


Diabetic retinopathy is a leading cause of blindness in adults in developed countries
Diabetic retinopathy is diagnosed by funduscopic examination after pupil dilation and is categorized into nonproliferative and proliferative types. Non-proliferative changes include microaneurysms, intraretinal hemorrhages, intraretinal micro-vascular abnormalities and cotton wool spots; proliferative retinopathy refers to neovascularization of the optic disc or elsewhere (Figure 1).1 Loss of vision is usually secondary to macular edema, macular ischemia, vitreous hemorrhage or tractional detachment of the retina.
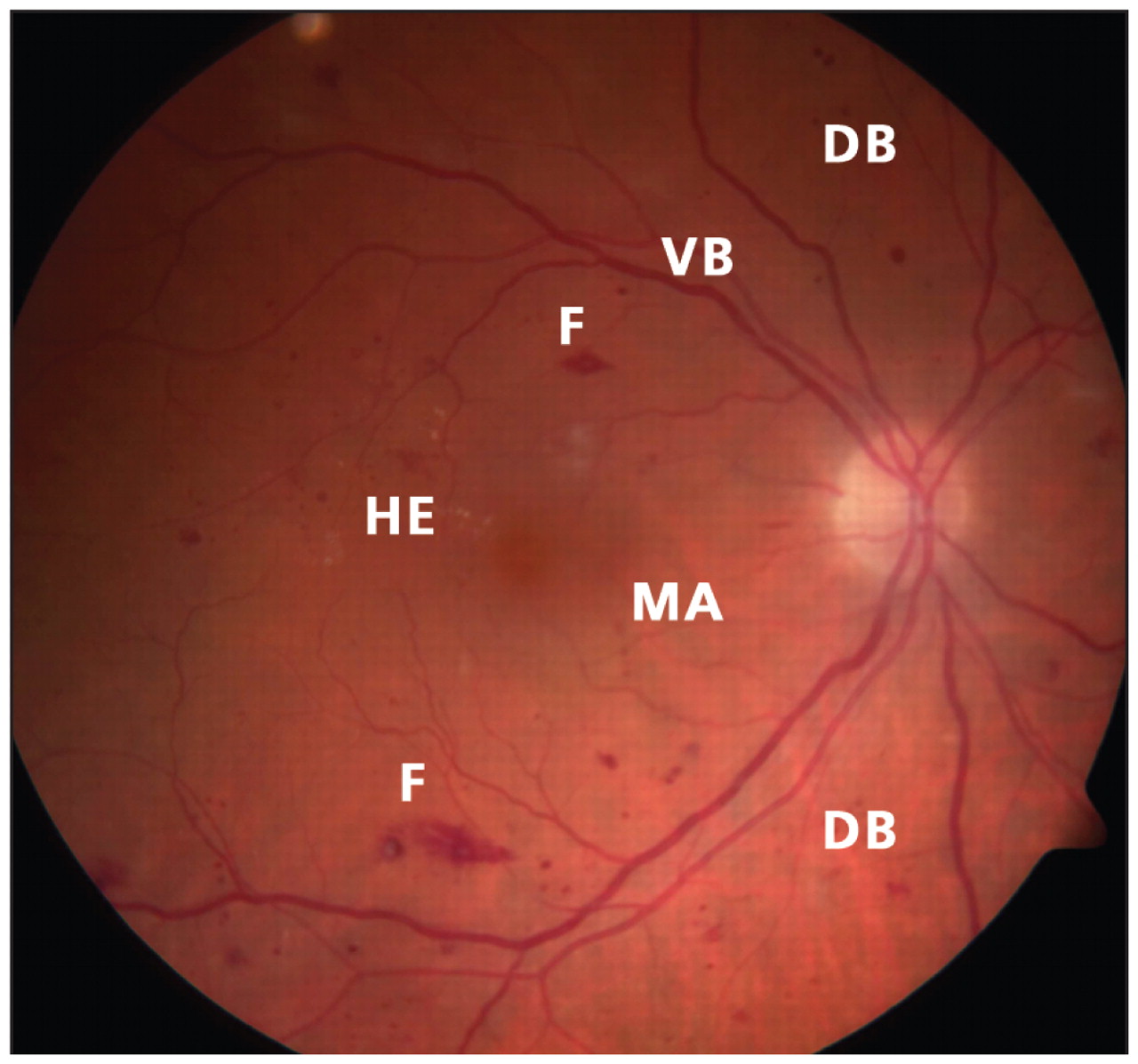
Figure 1: Fundus of the right eye showing characteristic features of nonproliferative diabetic retinopathy, including dot-blot hemorrhages (DB), flame-shaped hemorrhages (F), hard exudates (HE), micro-aneurysms (MA) and venous beading (VB).
Patients with diabetes should undergo routine funduscopic examination with pupil dilation
Patients with type 1 diabetes should have their eyes examined within five years of diagnosis. Those with type 2 diabetes should be referred at the time of diagnosis, since nearly 30% will already have diabetic retinopathy. The frequency of follow-up examinations will depend on the severity of the retinopathy at diagnosis. Typically, patients with early disease require annual examination, whereas those with more advanced retinopathy or who are pregnant will need more frequent follow-up.2
The risk of diabetic retinopathy is directly related to the duration of diabetes and the severity of hyperglycemia
Among patients with type 1 diabetes, 25%, 60% and 80% will have retinopathy after 5, 10 and 15 years of disease.3 Among patients with type 2 diabetes, 40% who use insulin and 24% who do not use insulin will have retinopathy at five years; the proportions will increase to 84% and 53%, respectively, at 19 years.4 Poor glycemic control, smoking, hyperlipidemia, hypertension, anemia and nephropathy are associated with progression of diabetic retinopathy.
Strict control of blood glucose levels and blood pressure remain key strategies for decreasing the risk of diabetic retinopathy or slowing its progression
Studies from the Diabetes Control and Complications Trial Research Group and the United Kingdom Prospective Diabetes Study Group both showed significant reductions in the development of diabetic retinopathy among patients who intensely controlled their blood glucose levels.3,4 Control of blood pressure and serum lipid levels can slow the progression of the retinopathy.
Key treatments are laser photo-coagulation and vitrectomy
Panretinal photocoagulation for high-risk proliferative retinopathy can reduce the risk of severe visual loss by 50%.1 For those with clinically significant macular edema, macular laser can reduce the risk of moderate visual loss by 50%.1 Vitrectomy improves vision in patients with nonclearing vitreous hemorrhage or retinal detachment. Intravitreal injection with pharmacologic agents such as triamcinolone acetonide and bevacizumab has shown promise in the treatment of macular edema and neovascularization, respectively. However, there is no proven intervention that works in all patients.5
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared
For references, please see Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090536/DC1
Previously published at www.cmaj.ca
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Diabetic retinopathy is a leading cause of blindness in adults in developed countries
- Patients with diabetes should undergo routine funduscopic examination with pupil dilation
- The risk of diabetic retinopathy is directly related to the duration of diabetes and the severity of hyperglycemia
- Strict control of blood glucose levels and blood pressure remain key strategies for decreasing the risk of diabetic retinopathy or slowing its progression
- Key treatments are laser photo-coagulation and vitrectomy
- Footnotes
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

