Quinn HE, McIntyre PB, Backhouse JL, Gidding HF, Brotherton J, Gilbert GL. The utility of seroepidemiology for tracking trends in pertussis infection. Epidemiol Infect. 2010 Mar;138(3):426–33.28 Reprinted with the permission of Cambridge University Press.
Understanding emerging infections
Knowledge of age-specific immunity to emerging infections is important for modeling the future burden of disease, formulating vaccine policy and planning for health care resources. Seroprevalence studies done during the H1N1 influenza pandemic were important for identifying risk factors for infection, anticipating the size of the second wave, estimating the final burden of disease and modeling the effectiveness of public health interventions, such as school closures and vaccination.29–31
Identifying at-risk groups
Immigrants and refugees settling in Canada comprise a group at risk for certain vaccine-preventable diseases. Seroprevalence studies done in populations of immigrants and refugees in Montréal, Que.,21 in Boston, Massachusetts,32 and in the United Kingdom33 have found substantial susceptibility to MMR and varicella consistent with both the variability in global vaccine recommendations and uptake and the epidemiology of natural infection outside of North America and western Europe. Outbreaks of rubella within migrant populations from Latin America have occurred in the United States and parts of Europe.34–36 Since 1996, new immigrants to the United States are required to have their vaccinations updated as part of the mandatory medical screening prearrival. No such policy exists in Canada. The Public Health Agency of Canada recommends that health care providers who see immigrants assess and update immunizations and screen for chronic conditions that would alter vaccine recommendations;37 however, because of delays in health care coverage, difficulty in locating providers of primary care and competing priorities at the time of resettlement, these recommendations are often challenging to implement, and many new Canadians remain susceptible to some vaccine-preventable diseases.
Seroepidemiologic studies have also shown an increased burden of some vaccine-preventable diseases in Aboriginal communities.38–40 However, studies of this population have tended to use sera from specific communities37 or convenience samples,39,40 with questionable generalizability to the diverse communities of First Nations, Métis and Inuit people. Ensuring the inclusion of both immigrants and Aboriginal people in a future sero-epidemiology program in Canada is both vitally important and challenging.
Other groups at risk are communities with low vaccination coverage due to vaccine refusal, such as communities that reject immunization based on religious beliefs or for philosophical reasons.41–43 There have been outbreaks of vaccine-preventable diseases among underimmunized religious groups.44–48
Evaluating vaccines
After the introduction of new vaccines, seroepidemiology is an important adjunct to other methods of surveillance to monitor their long-term impact and duration of immunity, and to identify whether adjustments to vaccine policy are required.
Establishing serosurveillance programs has been instrumental to the successful control of measles in many countries where age-specific data on susceptibility to the disease has influenced vaccine policy. In the UK, the combination of seroepidemiologic data and mathematical modeling predicted the potential for a measles epidemic to occur by the mid-1990s.49,50 This led to a national campaign in which 92% of children between the ages of 5 and 16 years were vaccinated.9 Subsequent serosurveys suggested that the campaign was a success, but they also showed high susceptibility among preschool-aged children. This informed the introduction of a second dose of MMR vaccine in the routine vaccination schedule at four years of age.9 Similarly, in Australia, seroprevalence data identified young adults as having low levels of immunity to measles, and a targeted campaign of MMR vaccination began in 2001.51,52
Serosurveillance has also been used to identify risks posed by emerging vaccine-preventable diseases in neighbouring regions. In response to a large outbreak of diphtheria in eastern Europe, a serosurvey of nearby countries found substantial proportions of adults with antitoxin titres below the putative protective threshold. This evidence suggested that few adults had been vaccinated despite changes to the vaccine policy that were implemented in response to the outbreak.53 High levels of protection among children and the limited infectiousness of diphtheria are thought to have protected these countries despite suboptimal protection among adults.53
Modeling and health economic evaluations
Seroepidemiologic data can be entered into mathematical models that can then be used to determine the potential for sustained outbreaks by calculating the effective reproductive number (Re) for specific regions and/or age groups. This method has been used to predict the risk of future measles epidemics in both the UK and Australia, and it can also be used to estimate the cost-effectiveness of vaccination programs and to predict their indirect consequences, such as increased age at infection and any attendant risks.
Epidemiologic considerations for seroepidemiology programs
There are two general approaches to serum sampling: convenience and population-based random sampling (Table 1). Most countries use “residual” sera submitted for diagnostic testing that would otherwise have been discarded (i.e., convenience sampling). Less commonly, countries collect sera from people randomly selected from a population-based sample. The advantages of population-based random sampling include the opportunity to obtain informed consent, to over-sample specific groups and to obtain information at the level of the individual, including a person’s history of vaccination. These advantages must be balanced against increased cost and the time required for population-based surveys.
