


- © 2008 Canadian Medical Association
Abstract
Background: Whether to continue oral anticoagulant therapy beyond 6 months after an “unprovoked” venous thromboembolism is controversial. We sought to determine clinical predictors to identify patients who are at low risk of recurrent venous thromboembolism who could safely discontinue oral anticoagulants.
Methods: In a multicentre prospective cohort study, 646 participants with a first, unprovoked major venous thromboembolism were enrolled over a 4-year period. Of these, 600 participants completed a mean 18-month follow-up in September 2006. We collected data for 69 potential predictors of recurrent venous thromboembolism while patients were taking oral anticoagulation therapy (5–7 months after initiation). During follow-up after discontinuing oral anticoagulation therapy, all episodes of suspected recurrent venous thromboembolism were independently adjudicated. We performed a multivariable analysis of predictor variables (p < 0.10) with high interobserver reliability to derive a clinical decision rule.
Results: We identified 91 confirmed episodes of recurrent venous thromboembolism during follow-up after discontinuing oral anticoagulation therapy (annual risk 9.3%, 95% CI 7.7%–11.3%). Men had a 13.7% (95% CI 10.8%–17.0%) annual risk. There was no combination of clinical predictors that satisfied our criteria for identifying a low-risk subgroup of men. Fifty-two percent of women had 0 or 1 of the following characteristics: hyperpigmentation, edema or redness of either leg; D-dimer ≥ 250 μg/L while taking warfarin; body mass index ≥ 30 kg/m2; or age ≥ 65 years. These women had an annual risk of 1.6% (95% CI 0.3%–4.6%). Women who had 2 or more of these findings had an annual risk of 14.1% (95% CI 10.9%–17.3%).
Interpretation: Women with 0 or 1 risk factor may safely discontinue oral anticoagulant therapy after 6 months of therapy following a first unprovoked venous thromboembolism. This criterion does not apply to men. (http://Clinicaltrials.gov trial register number NCT00261014)
Venous thromboembolism is a common, potentially fatal, yet treatable, condition. The risk of a recurrent venous thromboembolic event after 3–6 months of oral anticoagulant therapy varies. Some groups of patients (e.g., those who had a venous thromboembolism after surgery) have a very low annual risk of recurrence (< 1%),1 and they can safely discontinue anticoagulant therapy.2 However, among patients with an unprovoked thromboembolism who discontine anticoagulation therapy after 3–6 months, the risk of a recurrence in the first year is 5%–27%.3–6 In the second year, the risk is estimated to be 5%,3 and it is estimated to be 2%–3.8% for each subsequent year.5,7 The case-fatality rate for recurrent venous thromboembolism is between 5% and 13%.8,9 Oral anticoagulation therapy is very effective for reducing the risk of recurrence during therapy (> 90% relative risk [RR] reduction);3,4,10,11 however, this benefit is lost after therapy is discontinued.3,10,11 The risk of major bleeding with ongoing oral anticoagulation therapy among venous thromboembolism patients is 0.9–3.0% per year,3,4,6,12 with an estimated case-fatality rate of 13%.13
Given that the long-term risk of fatal hemorrhage appears to balance the risk of fatal recurrent pulmonary embolism among patients with an unprovoked venous thromboembolism, clinicians are unsure if continuing oral anticoagulation therapy beyond 6 months is necessary.2,14 Identifying subgroups of patients with an annual risk of less than 3% will help clinicians decide which patients can safely discontinue anticoagulant therapy.
We sought to determine the clinical predictors or combinations of predictors that identify patients with an annual risk of venous thromboembolism of less than 3% after taking an oral anticoagulant for 5–7 months after a first unprovoked event.
Materials and methods
Study design and selection of participants
We performed a prospective clinical decision-rule derivation cohort study and a split-sample validation study that included consecutive unselected patients from 12 tertiary care centres in 4 countries. We included patients whose first, objectively proven unprovoked thromboembolism (proximal deep vein thrombosis, or segmental or greater pulmonary embolism) occurred 5–7 months before enrollment. We included patients who received heparin or low-molecular-weight heparin for 5 or more days and who received oral anticoagulation therapy for 5–7 months after the event (target international normalized ratio 2–3). We also included patients if they had not had a recurrent venous thromboembolism during the treatment period. Objective documentation of deep vein thrombosis required the presence of a noncompressible segment on a compression ultrasound of the popliteal vein or a more proximal leg vein. Objective documentation of a pulmonary embolism required a high-probability ventilation–perfusion scan or a segmental or larger artery filling defect on a spiral computed tomography (CT) scan. We defined an unprovoked index venous thromboembolism as one that occurred in the absence of a leg fracture or lower-extremity plaster cast, immobilization for greater than 3 days or surgery using a general anesthetic in the 3 months before the index event, and without the diagnosis of a malignant disease in the past 5 years.
