


Antiphospholipid syndrome
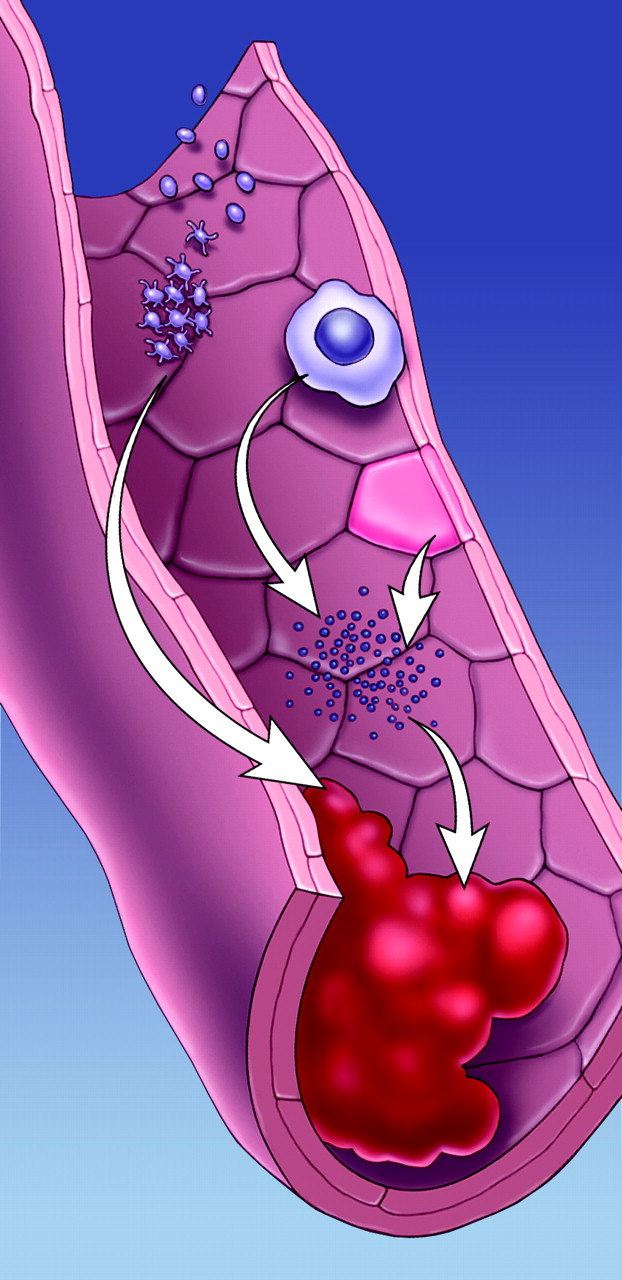
Figure. Photo by: Myra Rudakewich
A diagnosis of antiphospholipid syndrome can be made in a patient who has a history of either vascular thrombosis or fetal loss and has specific antibodies, detected by laboratory testing. This seemingly simple diagnosis is in contrast to the complex origins of the syndrome's pathogenic mechanisms. Although research efforts have shown an association with autoantibodies specific for phospholipid-binding proteins, the precise etiology remains hidden. John Hanly describes what is known about the pathophysiology of this occasionally catastrophic syndrome and comments on its clinical manifestations and treatment.
See page 1675
The clinical course of SARS in health care workers
After a brief reprieve, severe acute respiratory syndrome (SARS) in Toronto has bounced back. In other places, such as China, it simply has not gone away. Although several descriptions of SARS cases have been published, most have taken the form of large summary reports. Monica Avendano and colleagues describe the specific clinical and laboratory features of the cases of SARS diagnosed in 14 health care workers in Toronto and report on their health status at 3 weeks post discharge. They present individual data for all of these patients and comment on their response to empiric treatment with ribavirin and steroids. In all patients, ribavirin was stopped because of a high number of adverse events attributed to the drug. All patients survived, none needed respiratory support and none have transmitted any infection since discharge.
See page 1649
The cost of diabetes mellitus
About 5% of Canadians over the age of 12 years have diabetes mellitus and are therefore at increased risk of macrovascular and microvascular complications. It has been estimated that, in 1998, the direct medical cost of diabetes was 8% of total medical expenditures in Canada; however, the methods used to reach this estimate have been criticized. Scot Simpson and colleagues used Saskatchewan Health's health care databases to identify individuals with diabetes and linked this cohort to medical expenditures for diabetes and its complications. They found that the medical costs incurred by the 3.6% of people in Saskatchewan who had diabetes accounted for about 15% of total provincial expenditures on admissions to hospital, physician services and prescription drugs.
See page 1661
Management of pregnancy, labour and delivery in HIV-positive women

Figure. Photo by: Digital Stock
Over 19 million women are infected with HIV world wide and, as we become better at treating their disease, they are living longer and healthier lives. Some choose to become pregnant, whereas for other HIV-positive women pregnancy is an unplanned circumstance with which they must cope. Perinatal transmission from mother to child is an important source of HIV infection, but this can be ameliorated with the proper treatment of mother and child. David Burdge and colleagues present Canadian consensus guidelines that provide evidence-based recommendations to practitioners involved in all stages of pregnancy management of HIV-positive patients, including proper care for their infants. In an associated piece in the Practice section, these authors outline 7 common clinical scenarios and describe the practical application of the guidelines in these cases.
In this issue
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

