


Abstract
Background: The foreign-born population bears a disproportionate health burden from tuberculosis, with a rate of active tuberculosis 20 times that of the non-Aboriginal Canadian-born population, and could therefore benefit from tuberculosis screening programs. We reviewed evidence to determine the burden of tuberculosis in immigrant populations, to assess the effectiveness of screening and treatment programs for latent tuberculosis infection, and to identify potential interventions to improve effectiveness.
Methods: We performed a systematic search for evidence of the burden of tuberculosis in immigrant populations and the benefits and harms, applicability, clinical considerations, and implementation issues of screening and treatment programs for latent tuberculosis infection in the general and immigrant populations. The quality of this evidence was assessed and ranked using the GRADE approach (Grading of Recommendations Assessment, Development and Evaluation).
Results: Chemoprophylaxis with isoniazid is highly efficacious in decreasing the development of active tuberculosis in people with latent tuberculosis infection who adhere to treatment. Monitoring for hepatotoxicity is required at all ages, but close monitoring is required in those 50 years of age and older. Adherence to screening and treatment for latent tuberculosis infection is poor, but it can be increased if care is delivered in a culturally sensitive manner.
Interpretation: Immigrant populations have high rates of active tuberculosis that could be decreased by screening for and treating latent tuberculosis infection. Several patient, provider and infrastructure barriers, poor diagnostic tests, and the long treatment course, however, limit effectiveness of current programs. Novel approaches that educate and engage patients, their communities and primary care practitioners might improve the effectiveness of these programs.
The cases
Ousman, a 32-year-old man; his 8-year-old daughter, Nene; and his 65-year-old mother, Mariama, from Casamance, Senegal, speak only Wolof and arrived in Canada six months ago from a refugee camp. What, if any, screening for latent tuberculosis should be done for this family?
Active pulmonary tuberculosis was recently diagnosed in Harjit, a 65-year-old man who immigrated to Canada from India at age 32. Diabetes was diagnosed when he was 40 years old, and chronic renal failure developed one year ago that required dialysis because of the diabetes. Should screening for latent tuberculosis have been done for this man, and if so when?
Introduction
Tuberculosis is an airborne transmissible disease that causes a substantial burden to patients, their contacts and society. Although tuberculosis is relatively uncommon in Canada (1621 cases reported in 2006), it is costly ($58 million in direct costs in Canada in 2004), treatment is lengthy, many patients require admission to hospital, and the mortality rate in patients with tuberculosis is still high (11%).1,2
The foreign-born population bears a disproportionate burden of tuberculosis in Canada; 65% of all cases of active tuberculosis occur in foreign-born patients although they make up only 20% of the population.3 This is because most recent immigrants and refugees originate from countries with a high incidence of tuberculosis, and up to half harbour latent tuberculosis infection and are at risk of active tuberculosis.2 Successful control of tuberculosis in Canada will depend on decreasing rates of tuberculosis in the foreign-born population. We conducted a review to quantify the burden of tuberculosis in the migrant population, to identify those at highest risk of active tuberculosis, to describe the effectiveness of screening and treatment programs for latent tuberculosis, to identify barriers or challenges to implementation of such programs and to highlight possible interventions to improve these programs. The recommendations for preventing tuberculosis from the Canadian Collaboration for Immigrant and Refugee Health are found in Box 1.
Recommendations for preventing tuberculosis from the Canadian Collaboration for Immigrant and Refugee Health
Children
Screen children and adolescents < 20 years of age from countries with a high incidence of tuberculosis (smear-positive pulmonary tuberculosis > 15 per 100 000 population) as soon as possible after their arrival in Canada with a tuberculin skin test and recommend treatment for latent tuberculosis infection if results are positive, after ruling out active tuberculosis.
Adults
Screen all refugees between 20 and 50 years of age from countries with a high incidence of tuberculosis as soon as possible after their arrival in Canada with a tuberculin skin test. Screen all other adult immigrants who have risk factors that increase the risk of active tuberculosis with a tuberculin skin test and recommend treatment for latent tuberculosis infection if results are positive, after ruling out active tuberculosis.