We excluded patients who were unable or unwilling to provide written informed consent, were aged 17 years or younger, had already discontinued oral anticoagulants, required ongoing anticoagulation for reasons other than venous thromboembolism, were geographically inaccessible for follow-up, were being treated for a recurrent unprovoked venous thromboembolism or “known” high-risk thrombophilia (defined as known deficiency of protein S, protein C or antithrombin, known persistently positive anticardiolipin antibodies [> 30 U/mL], a known persistently positive lupus anticoagulant, or who had 2 or more known thrombophilic defects [e.g., homozygous for factor V Leiden or prothrombin gene mutation, or compound heterozygous for factor V Leiden and prothrombin gene mutation]). We did not perform thrombophilia testing before enrollment; however, we excluded patients with high-risk thrombophilia if it had been independently identified before enrollment.
We obtained approval from the institutional research ethics board at all participating centres (Ottawa Hospital Research Ethics Board for the lead institution).
Baseline patient assessment
We performed an assessment 5–7 months after the index venous thromboembolism event while patients were receiving oral anticoagulant therapy. We collected data for 69 independent variables identified in a systematic review conducted a priori and periodically updated throughout the study (Appendix 1, available online at www.cmaj.ca/cgi/content/full/179/5/417/DC2). We collected data about demographic characteristics, risk factors for venous thromboembolism at the time of index event, patient-reported post-thrombotic symptoms, concomitant medications, results of thrombophilia testing, and imaging reports confirming the index venous thromboembolism event. In addition, study nurses performed a physical examination of each patient, recording height and weight. Nurses also performed a standardized evaluation of post-thrombotic signs for both legs.
We obtained samples for laboratory analysis while patients were taking oral anticoagulants. A complete blood count was performed and homocysteine levels were analyzed at local clinical laboratories. Standard protocols were used to extract DNA from peripheral blood leukocytes, and an ABI PRISM 3100 genetic analyzer (Applied Biosystems) was used to test for factor V Leiden and to perform prothrombin gene variant genotyping by use of established methods.15 We also obtained samples to test for the levels of factor VIII, D-dimer, lupus anticoagulant and anticardiolipin IgG and IgM. These samples were processed and stored locally, but they were shipped on dry ice and analyzed centrally at the London Health Sciences Centre. Within 1 hour of collection, plasma samples were double centrifuged at 2500g for 20 minutes and frozen immediately at –70°C. D-Dimer testing was performed using the Vidas D-dimer reagent on the Vidas Instrument (bioMérieux). Coagulation assays were performed on an ACL 9000 instrument (Instrumentation Laboratory). We used the HemosIL APTT-SP reagent to test for factor VIII, and we tested for lupus anticoagulant using dilute Russel viper venom time (HemosIL LAC screen) with LAC Confirm reagents (Instrumentation Laboratory). Anticardiolipin antibodies (IgG and IgM) were tested for using commercially available enzyme-linked immunosorbent assay kits (Louisville APL Diagnostics).
We performed baseline imaging using compression ultrasonography of the leg that was symptomatic at the time of the index event. If the patient had signs or symptoms of a pulmonary embolism at the time of index event, a ventilation-perfusion scan was also performed.
Follow-up and outcome assessment
Patients were instructed to contact study personnel if they developed symptoms of recurrent venous thromboembolism. Patients were seen in clinic every 6 months and were asked about whether they had any symptoms of venous thromboembolism. Participants were withdrawn and their data censored if they withdrew consent or started anticoagulant therapy (reasons for starting anticoagulants were documented).
All suspected venous thromboembolism events and deaths were independently adjudicated by physicians (M.R., S.K., P.W., D.A., M.K., G.L.) who were blinded to the predictor data. All patients with a suspected recurrent venous thromboembolism who presented with leg symptoms underwent compression leg vein ultrasonography or venography. The criteria for diagnosis of recurrent deep vein thrombosis have been previously described.16 All patients with a suspected pulmonary embolism had a ventilation–perfusion scan. If results of the scan were normal, unchanged or better than those from the baseline exam, we excluded the diagnosis of pulmonary embolism. If the ventilation–perfusion scan showed a new mismatched segmental defect or a greater perfusion defect compared with baseline, a pulmonary embolism was diagnosed. If a new matched or subsegmental perfusion defect was found, we performed a spiral CT scan. If this scan showed an intraluminal filling defect in a segmental or larger artery in an area that had normal perfusion in the baseline ventilation–perfusion scan, a pulmonary embolism was diagnosed. All other patients were required to undergo pulmonary angiography to diagnose or exclude suspected recurrent pulmonary embolism. We also considered pulmonary embolism found at autopsy to be diagnostic of recurrent venous thromboembolism.
Data analysis
We first performed univariable analyses to determine the strength of association between each potential predictor variable and recurrence of venous thromboembolism. All potentially significant (p < 0.20) continuous variables were dichotomized at varying cut-off points, and the optimal cut-off points were identified (i.e., the cut-off points with the highest χ2 value). We used dichotomous variables to make the final clinical decision rule easier to remember and apply. We then assessed the dichotomized variables with p < 0.10 for interobserver reliability. Variables with previously published high reproducibility were retained. For those without published evidence of reproducibility, we conducted interobserver reliability studies. We retained variables with a kappa score greater than 0.6. This process aided in the selection of the best variables for the multivariable analysis.