Both methods present the risk of selection bias. For example, data from the Netherlands that used population-based random sampling found that the sole predictor of nonparticipation was individual perception of vaccines to be “unnecessary.”54 Given that people with these beliefs are less likely to be vaccinated, seroepidemiologic programs using population-based sampling may overestimate population-level immunity to vaccine-preventable diseases. In contrast, use of residual sera may result in a bias toward populations with a higher number of medical comorbidities or different risk and health-seeking behaviours. Sera collected for occupational or prenatal screening could introduce healthy-person biases. The only published study comparing the two sampling approaches yielded similar estimates of immunity against five vaccine-preventable diseases at about a sevenfold increased cost for population-based sampling.55
Challenges to implementation
Developing a seroepidemiology network in Canada is ambitious and poses a number of challenges related to funding, ethics and epidemiologic and laboratory considerations. Detractors may cite these challenges as barriers to the implementation of a Canadian network; they may also argue that funding should be prioritized for new vaccine programs or for establishing other surveillance activities, such as a pan-Canadian immunization registry. However, these challenges are not insurmountable, and there will always be competing priorities for scarce resources. Establishing a seroepidemiology network would provide a strong evidence-informed foundation from which to successfully advocate for improvements in vaccine policy and methods of surveillance.
Funding and the longer-term stewardship of such a network is key to its successful implementation. Most seroepidemiologic studies in Canada have been supported by time-limited research funds.29,38,39,56,57 These studies show the epidemiologic and laboratory capacity to complete such work in Canada. Preliminary establishment of a network is likely to be started on a smaller scale in a limited number of participating provinces and territories, supported by research funds. However, in many jurisdictions, the seroepidemiology network is viewed as a core surveillance activity, as opposed to research, and receives dedicated government funding. The introduction of the Canadian Health Measures Survey, including plans for future surveys, affords the potential for using this federally funded initiative for the implementation of a Canadian seroepidemiology network.
If a de novo Canadian network were established, a number of practical and epidemiologic challenges would remain. The roles and responsibilities of provincial and federal stakeholders would require clarification. The selection of participating jurisdictions would ideally need to ensure representativeness of the Canadian population, including urban–rural composition, immigration trends and Aboriginal groups. Oversampling of specific at-risk groups may be required for accurate estimates of susceptibility to vaccine-preventable diseases, but this will likely require linkage to other sources of data, which may be viewed as a privacy issue in some quarters.
The collection of residual sera for analysis is the most pragmatic and least costly option for implementing a seroepidemiology network. However, this method raises important ethical and privacy issues that will need to be addressed, such as whether samples can be used without consent or notification, how anonymity can be ensured and whether record linking might be used. Precedence does exist — anonymized residual sera and record linking have been used in Canada without consent to assess the sero-prevalence of HIV.58–61
Laboratory issues must also be addressed. Although provincial public health laboratories are the most appropriate facilities to coordinate testing, the extent to which their residual sera are representative of their province’s general population may differ. Inclusion of hospital and commercial laboratories may be necessary. A second critical issue is that of standardization across laboratories and across manufacturers’ assays. Immune correlates of protection do not exist for all vaccines, and cell-mediated immunity may be more important than humoral in some instances. In addition, the lack of sensitivity of some commercially available assays and limited access to commercially protected test methods makes assessing immunity to certain antigens challenging. A seroepidemiology network will also require capacity for long-term cryogenic storage at participating laboratories and supporting infrastructure that includes systems for inventory and the management and analysis of data. These challenges are not insurmountable, and there is a wealth of international experience in the establishment of national and international seroepidemiology networks from which Canada will benefit.
Conclusion
Canada is uniquely positioned to benefit from the establishment of a seroepidemiology network, with its strong evidence-based immunization policy, its range of immunization schedules, the diverse and growing proportion of new Canadians and strong supporting systems for the surveillance of vaccine-preventable diseases. The revision of the National Immunization Strategy currently underway may provide an opportunity to contribute to the establishment of a crucial, and currently missing, component of Canada’s infrastructure for the surveillance of vaccine-preventable diseases.
Key pointsDespite strong supporting systems for the surveillance of vaccine-preventable diseases, Canada does not have a comprehensive approach to seroepidemiology.
Serosurveillance provides estimates of population-level immunity against vaccine-preventable diseases using cross-sectional studies of antibody prevalence.
The potential applications of seroepidemiologic data include estimating the burden of specific vaccine-preventable diseases, predicting potential outbreaks, identifying groups at risk and evaluating the impact of vaccination programs.
Owing to Canada’s range of immunization schedules, its diverse and growing population of new Canadians and its history of evidence-based immunization policy, the country would benefit from a seroepidemiology network.
Acknowledgement
The authors thank the participants of a meeting funded by the Canadian Institutes of Health Research convened to discuss Canadian research priorities in the field of seroepidemiology (Oct. 13–14 2011).
Footnotes
Competing interests: The authors received funding from the Canadian Institutes of Health Research to host a meeting to discuss the establishment of a seroepidemiology network. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Natasha Crowcroft developed the concept for the article. Sarah Wilson drafted the article. All of the authors critically revised the manuscript for important intellectual content and approved the final version submitted for publication.
Note: The opinions expressed in this paper are those of the authors and do not necessarily represent the position of the Public Health Agency of Canada.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Feasibility and acceptability of collecting dried blood spots (DBS) from children after vaccination during Supplementary Immunization Activities to estimate measles and rubella seroprevalence
- Wastewater as a back door to serology?
- Seroepidemiology of COVID-19 in pregnant women and their infants in Uganda and Malawi across multiple waves 2020-2022
- Multiyear prospective cohort study to evaluate the risk potential of MERS-CoV infection among Malaysian Hajj pilgrims (MERCURIAL): a study protocol
- Calibration and Evaluation of Quantitative Antibody Titers for Measles Virus by Using the BioPlex 2200
More in this TOC Section
Similar Articles
Collections

