


The case: A 1-year-old girl presented to hospital with fever, lethargy and vomiting. She had had an episode of Escherichia coli meningitis at 2 months of age, which had been treated with antibiotics. No further investigation was conducted at that time. The remainder of her medical history was unremarkable.
On examination, the child was febrile, lethargic and cried with neck flexion. She had a port-wine stain over her lumbar spine at the midline (Fig. 1). Lumbar puncture revealed a leukocyte count of 3340 × 106/L (normal value < 5 × 106/L) with 78% polymorphs, an erythrocyte count of 110 × 106/L, a glucose level of 1.9 mmol/L (the serum glucose level was 13.3 mmol/L) and a protein level of 0.74 g/L (normal 0.15–0.40 g/L). Results of blood and urine cultures were negative. Her cerebrospinal fluid tested positive for E. coli. In addition, growth of Peptoniphilus asaccharolyticus was noted.

Fig. 1: Port-wine stain over lumbar spine at midline of 1-year-old child with recurrent meningitis.
There was no history of recurrent infection or head trauma. Results of tests for HIV infection and immunodeficiency were negative. A spinal MRI scan revealed 3 lesions in the lumbar region compatible with epidermoid or dermoid cysts. A sinus tract extending from the skin into the third extradural lesion was also noted (Fig. 2). On more careful clinical assessment, with rostral and caudal traction of the skin, tethering of the skin was seen supporting the presence of a sinus tract, and an overlying pustule was evident in the centre of the port-wine stain (Fig. 3).

Fig. 2: Spinal MRI scan, showing 3 lesions in lumbar region compatible with epidermoid or dermoid cysts, and sinus tract extending from skin into third extradural lesion.