Basis of recommendations
Balance of benefits and harms*
The decision about whom to screen and offer treatment for latent tuberculosis is based on the balance between the potential benefit of treatment (decreasing the lifetime risk of active tuberculosis, which is influenced by age, presence of underlying medical conditions and immigration category) versus the potential harm of hepatotoxicity (which increases with age) and the poor effectiveness of isoniazid in many settings because of suboptimal uptake of screening and treatment. For several groups, screening for latent tuberculosis should be routinely performed, and those with positive results should be offered treatment. These groups are children from countries with a high incidence of tuberculosis (number needed to treat [NNT] 20–26, number needed to harm [NNH] 134–268), adults with risk factors for active tuberculosis (NNT 3–20, NNH variable) and refugees < 50 years of age (NNT 15–26, NNH 49). Screening for latent tuberculosis and offering treatment could also be considered for adult refugees 50–65 years of age (NNT 20–51, NNH 9–18) and other adults without underlying medical conditions < 65 years of age if adherence to treatment can be assured and hepatotoxicity carefully monitored to minimize harm. A decision to screen is a decision to offer treatment and to ensure adherence to treatment with appropriate counselling and monitoring.
Quality of evidence
High
Values and preferences
The guideline committee attributed more value to screening and treating latent tuberculosis infection to prevent active disease in patients and to prevent transmission of active disease and less value to the practitioner burden of screening and counselling.
-
↵* Estimated NNT and NNH are based on the following assumptions: seven years after arrival, the annual risk of active tuberculosis is 0.1%; the relative risk of active tuberculosis is highest upon arrival and decreases with time (relative risk 5.1, compared with 1.4 seven years after arrival); the patient will live to age 80 years; the efficacy of isoniazid is 90%; and adherence is 70%.
Methods
We used the 14-step approach developed by the methods team of the Canadian Collaboration for Immigrant and Refugee Health.4 The Clinician Summary Table highlights the population of interest, the epidemiology of disease within this population, population-specific considerations and potential key clinical actions (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.090302/DC1). We then constructed a logic model to define the clinical preventive actions (intervention), outcomes and key clinical questions. Details of the review are summarized in the tuberculosis technical document (www.ccirh.uottawa.ca).
Search strategy for systematic reviews, guidelines and population-specific literature
We designed a search strategy in consultation with a librarian to identify relevant systematic reviews and guidelines to address the burden of tuberculosis and the effectiveness of screening programs for tuberculosis (latent and active) in the immigrant population. For this search, we reviewed five electronic databases: MEDLINE (Ovid), MEDLINE In-Process, EMBASE, CINAHL and the Cochrane Database of Systematic Reviews from 1950 to Dec. 17, 2008. We conducted a similar search for the general population, with the same five databases and the same objectives but restricted the search dates to Jan. 1, 1996 to Dec. 17, 2008. We performed a separate search for tuberculosis among immigrants to address population-specific concerns including baseline risk or prevalence compared with the Canadian-born population; risk of clinically important outcomes; genetic and cultural factors (e.g., preferences, values, knowledge); and compliance variation using the same five databases (1950 to Dec. 17, 2008). An updating search, focusing on randomized controlled trials and systematic reviews during the period Jan. 1, 2007 to Jan. 1, 2010, was conducted to identify any recent publications that would change the position of the recommendation. We performed a Web-based search until September 2007 to identify guidelines on tuberculosis screening and treatment in the following websites: the CMA Infobase; the National Guideline Clearing House; the Canadian Task Force on Preventive Health Care; the Public Health Agency of Canada; the Canadian Lung Association; the US Preventive Task Force; Centers for Disease Control and Prevention; Infectious Disease Society of America; American Thoracic Society; National Institute for Health and Clinical Excellence; and the World Health Organization. We appraised eligible systematic reviews using the critical appraisal tool of the National Institute for Health and Clinical Evidence to assess systematic approach, transparency, quality of methods and relevance. We assessed relevant guidelines using the Appraisal of Guidelines for Research and Evaluation (AGREE) Instrument (www.agreecollaboration.org).
