


Start low, go slow” is a strategy used to minimize adverse drug events when prescribing for older people.1 However, low doses are seldom produced by pharmaceutical manufacturers and are often not paid for by provincial or hospital formularies. Although pill-splitting allows older adults to obtain the prescribed therapy, it is arduous, time-consuming and can lead to inaccurate dosing, which may result in ineffective disease management.2 This study examined the frequency of and reasons for pill-splitting in a long-term care facility.
We prospectively followed all 370 nursing home residents at the Baycrest Centre for Geriatric Care in Toronto between July 7, 1998, and Aug. 7, 1998. Any medication dispensed as a split pill to at least one resident was included in our analysis. Data were obtained from chart reviews and the Baycrest pharmacy that dispenses all medications. The main reasons for pill-splitting were classified as follows: manufacturing limitations, that is, when low doses are not manufactured or when a specific low dose is not manufactured, Ontario Drug Benefit Plan (ODB) restrictions or hospital restrictions.3 We used the Compendium of Pharmaceuticals and Specialties,4 the ODB formulary5 and the Baycrest formulary6 to determine the lowest doses provided by the pharmaceutical companies, province and nursing home respectively.
Baycrest Centre residents were 78.4% female and had a mean age of 87.9 years. Forty-one medications from 14 therapeutic groups were included in our analysis. Of the residents, 131 (35.4%) received at least one split pill and 58 (15.7%) received 2 or more split pills. In total, 422 prescriptions were dispensed, of which 157 were split. The pills most frequently split were psychotropic drugs (36.3%) and cardiac agents (19.1%).
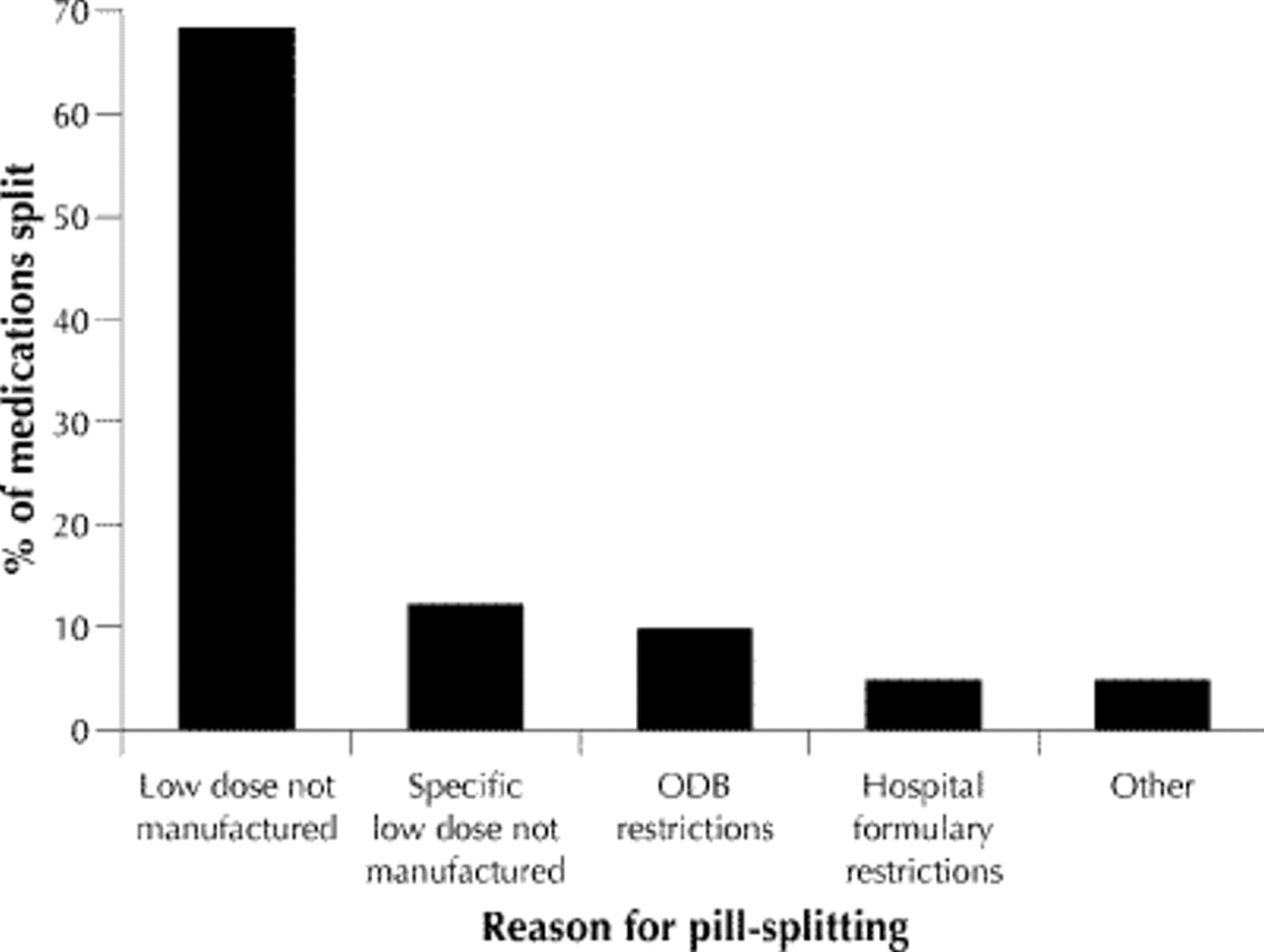
Manufacturing limitations accounted for 80.5% of pill-splitting (Fig. 1). Twenty-eight (68.3%) medications were split because low-dose formulations were not manufactured; these included olanzapine, risperidone and metoprolol. Five (12.2%) medications were split because they were not manufactured in the specific low-dose formulation prescribed, even though other low-dose formulations were available. For example, prednisone is available in a 1-mg tablet but not in the desired 2.5-mg formulation. Four (9.8%) medications were split because of ODB restrictions; these included paroxetine, sotalol, benztropine mesylate and captopril. Two (4.8%) medications were split due to hospital formulary restrictions; these were clonazepam and simethicone. Two medications (4.8%), warfarin and donepezil, were split for other reasons: convenience and cost savings respectively.
