


A previously healthy 38-year-old woman had undergone laparoscopic left ovarian cystectomy because of endometriosis. She had previously undergone 2 cesarean sections. Two months after the cystectomy, she had sudden onset of diffuse abdominal pain and distension as well as dysuria. Examination revealed no localized or peritoneal signs but did show substantial ascites. The laboratory test results were normal except for an elevated serum creatinine level (198 [normal < 133] μmol/L). Noncontrast CT scanning showed free fluid in her abdomen and a thickened omentum. One litre of straw-coloured ascitic fluid was aspirated; the leukocyte count was 0.50 [normal < 0.25] х 109/L (lymphocytes 55%, neutrophils 45%).
Tuberculosis of the abdomen was suspected. However, this diagnosis was unlikely because the ascites, dysuria and abdominal pain resolved spontaneously within 48 hours after aspiration of the ascitic fluid, and renal function returned to normal within 72 hours.

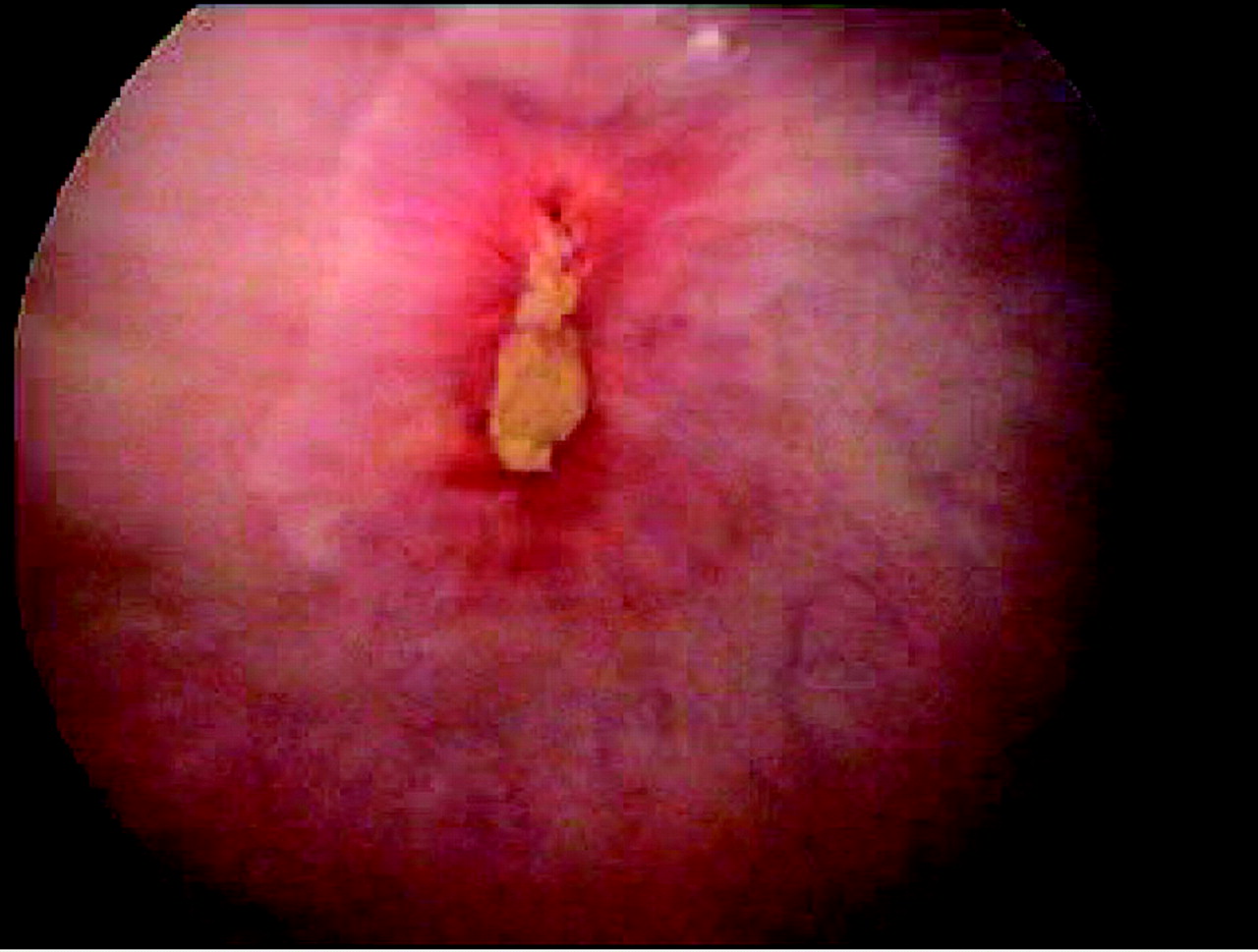
One month later the patient was reassessed and found to have ascites with generalized abdominal tenderness and guarding in the hypogastrium, which worsened over 24 hours. Oliguria (serum creatinine level 180 μmol/L) and, subsequently, anuria (serum creatinine level 675 μmol/L) developed. A catheter was inserted, and brisk diuresis of more than 5 L resulted in her renal function rapidly returning to normal. The creatinine level of the ascitic fluid was grossly elevated (2178 μmol/L), which confirmed the diagnosis of urinary ascites. Ultrasonography revealed kidneys of normal size, and noncontrast CT scanning did not show obvious bladder injury but did reveal a fat density lesion in the bladder. Contrast-enhanced CT scanning showed normal kidneys and ureters and a tongue of fat, probably omental tissue, adherent to the anterior wall of the bladder. CT cystography did not reveal any urinary leak. Cystoscopy, performed to identify the bladder perforation, revealed that omentum was plugging the defect at the dome of the bladder (Fig. 1). Laparotomy was performed to close the bladder perforation, and the patient had an uneventful recovery.
Bladder injury is a known complication of gynecologic laparoscopic surgery, occurring in up to 8.3% of cases,1 and is more common in women who have undergone previous pelvic operations. The diagnosis of accidental intraperitoneal bladder injury may be delayed2 if the injury is trivial or if omentum plugs a larger defect, as was seen in our case. Unexplained ascites and decreased renal function in a previously healthy person with a recent history of pelvic surgery should raise the suspicion of intraperitoneal bladder rupture. Our patient's first episode of ascites resolved without treatment, probably because of spontaneous evacuation of urine through the bladder defect. A very high creatinine level in the ascitic fluid is diagnostic.3 Treatment should involve conventional or CT cystography to localize the bladder perforation, followed by laparotomy to repair it.
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