Synthesis of evidence and values
Evidence from systematic reviews, cohort studies and clinical trials using the summary of findings table from Grading of Recommendations Assessment, Development and Evaluation (GRADE) (Box 2), which assesses both relative and absolute effects of interventions (relative risk and absolute event rate), was synthesized. We appraised quality of data for each outcome using the GRADE quality assessment tool, which assesses study limitations, directness, precision, consistency and publication bias across all studies. In the search and synthesis of data on concerns specific to immigrants, clinically relevant considerations and implementation issues, as well as gaps in the research and evidence base, were identified.
Grading of Recommendations Assessment, Development and Evaluation Working Group grades of evidence (www.gradeworkinggroup.org)
-
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
-
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
-
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
-
Very low quality: We are very uncertain about the estimate.
Results
In the search for systematic reviews and guidelines for immigrants, 176 records were identified and screened, and 9 met the eligibility criteria. They included two guidelines from the United States that addressed screening for latent tuberculosis infection in immigrants,5,6 three articles that addressed tuberculosis screening issues in foreign-born patients,7–9 one review of postlanding surveillance in Canada,10 and three narrative reviews of screening immigrants and refugees that recommended screening for latent tuberculosis infection in immigrants and refugees, but none used a systematic review method.11–13
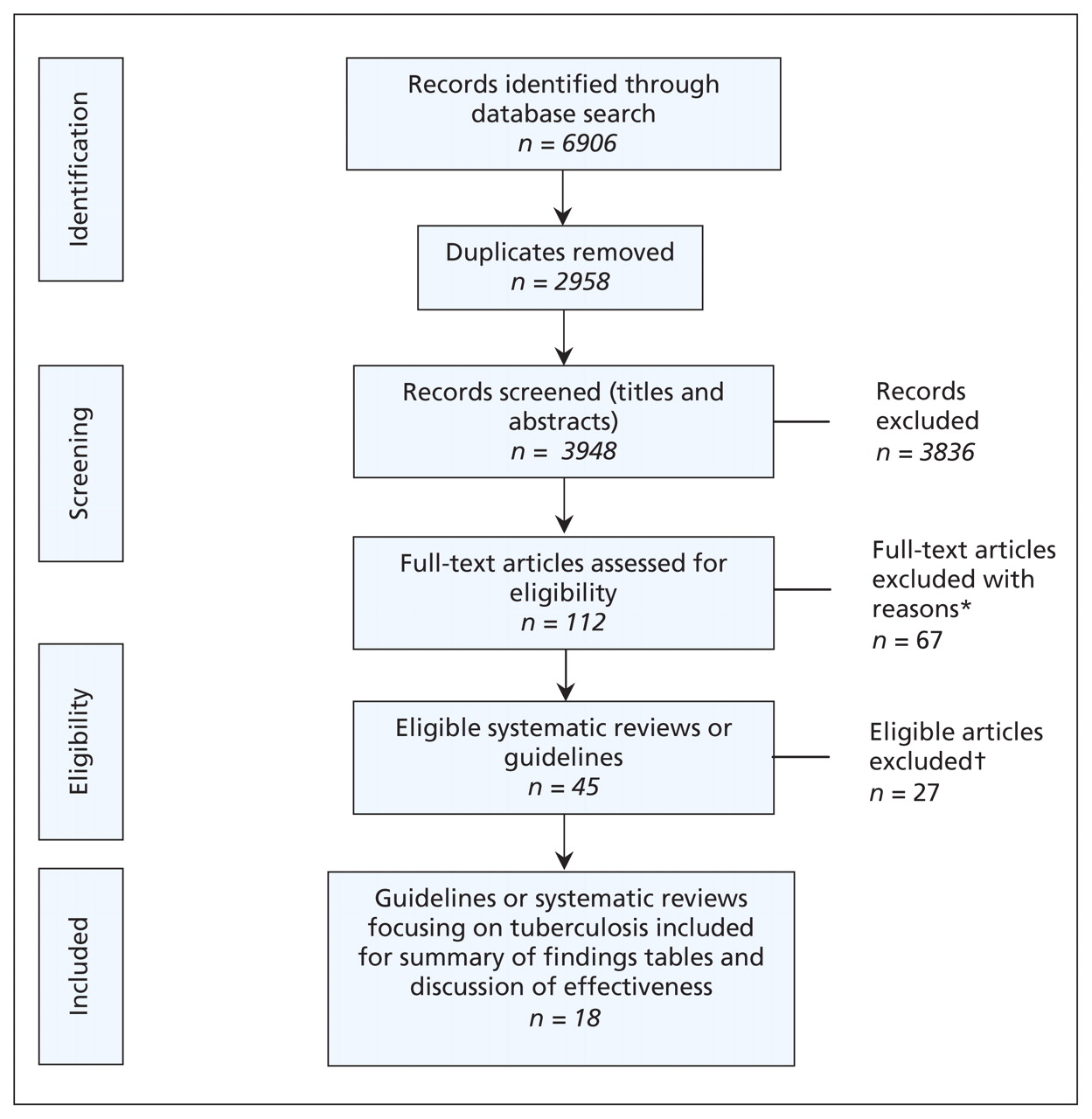
In the search for systematic reviews and guidelines for research involving the general population and tuberculosis, 3968 articles were identified, and 18 met the eligibility criteria. These reviews addressed diagnostic tests for latent tuberculosis infection,14,15 the effect of bacille Calmette-Guérin (BCG) on the tuberculin skin test,16–18 screening,7,19,20 factors that increase the risk of active tuberculosis,21–23 efficacy of treatment for latent tuberculosis infection24 and adherence to treatment,25 and included four US guidelines on controlling tuberculosis and treating latent tuberculosis infection.6,26–28 