Using conditional logistic regression with forward variable selection, we conducted multivariable analysis with recurrent venous thromboembolism as the dependent variable. The study steering committee (M.R., M.K., P.W., G.L., A.P., R.W., S.K., D.A.) derived and reviewed 5 candidate clinical decision rules for women and 2 for men. These rules were selected based on classification performance (annual risk of recurrence in the low-risk group, defined a priori as a target of < 3%), proportion of patients identified as low risk, face validity, ease of use and fewest predictor variables. We performed split-sample cross-validation by determining the classification performance of a short list of candidate clinical decision rules for 500 subsamples. Each subsample consisted of randomly chosen patients from the study population. The size of each subsample was 50% of the study population. We rejected any decision rule for which any of the 500 samples had a greater than 3% annual risk of recurrence. We further internally assessed the performance of the final clinical decision rules using the subset of patients whose data could not be included in the derivation of the rule because of missing data.
Funding and commercial interests
This study was funded by the Canadian Institutes of Health Research (grant no. MOP 64319) and bioMérieux. bioMérieux provided funding via an unrestricted research grant. The company did not influence the design, conduct or reporting of the trial.
Results
Between October 2001 and March 2006, we enrolled 665 participants. Of these, 600 patients completed follow-up in September 2006 (Figure 1). The mean age of participants was 53 (min–max 18–95) years, and 49% were female (Table 1). Index events included 194 (30%) isolated pulmonary embolisms, 339 (52.5%) isolated deep vein thrombosis events and 113 (17.5%) events of both deep vein thrombosis and pulmonary embolism. During a mean follow-up interval of 18 (min–max 1–47) months, 91 of 306 suspected recurrent venous thromboembolism were objectively documented, which is equal to a 9.3% annual risk of recurrent venous thromboembolism (95% CI 7.7%–11.3%). None of the deaths during follow-up were caused by recurrent venous thromboembolism (case-fatality rate 0%, 95% CI 0%–3.2%).
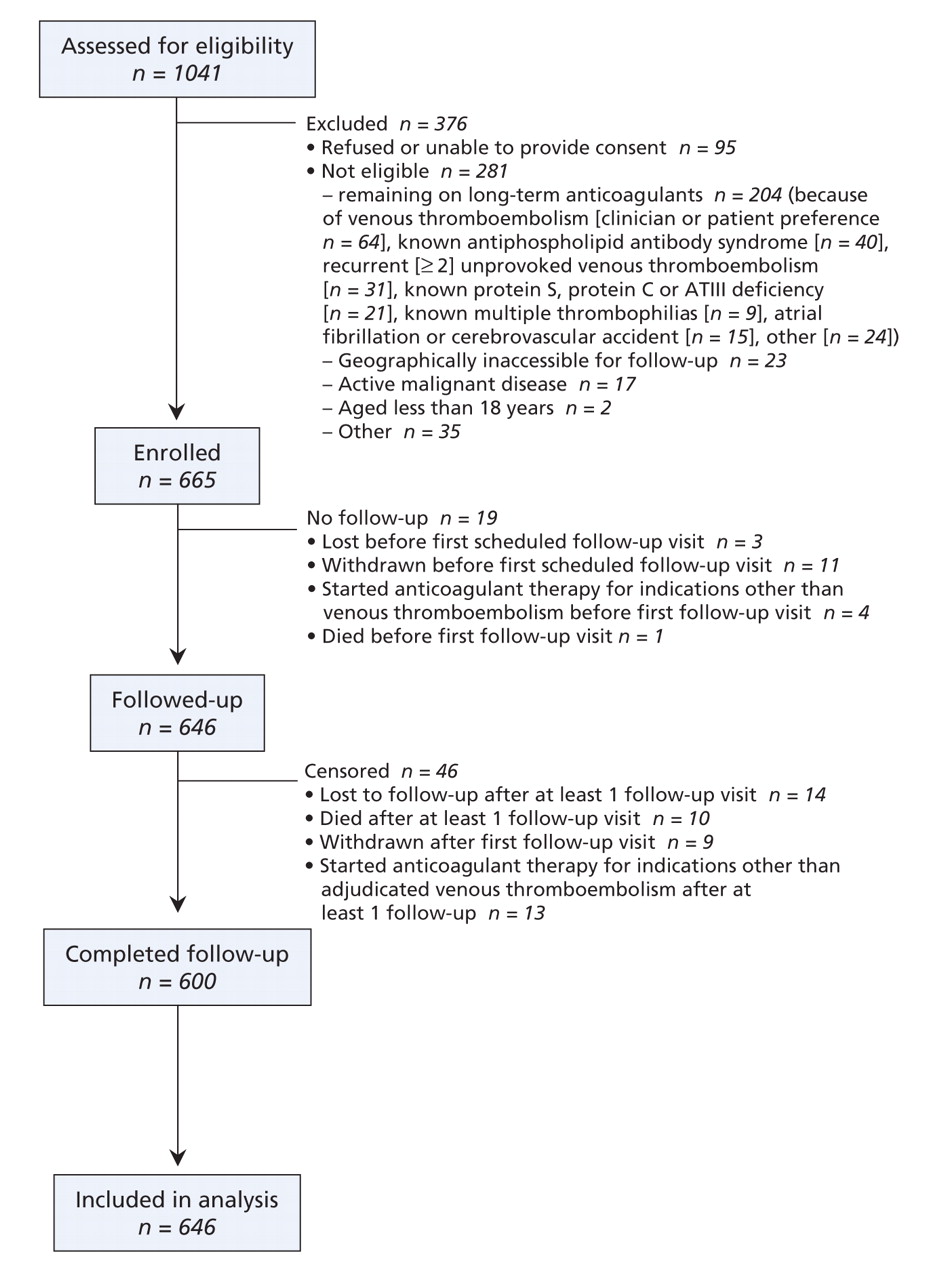
Figure 1: Flow of participants through the study.