{kind=link}
Fig. 1: Distribution of reported reasons for pill-splitting. ODB = Ontario Drug Benefit Plan. The “other” category represents 2 cases of pill-splitting. In one, it was a more convenient dispensing practice for the staff pharmacist, and in the other the pharmacist wanted to save the resident money by splitting the pill.
Our results suggest that pill-splitting is widespread in this long-term care facility. Our study serves to heighten clinicians' awareness of the problems associated with pill-splitting and advocates the manufacture of low-dose forms. Our finding of frequent pill-splitting is consistent with the findings of Rochon and colleagues who demonstrated that more than a quarter (26%) of Ontario seniors on thiazide diuretics had to split pills due to manufacturing limitations.7 Pill-splitting is a concern because it can lead to inaccurate dosing that may limit the pill's effectiveness. McDevitt and coworkers showed that about 40% of manually split hydrochlorothiazide tablets deviated from their ideal weight by more than 10%.2 At Baycrest, the pills most frequently split include cardiac and psychotropic agents, which are essential, nondiscretionary drugs. Soumerai and colleagues demonstrated that noncompliance with nondiscretionary therapies can lead to deteriorating health and increased risk of needing institutional care.8 This finding suggests that older people may not be receiving the appropriate dose needed to manage their health conditions.
Pill-splitting occurs frequently in long-term care facilities but also has implications for older adults still living in the community. Manufacturers should produce lower-dose tablets, particularly for essential therapies, to meet the needs of older people. Hospital and provincial formularies should include financial coverage of low-dose formulations. Health professionals should be aware that pill-splitting may limit the efficacy of the medication prescribed.
Footnotes
-
This article has been peer reviewed.
Contributors: All the authors contributed to the idea and development of the study. Ms. Fischbach, Ms. Gold and Ms. Lee were responsible for the data collection. All the authors participated in writing the manuscript.
Competing interests: None declared.
Reprint requests to: Dr. Paula A. Rochon, Kunin-Lunenfeld Applied Research Unit, Baycrest Centre for Geriatric Care, 3560 Bathurst St., Toronto ON M6A 2E1; fax 416 785-2378; [email protected]
In this issue
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles

