


A 76-year-old man with a past history of hypertension, diabetes and cerebrovascular disease presented with nonresolving pneumonia. He was a long-time smoker. He underwent bronchoscopy and was found to have an endobronchial carcinoid tumour in the bronchus intermedius (Fig. 1, Panel A). Because of his comorbidities and the relatively indolent nature of carcinoid tumours, bilobectomy was not undertaken and the patient was referred for possible endobronchial resection with electrocoagulation.1 Patients for whom this treatment modality is considered are routinely investigated with CT scans of the chest to determine whether the tumour has spread through the bronchial wall. If the bronchial wall is compromised, curative endobronchial resection is not possible, because the tumour cannot be completely removed without perforating the airway.
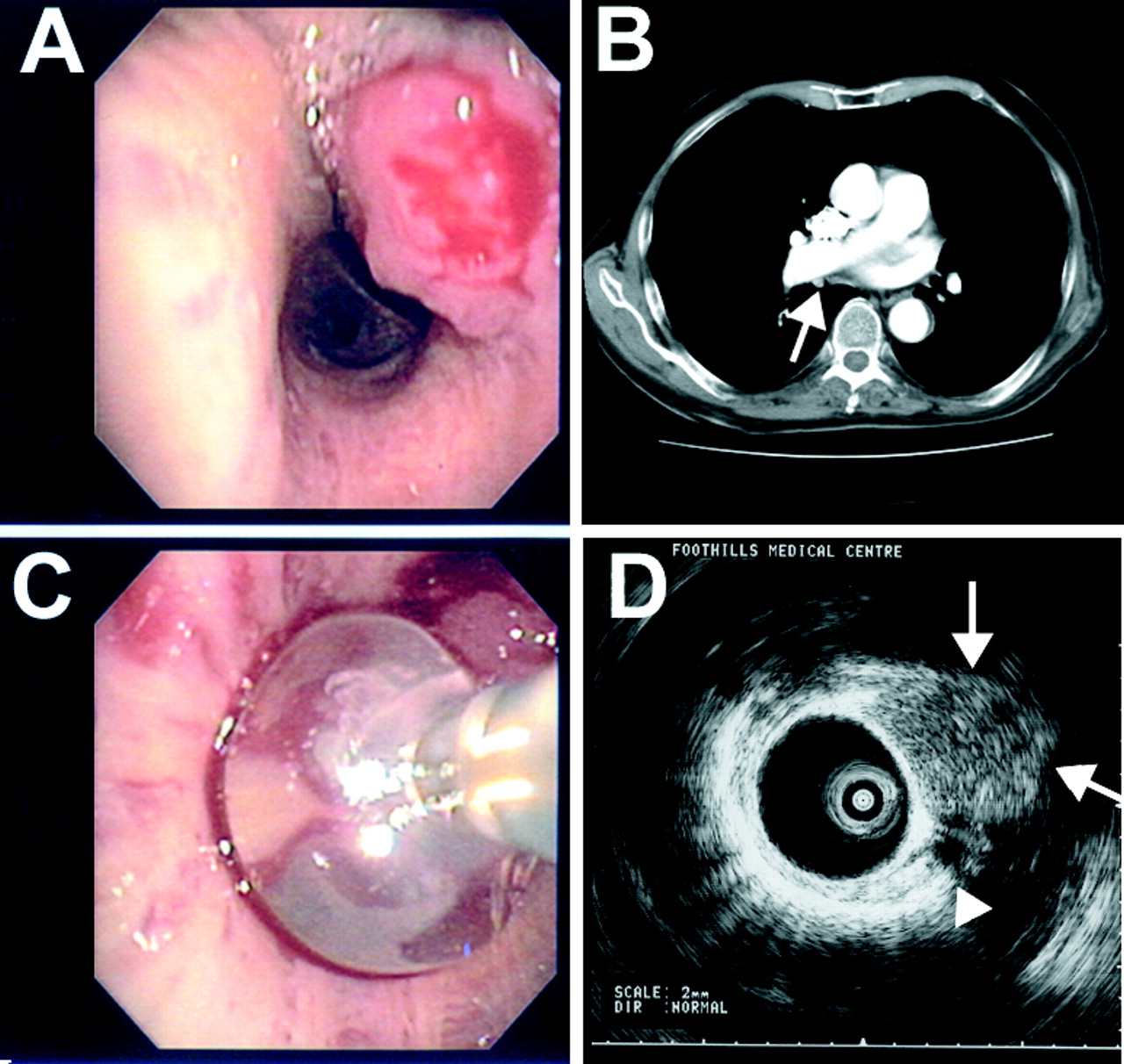
Figure 1. Photo: Images courtesy of Dr. Alain Tremblay.
For our patient, it was not possible to determine whether the bronchial wall was compromised (Panel B, white arrow) using a thoracic CT scan with thin-section cuts. It was decided with the patient's consent that a relatively new technique, endobronchial ultrasonography (EBUS),2 would be used to help resolve the issue. EBUS involves the insertion of a 2.6-mm ultrasound probe into a dedicated balloon sheath (UM-BS20-26R 20-MHz probe, MAJ-643R sheath; Olympus, Melville, NY) that can be inserted into the working channel of a flexible bronchoscope (diameter of working channel is 2.8 mm). With the patient under conscious sedation, the flexible bronchoscope is advanced in the usual fashion and the balloon is inflated with saline in the area of interest to create an imaging window free of air, which would make clear ultrasound images difficult to obtain. EBUS was performed in our patient at the level of the lesion (Panel C). At the same time, ultrasound radial images of the tissues adjacent to the probe are obtained in real time. Unfortunately in our patient's case, the lesion (Panel D, white arrows) has destroyed the bronchial wall (Panel D, white arrowhead), which is usually seen as a multilayered structure. This made this patient ineligible for curative endobronchial resection. He has had no recurrence of pneumonia to date, but should he develop obstructive symptoms in the future a palliative (partial) endobronchial resection could be considered.
Although further study is needed, EBUS appears to be a useful, safe and relatively simple tool to allow bronchoscopists to see beyond the airway wall, thus expanding the reach of the bronchoscope.
Alain Tremblay Division of Respiratory Medicine Department of Medicine University of Calgary Calgary, Alta.
In this issue
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