Table 1.
Table 1 lists potential predictor variables for the study population. Of men, 19% developed recurrent venous thromboembolism over a mean follow-up of 72 weeks (annual risk 13.7%, 95% CI 10.8%–17.0%) compared with 8.9% of women during a mean follow-up of 84 weeks (5.5% annual risk, 95% CI 3.7%–7.8%) (p < 0.001). Men with post-thrombotic symptoms of leg hyperpigmentation, edema or redness had very high risk of recurrence (24.0% annual risk) (Figure 2).

Figure 2: Potential predictor variables for men at optimal cutoff points, by strength of association. *Determined by χ2 testing, unless stated otherwise. †Presence of antiphospholipid (APL) antibodies was determined by anticardiolipin antibody (IgG or IgM) ≥ 6 U/mL or by a positive result for lupus anticoagulant. ‡Determined by the Fisher exact test. Note: BMI = body mass index, CI = confidence interval, HER = hyperpigmentation, edema or redness, RR = relative risk, VTE = venous thromboembolism.
Initial multivariable modelling failed to identify a clinical decision rule that satisfied our criterion (< 3% annual risk) for identifying a low-risk subgroup of men. Thus, we performed a post-hoc stratification of participants by sex, and we repeated the univariable analyses, including identifying optimal cut-off points for each sex strata (Figure 2 and Figure 3). The use of multivariable modelling with sex-specific subgroups led to 5 candidate decision rules for women (Table 2) and 2 for men (Table 3). We performed split sample cross-validation with the candidate clinical decision rules that had good classification performance, face validity and ease of use. Neither of the candidate clinical decision rules for men had face validity, nor were they statistically validated in the 500 subsample analysis (mean risk > 3%).

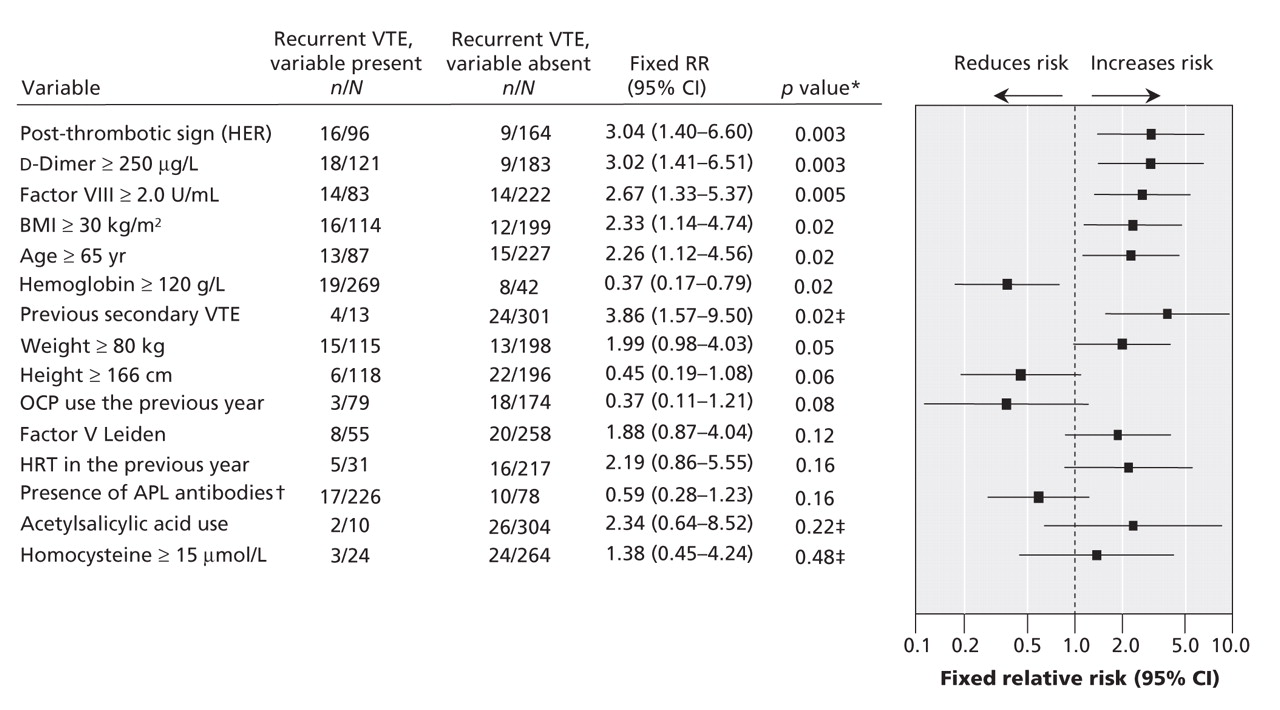
Figure 3: Potential predictor variables for women at optimal cut-off points, by strength of association. *Determined by χ2 testing, unless stated otherwise. †Presence of antiphospholipid (APL) antibodies was determined by anticardiolipin antibody (IgG or IgM) ≥ 4 U/mL or by a positive result for lupus anticoagulant. ‡Determined by the Fisher exact test. Note: BMI = body mass index, CI = confidence interval, HER = hyperpigmentation, edema or redness, HRT = hormone replacement therapy, OCP = oral contraceptive pills, RR = relative risk, VTE = venous thromboembolism.
