


What's your call?
Figure Six weeks after a 49-year-old woman underwent an instrumented cervical fusion procedure, she experienced pain at her left iliac crest and weakness in her left hip. Plain radiographs show her pelvis in an anteroposterior view (left) and with the left hip in abduction (right).
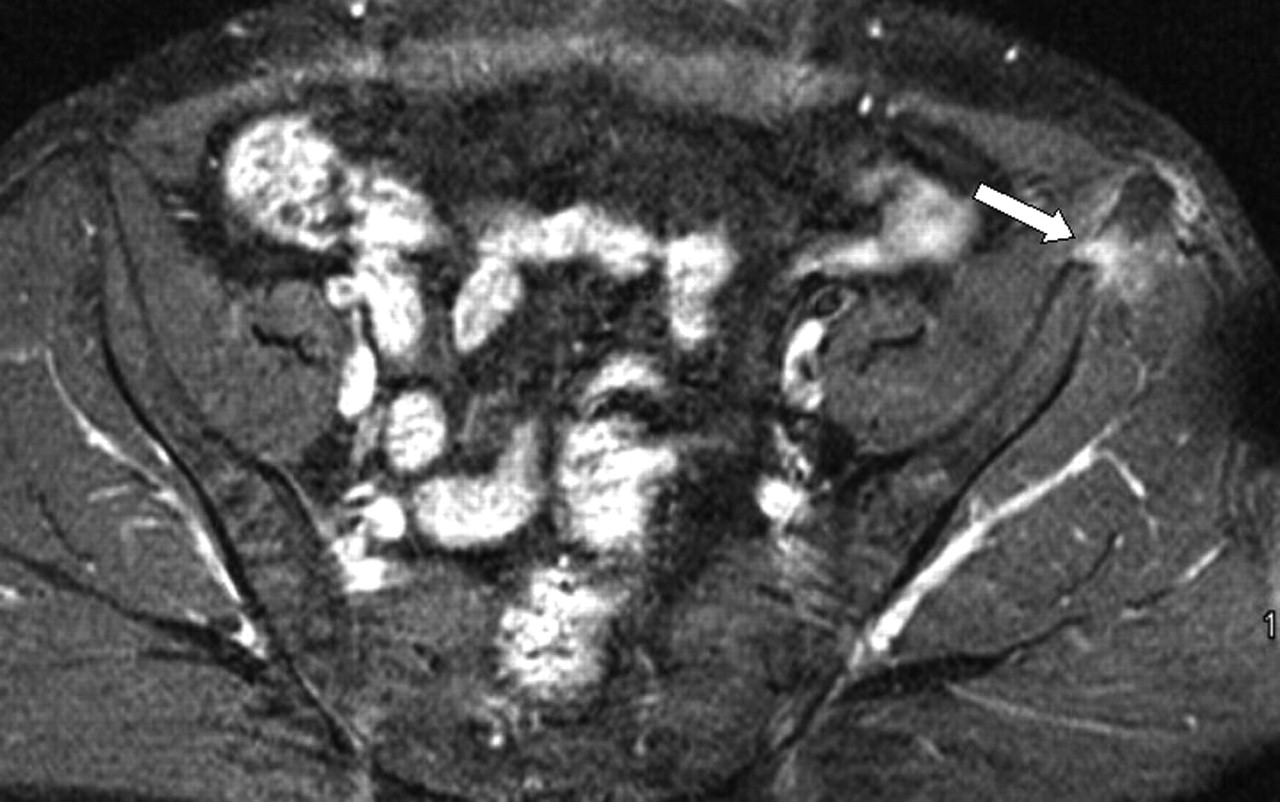
This patient, a smoker with cervical spondylotic myeloradiculopathy, had required a C4–C5 anterior cervical discectomy and fusion with a tricortical autograft harvested with a sagittal saw and osteotome from her left anterior iliac crest, and anterior cervical plate fixation. Six weeks after surgery her myeloradiculopathic symptoms had improved, but she was experiencing acute pain at her graft-harvest site despite no history of trauma. Plain film radiographs revealed an avulsion fracture of her left anterior superior iliac spine (ASIS), confirmed by MRI (Fig. 1).

Fig. 1: Axial MRI of the pelvis, 6 weeks after the patient's autograft operation. It shows a left avulsion fracture (arrow) of the left anterior superior iliac spine, with edema at the fracture site.
Initially she was treated conservatively with modified activity, analgesics, anti-inflammatory medications and physical therapy. Two years later her pain was still present but much reduced, and a CT scan revealed bone healing at the fracture site (Fig. 2).

Fig. 2: Axial CT of the pelvis 2 years after surgery, showing bone healing at the fracture site (arrow).
The iliac crest, which is rich in cancellous, cortical and corticocancellous bone stock and the osteocompetent cells necessary for optimal bone fusion, is a common donor site for bone grafts. Avulsion fracture of the ASIS is an uncommon adverse event after graft harvesting. More common complications at the ASIS after harvesting include neural and vascular injuries, hematoma, infection, chronic pain, and cosmetic defects. Avulsion fractures may occur because of altered stresses by the sartorius and tensor fascia lata muscles.
Although predisposing risk factors are not yet certain, the patients who seem to be at greatest risk of such fractures are those in whom graft material was harvested less than 5 cm from the ASIS (Clin Orthop Relat Res 1986;Aug:224-6) and in whom an osteotome was used (Spine 1993;18:2048-52). Reduced bone density may also play a role, since such fractures occur more often in women (6:1 females to males) who are mostly in the fifth decade of life (J Oral Maxillofac Surg 2004;62:781-6).
Footnotes
-
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