Fig. 3: Rostral and caudal traction of skin revealed presence of sinus tract and overlying pustule in centre of port-wine stain.
In consultation with infectious disease specialists, a 6-week course of meropenem, amikacin and vancomycin was administered. The child then underwent neurosurgical excision of the sinus tract and resection of the cystic lesions. Pathology revealed the presence of hair elements, which confirmed the diagnosis of dermoid cysts.
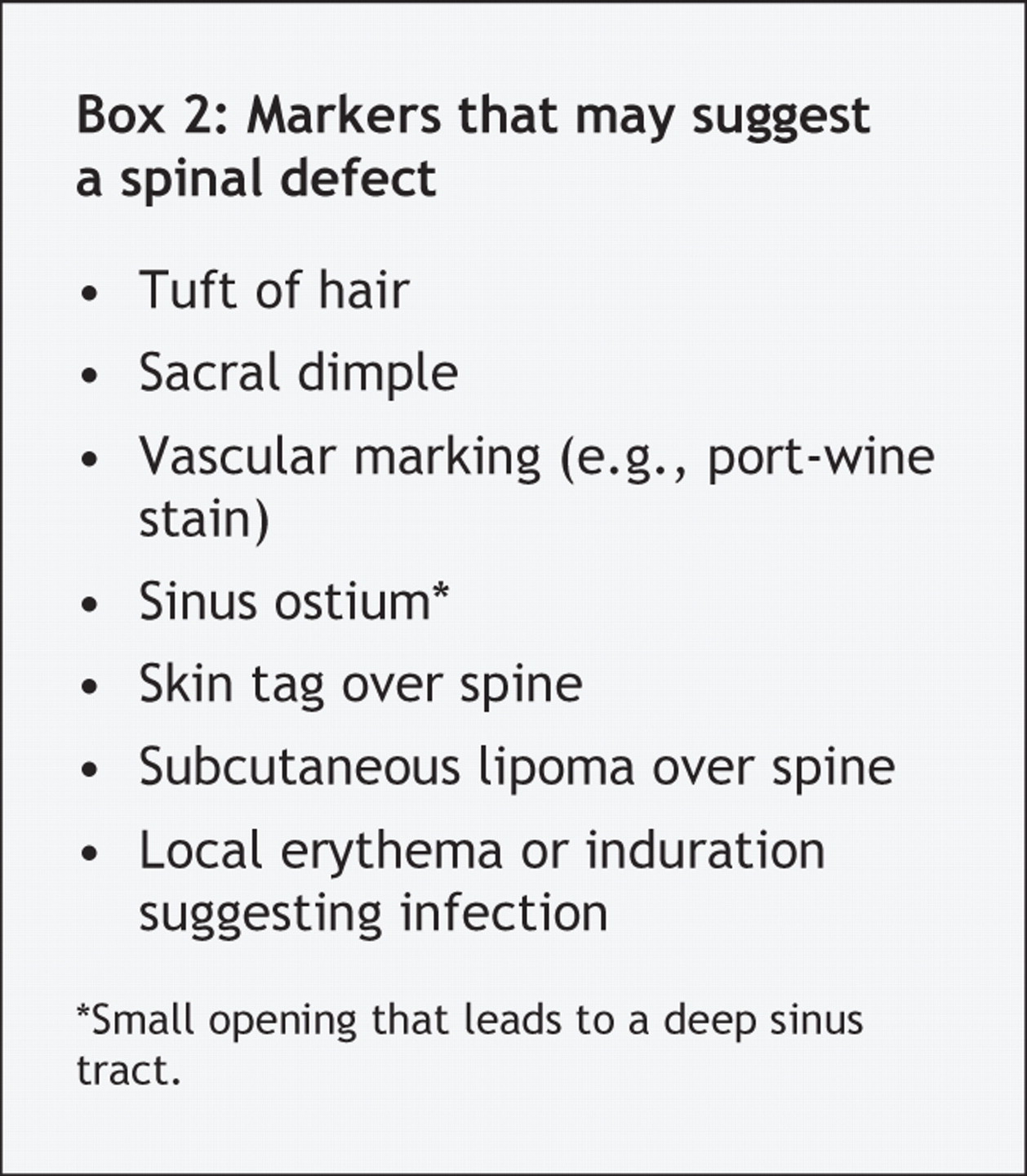
Recurrent meningitis can lead to significant morbidity and mortality. Careful history taking, physical examination and investigations are required to rule out causes of recurrent bacterial meningitis (Box 1). Examination of a newborn's back is important to check for signs that suggest an underlying spinal defect (Box 2). Possible spinal defects include dermal sinus tracts, intraspinal cysts, intraspinal lipomas or other tumours, and tethered spinal cord. These abnormalities may lead to progressive weakness or sensory loss in the lower extremities, gait abnormalities, bowel and bladder dysfunction, and foot deformities.

More than 90% of patients with an occult spinal abnormality have a cutaneous marker over the lower spine. However, if only 1 cutaneous marker is present, spinal defects are found in less than 1% of patients. The presence of 2 or more cutaneous markers increases the likelihood of an occult spinal abnormality.1 A coccygeal pit (Fig. 4) is not associated with any intradural pathology and should be differentiated from a sacral dimple. Coccygeal pits are small, less than 5 mm in diameter, are located in the midline within 2.5 cm of the anus and may be present in up to 4% of the normal population.1,3 Sacral dimples, on the other hand, are usually larger than 5 mm in diameter, are located above the intergluteal cleft and are often found with other cutaneous markers. Current recommendations state that spinal ultrasounds should be performed in infants less than 4–6 months of age with any cutaneous marker over the spine.4

Fig. 4: Simple midline dimple (coccygeal pit) in newborn. Coccygeal pits are not associated with any intradural pathology. Reproduced, with permission, from Kriss et al.2
All newborns should have a careful physical examination, which includes their back. If a cutaneous abnormality is seen, rostral and caudal traction of the skin may identify the presence of a sinus tract. The ease and availability of spinal ultrasound makes it a valuable screening tool. If an abnormality is found or the test result is unclear, then an MRI scan is recommended. Nonurgent referral to a neurosurgeon can be made if the results of neurologic examination are normal. An urgent referral must be made if an infection is present or neurologic deficits are detected.
Footnotes
-
Acknowledgements: I thank Dr. Jeremy Friedman for his thoughtful review of the initial draft of the manuscript and Dr. Peter Dirks for his teaching and the photographs.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