Table 2.
Table 3.
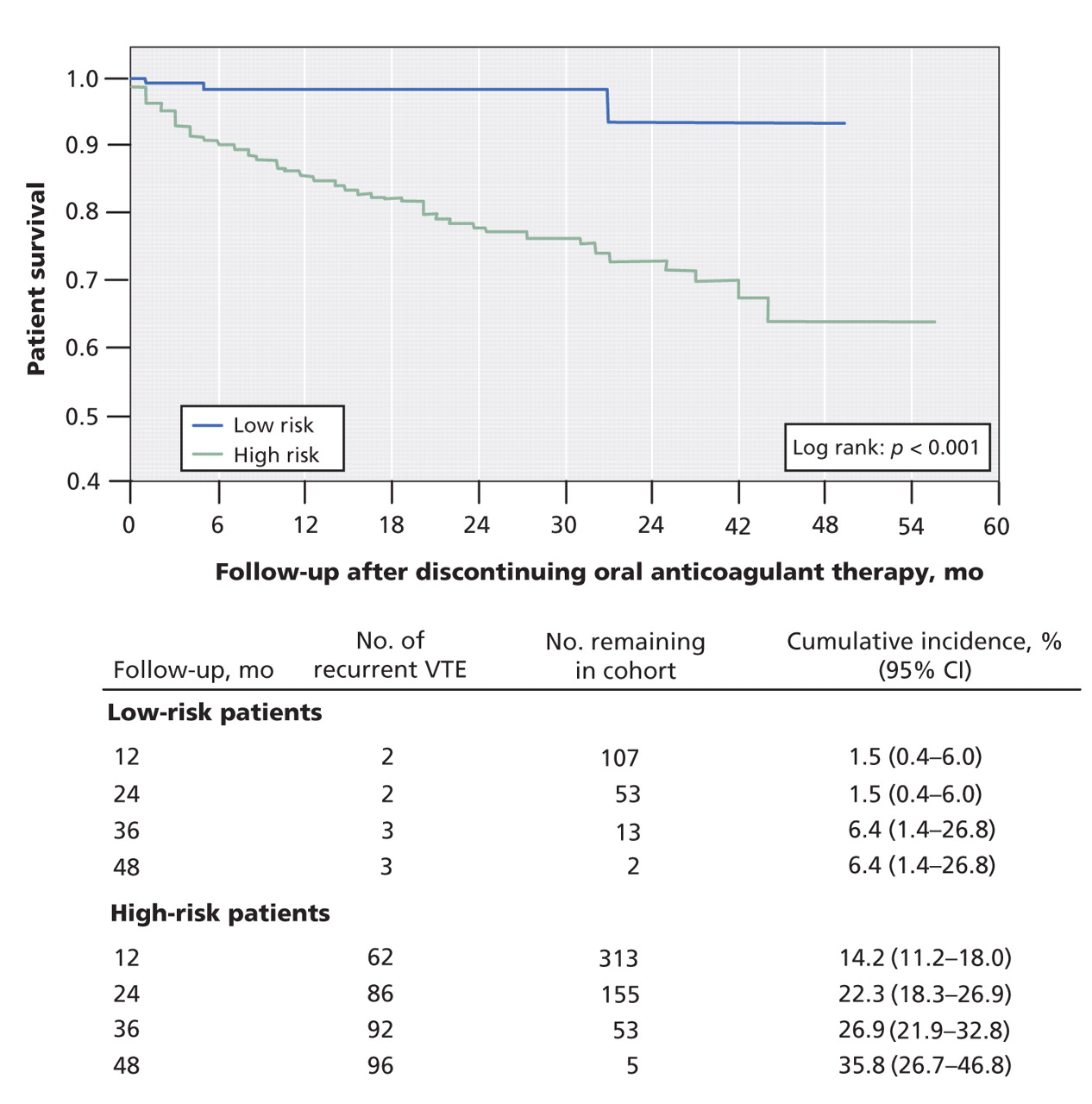
In total, 52% of women had 0 or 1 risk factors for recurrent venous thromboembolism (hyperpigmentation, edema or redness of either leg; D-dimer ≥ 250 μg/L while on warfarin; BMI ≥ 30 kg/m2; age ≥ 65 years). Among these women, the annual risk of venous thromboembolism was 1.6% (95% CI 0.3%–4.6%). Women with 2 or more risk factors had an annual risk of 14.1% (95% CI 10.9%–17.3%). Of low-risk patients, the annual risk was 1.2% in the subgroup with index deep vein thrombosis alone, 0% in the group with index pulmonary embolism alone, 2.1% in the group with index pulmonary embolism with or without deep vein thrombosis, and 2.5% in the group with index deep vein thrombosis with or without pulmonary embolism. The survival curve for women at low risk and for those at high risk (men, and women with ≥ 2 risk factors) are shown in Figure 4. For the 500 subsamples from the derivation set, the mean annual risk of recurrent venous thromboembolism in women at low risk of recurrence was between 0% and 3.0%.

