


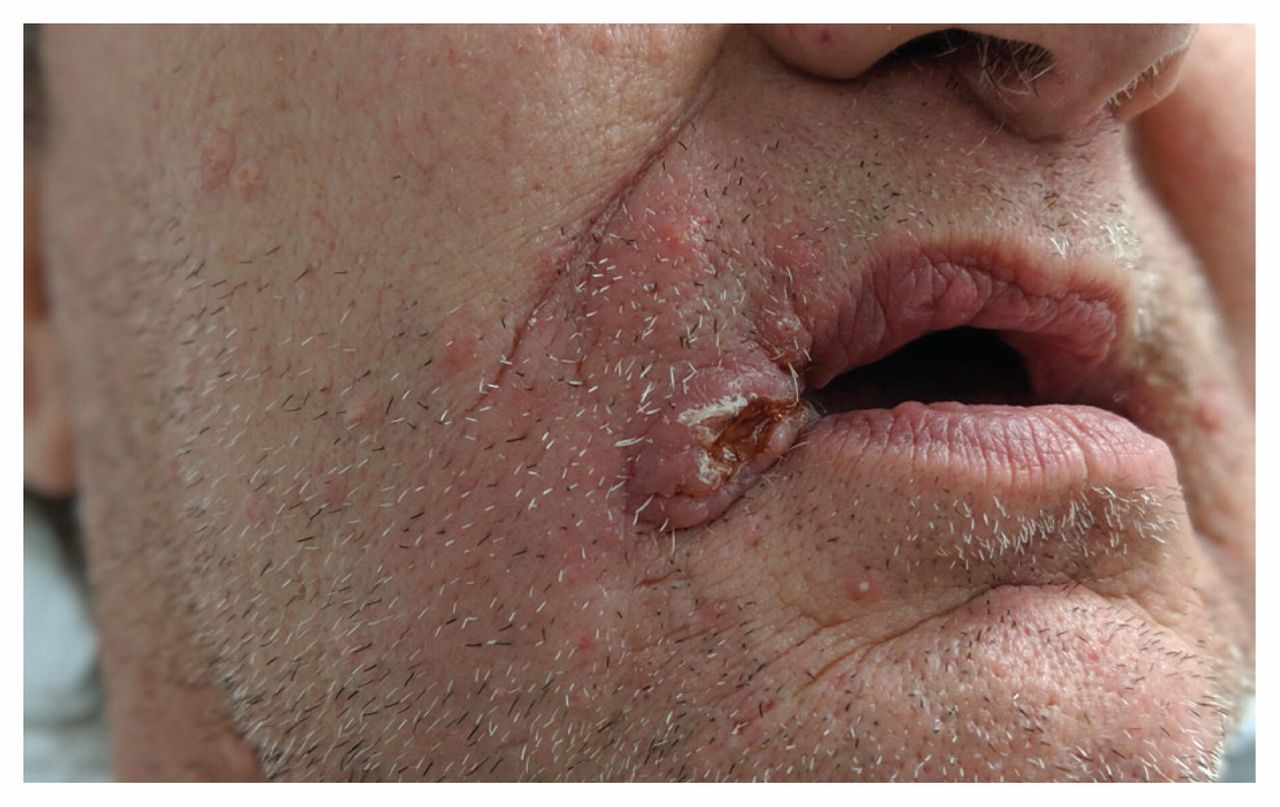
A 50-year-old man presented to the department of infectious diseases with an ulcerated nodule over the right oral commissure that had progressed over 4 weeks (Figure 1). The patient reported multiple smaller papules over his face and scalp, nontender ulcers of the hard palate (Appendix 1, Supplementary Figure 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.191540/-/DC1), dyspnea and fatigue. He had undergone lung transplantation 6 years earlier. His medications included cyclosporine, mycophenolate mofetil, prednisone and azithromycin. Six months before his presentation, the patient had built a patio in his backyard that required digging in soil.

Erythematous ulcerated nodule on the right oral commissure surrounded by several erythematous papules and discrete molluscum-like papules on the right upper cheek of a 50-year-old man with histoplamosis who underwent lung transplantation 6 years earlier.
A punch biopsy of the ulcerated nodule found numerous small yeasts within mixed inflammatory granulomas. Radiography of his chest showed bilateral micronodular pneumonia (Appendix 1, Supplementary Figure 2). Fungal cultures from the skin biopsy and bronchoalveolar lavage identified Histoplasma capsulatum. We diagnosed disseminated histoplasmosis. Our patient’s lesions and symptoms rapidly improved with oral itraconazole tablets (20 mg twice daily).
In Canada, it is estimated that an average of 27 cases of active histoplasmosis occur per year.1 Histoplasmosis is mostly found in the St. Lawrence River area of Quebec, with Ontario and Quebec being endemic, and a few cases seen in the Atlantic provinces.2 Bird and bat feces act as reservoirs. It is acquired through inhalation of environmental fungal spores. There is no human-to-human transmission. Pulmonary involvement is most commonly observed. Disseminated disease usually occurs in immunocompromised individuals and typically involves the liver, spleen, lymph nodes and bone marrow. Skin and mucosal manifestations occur in about 10% of patients with disseminated disease and can present as molluscum-like papules, nodules, vegetative plaque or ulcerative lesions.3
Ulcerative skin lesions in a recipient of lung transplantation should raise concern for opportunistic infections (e.g., mycoses, mycobacteria, Nocardia and Rhodococcus bacteria, Leishmania and sepsis-related ecthyma gangrenosum), cutaneous malignant neoplasms (including basal and squamous cell carcinomas), systemic malignant disease such as posttransplant lymphoproliferative disease or inflammatory conditions such as pyoderma gangrenosum. A skin biopsy for culture and histopathology is essential to establish a diagnosis. If histoplasmosis is suspected, additional work-up should include fungal culture of the respiratory tract, imaging of the chest, fungal blood culture, and testing for serum and urinary histoplasma antigen.
Acute histoplasmosis in immunocompetent individuals may not always require treatment.4 However, chronic mild to moderate disease can be treated with oral itraconazole, whereas severe or disseminated disease should be treated with liposomal amphotericin B. Histoplasmosis in immunocompromised individuals, regardless of severity of disease, should always be treated.5
Acknowledgements
The authors thank Dr. Charles Poirier and Dr. Sandra Davar for their contribution in the care of the patient.
Footnotes
Competing interests: Me-Linh Luong has received a researcher-initiated grant from Pfizer and consultant fees from Avir outside the submitted work. No other competing interests were declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