Figure 4: Survival estimates and cumulative risk of recurrent venous thromboembolism (VTE) after discontinuing oral anticoagulant therapy after 5–7 months. Patients were classified as low or high risk according to the candidate diagnostic rules for men and women. We performed the survival analysis with updated data in June 2007 (mean follow-up 22.5 months). Note: CI = confidence interval.
In total, 124 participants in the derivation set were missing predictor data. Of these, 101 were classifiable as low or high risk of recurrence and were included in the internal validation. In this cohort, women in the low-risk group (≤ 1 risk factor) had an annual risk of recurrent venous thromboembolism less than 3% (annual risk 2.7%, 95% CI 0.3%–8.9%). Women with 2 or more risk factors had an annual risk of recurrence of 10.2% (95% CI 6.2%–15.1%).
Interpretation
We developed and internally validated a clinical decision rule that may ultimately provide clinicians with guidance as to whether oral anticoagulation therapy can be discontinued after 5–7 months of treatment for an “unprovoked” venous thromboembolism. This clinical decision rule identifies women with an annual risk of venous thromboembolism less than 3% who can likely safely discontinue anticoagulant therapy (Box 1).

Despite research about the duration of anticoagulant treatment for unprovoked venous thromboembolism3,4,11,17,18 and the identification of risk factors for its recurrence,19–26 clinicians remain vexed as to who should continue taking anticoagulants after an initial 3–6 months of therapy. In fact, practice guidelines have remained unchanged despite a decade of research.2 This failure to change practice is likely because a therapy has not been identified that reduces the risk of bleeding below the level of risk of recurrent venous thromboembolism after 3–6 months of anticoagulant therapy (e.g., lower intensity international normalized ratio, new anticoagulants). This failure is also likely because of a failure to identify high-risk groups in which the benefits of standard therapies clearly outweighed the risks and to identify low-risk groups for whom no further therapy is necessary.
A number of variables to stratify risk of recurrent venous thromboembolism in patients with an unprovoked index event have been investigated, including sex,22 plasma D-dimer levels measured 1–2 months after discontinuation of oral anticoagulants,19,20,23,24 residual venous obstruction using venous ultrasonography19,25,26 and elevated plasma levels of factor VIII.21 Studies investigating these variables have all been hampered by the inclusion of patients with heterogeneous risk of recurrence (e.g., a variable duration of oral anticoagulation therapy,19–21,23,24 both provoked and unprovoked index events,19,20,23 both distal and proximal deep vein thrombosis23). Only the use of D-dimer levels as a predictor variable has been studied in a prospective management study.24 In this study, a normal D-dimer value after stopping oral anticoagulants was not sufficient to identify patients at low risk (i.e., < 3% annual risk) to be clinically useful.24 Furthermore, stopping anticoagulants, testing D-dimer levels 1 month later and restarting anticoagulant therapy if necessary, is impractical for the majority of patients and exposes high-risk patients to a long period without anticoagulants. We did not find that residual venous obstruction (detected by leg vein imaging) was an important predictor of recurrent venous thromboembolism. We found that elevated levels of factor VIII was a significant univariable predictor, but it was not an independent predictor in the multivariable analysis. In our study, no single predictor identified a sufficiently low-risk group to be clinically useful. A multivariable clinical decision rule is a more powerful approach because it combines the predictive power of multiple independent variables.
We identified 3 major novel findings. First, post-thrombotic findings after 5–7 months of oral anticoagulant therapy are the strongest predictors of recurrent venous thromboembolism. Second, for women, but not for men, D-dimer levels (measured while taking oral anticoagulants) are an important predictor of recurrence after the patient has stopped taking anticoagulants. Third, we have identified a clinical decision rule that can be used to identify women at low risk of recurrence.
Our study has a number of strengths. To date, this is the largest and most comprehensive clinical study that has evaluated risk factors for recurrent venous thromboembolism in patients with unprovoked proximal deep vein thrombosis or pulmonary embolism. We prospectively measured all important risk factors potentially associated with recurrent venous thromboembolism in a standardized fashion. Our study included patients for whom the clinical decision to discontinue oral anticoagulation therapy is most uncertain, and we analyzed risk factors at the time when a decision is usually made. In addition, our study included a representative sample of patients from multiple centres and countries. These patients were consecutively enrolled without bias. The clinically relevant primary outcome of recurrent venous thromboembolism was clearly defined and independently adjudicated. We included only reproducible clinical variables in the final decision rule (age, BMI,27 D-dimer,28 post-thrombotic symptoms findings of hyperpigmentation, edema and redness29), which likely enhances the interobserver reproducibility of the rule. In addition, the 4 variables included in our decision rule all have face validity (i.e., make sense to clinicians) as predictors of recurrent venous thromboembolism. D-dimer levels, older age and increased BMI have been consistently shown to be predictors of recurrent venous thromboembolism.19,20,22–24,30 Venous stasis changes of hyperpigmentation, edema or redness have been previously suggested to be predictors of recurrent venous thromboembolism.31,32 Because venous damage predisposes patients to slower and abnormal blood flow, the risk of recurrent venous thromboembolism should be increased among these patients.
Our study has several limitations. First, to avoid over-fitting, not all potentially significant variables (p < 0.20) were included in our multivariable modelling. Second, not all patient data sets in the derivation group were complete. Third, D-dimer levels were measured and the optimal cut-off point (D-dimer ≥ 250 μg/L) was identified by use of 1 reagent on 1 instrument. The use of other D-dimer tests will require separate studies to identify optimal cut-off points and performance in predicting recurrent venous thromboembolism within the context of this clinical decision rule. Fourth, our clinical decision rule does not predict how long anticoagulants should be continued for patients in the high-risk group. Randomized controlled trials that compare therapeutic options (shorter v. longer duration, higher v. lower intensity therapy, alternative anticoagulants) or risk stratification at a later time may be required to define optimal therapeutic management for high-risk patients. Fifth, we excluded patients with known high-risk thrombophilia, and few of our patients were nonwhite (< 8%), hence our clinical decision rule may not apply to patients in these groups. Finally, and most importantly, additional important methodologic criteria33,34 must be met before our decision rule can be widely adopted: the interobserver agreement of the rule must be determined, and the safety of this rule must be prospectively validated in a separate population to ensure that the low-risk group has less than 3% annual risk of recurrence.
We were unable to derive a rule that identified men at low risk who can safely discontinue anticoagulants after 5–7 months of therapy. It is possible that a larger sample would have permitted us to identify a low-risk group of men; however, it is likely that this subgroup would represent a small proportion of men given our sample size and that men had more recurrences than women (giving us more power to derive a rule in men). However, until a successful risk stratification tool is developed that identifies low-risk men, it appears that all men are at high risk of recurrence, particularly men with hyperpigmentation, edema or redness in either leg.
In conclusion, it may be safe for women who have taken oral anticoagulants for 5–7 months after an unprovoked venous thromboembolism to discontinue therapy if they have 0 or 1 of the following signs or symptoms: hyperpigmentation, edema or redness of either leg; a D-dimer level of 250 μg/L or more while taking warfarin; BMI 30 kg/m2 or more; and age 65 years or more.
@@ See related commentary by Kearon, page 401
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/179/5/417/DC1
This article has been peer reviewed.
Contributors: Marc Rodger and Michael Kovacs were the co-principal investigators. They, along with Susan Kahn, Philip Wells and David Anderson, designed and performed the research, collected and analyzed the data and wrote the manuscript. Grégoire Le Gal, Arnaud Perrier and Richard White performed the research, collected and analyzed the data and wrote the manuscript. Isabelle Chagnon, Susan Solymoss and Mark Crowther performed the research, collected the data and wrote the manuscript. Linda Vickars performed the research and collected the data. Tim Ramsay and Marisol Betancourt analyzed the data and wrote the manuscript. All of the authors revised the manuscript for important intellectual content and approved the final version submitted for publication.
Acknowledgements: This study was funded by the Canadian Institutes of Health Research (grant no. MOP 64319) and bioMérieux (through an unrestricted research grant).
Dr. Rodger had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All analyses were conducted independent of the funding sources.
Competing interests: Marc Rodger has received consultant's fees (which were used to support his research) from bioMérieux, which has also provided travel assistance for study-related meetings to Dr. Rodger. Susan Kahn has received speaker's honoraria from Pfizer and Sanofi-Aventis and has participated on the advisory boards of Sanofi-Aventis and Bayer. Philip Wells has received speaker's honoraria from Dade Behring, bioMérieux, Sanofi-Aventis, LEO Pharma and Organon. Isabelle Chagnon has received travel assistance from LEO Pharma to attend an international thrombosis and hemostasis meeting. Grégoire Le Gal has received travel funding from bioMérieux to attend steering committee meetings for this study and for a related study. Susan Solymoss has served as a consultant for Bayer, Boehringer Ingelheim, Pfizer and LEO Pharma, and has received speaker's fees from Pfizer and LEO Pharma. Richard White is a member of a safety-monitoring board run by Sanofi-Aventis. Tim Ramsay has received travel assistance from bioMérieux to attend a planning meeting for a follow-up study and has received an honorarium from bioMérieux used to fund a graduate student. None declared for David Anderson, Mark Crowther, Arnaud Perrier, Linda Vickars, Marisol Betancourt and Michael Kovacs.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Tailored anticoagulant treatment after a first venous thromboembolism: protocol of the Leiden Thrombosis Recurrence Risk Prevention (L-TRRiP) study - cohort-based randomised controlled trial
- Standardized Data Elements for Patients with Acute Pulmonary Embolism: A Consensus Report from the Pulmonary Embolism Research Collaborative
- Elevated plasma Complement Factor H Regulating Protein 5 is associated with venous thromboembolism and COVID-19 severity
- Contribution of the elevated thrombosis risk of males to the excess male mortality observed in COVID-19: an observational study
- Evaluation of the PADIS score stratifying risk for venous thromboembolism recurrence after a first unprovoked pulmonary embolism: results from the REVERSE study
- Does the elevated (thrombosis risk of males relative to females help account for the excess male mortality observed in Covid-19? An observational study
- Management of Patients With Venous Thromboembolism After the Initial Treatment Period
- Antithrombotic Management of Venous Thromboembolism: JACC Focus Seminar
- Pulmonary embolism: update on management and controversies
- Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis
- Extended treatment of venous thromboembolism: a systematic review and network meta-analysis
- Residual pulmonary vascular obstruction and recurrence after acute pulmonary embolism: protocol for a systematic review and meta-analysis of individual participant data
- Who should get long-term anticoagulant therapy for venous thromboembolism and with what?
- Who should get long-term anticoagulant therapy for venous thromboembolism and with what?
- The authors respond to "Thrombophilia testing in venous thromboembolism"
- Update on the management of venous thromboembolism
- A Test in Context: D-Dimer
- Long-term risk of recurrence after discontinuing anticoagulants for a first unprovoked venous thromboembolism: protocol for a systematic review and meta-analysis
- Stopping anticoagulation in a woman with unprovoked venous thromboembolism
- Optimizing diagnostic testing for venous thromboembolism
- Predicting recurrent pulmonary embolism and chronic thromboembolic pulmonary hypertension: one more way to skin the cat
- Thrombosis in the setting of obesity or inflammatory bowel disease
- Thrombosis in the setting of obesity or inflammatory bowel disease
- Prediction of bleeding events in patients with venous thromboembolism on stable anticoagulation treatment
- Personalized medicine in thrombosis: back to the future
- Systematic review of prognostic models for recurrent venous thromboembolism (VTE) post-treatment of first unprovoked VTE
- Guided duration of anticoagulation after unprovoked venous thromboembolism using D-dimer testing
- Management of Pulmonary Embolism: An Update
- How I treat recurrent deep-vein thrombosis
- Secondary Prevention of Venous Thromboembolism: One Regimen May Not Fit All
- Predicting recurrence after unprovoked venous thromboembolism: prospective validation of the updated Vienna Prediction Model
- Rationale and design of three observational, prospective cohort studies including biobanking to evaluate and improve diagnostics, management strategies and risk stratification in venous thromboembolism: the VTEval Project
- New insights into treatment of venous thromboembolism
- How Long Is Long Enough? Extended Anticoagulation for the Treatment of Cancer-Associated Deep Vein Thrombosis
- D-dimer to guide the duration of anticoagulation in patients with venous thromboembolism: a management study
- Shorter or longer anticoagulation to prevent recurrent venous thromboembolism: systematic review and meta-analysis
- Duration of anticoagulant therapy for deep vein thrombosis and pulmonary embolism
- Sex Difference in Risk of Second but Not of First Venous Thrombosis: Paradox Explained
- d-Dimer Levels Over Time and the Risk of Recurrent Venous Thromboembolism: An Update of the Vienna Prediction Model
- Thrombophilia Testing in Women with Venous Thrombosis: The 4 P's Approach
- Should the presence of an antiphospholipid antibody affect the duration of anticoagulant treatment in patients with venous thromboembolism?
- Risk assessment for recurrence and optimal agents for extended treatment of venous thromboembolism
- Antiphospholipid antibodies and the risk of recurrence after a first episode of venous thromboembolism: a systematic review
- Management of venous thromboembolic diseases and the role of thrombophilia testing: summary of NICE guidance
- Identifying Risk Factors for Venous Thromboembolism
- Managing pulmonary embolism using prognostic models: future concepts for primary care
- Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials
- Risk of recurrence after venous thromboembolism in men and women: patient level meta-analysis
- Duration of Anticoagulation: Applying the Guidelines and Beyond
- Risk Assessment of Recurrence in Patients With Unprovoked Deep Vein Thrombosis or Pulmonary Embolism: The Vienna Prediction Model
- A lower risk of recurrent venous thrombosis in women compared with men is explained by sex-specific risk factors at time of first venous thrombosis in thrombophilic families
- Preventing recurrent venous thromboembolism
- Venous Thromboembolism: Risk Factors for Recurrence
- Duration of Anticoagulant Therapy for Unprovoked Venous Thrombosis
- Stopping anticoagulant therapy after an unprovoked venous thromboembolism
More in this TOC Section
Similar Articles
Collections