A flow chart of these combined searches is outlined in Figure 1. We identified the Canadian tuberculosis standards in the Web-based search.2 In the immigrant and tuberculosis search, 3073 primary articles were identified, of which 609 were relevant and addressed the following areas: epidemiology, diagnosis, screening, adherence and treatment for latent tuberculosis infection in immigrants.

Literature search for systematic reviews and guidelines on tuberculosis.
*Excluded because of lack of relevance. †Excluded because of lack of relevance, poor quality or outdated findings.
What is the burden of tuberculosis in immigrant populations?
Tuberculosis is an important global health burden, with more than one billion people infected with latent tuberculosis resulting in 9.2 million new active cases and 1.5 million deaths per year (> 95% occur in low- to middle-income countries).29 Canada is a low-incidence country, with an overall rate of active tuberculosis of 5 cases/100 000 population.3,30,31 Most of these cases (> 65%) occur in foreign-born patients, who have an incidence of tuberculosis 20 times that in the non-Aboriginal Canadian-born population (16 v. 0.8 cases/100 000 population) but with rates as high as 500 times those in certain subgroups of immigrants (Table 1).8,32,33 In the past 40 years, most new immigrants have originated from high-incidence countries (i.e., > 15 cases of smear-positive pulmonary tuberculosis/100 000 population), 30%–50% of whom are infected with latent tuberculosis, resulting in a reservoir of approximately 1.5 million people in Canada with latent tuberculosis infection who are at risk of active tuberculosis.2
Incidence of tuberculosis/100 000 population for immigrants and refugees after arrival in high-income countries
The prevalence of latent tuberculosis infection and the presence of factors associated with increased risk of active tuberculosis determine the people in whom active tuberculosis will develop. People with positive results of tuberculin skin tests who live in a low-incidence country and have no risk factors have an estimated annual probability of active tuberculosis developing of only 0.1% per year. This means that active disease will develop in only 5%–10% of those with latent tuberculosis infection.21 Recent transmission of tuberculosis confers an increased risk of active tuberculosis. This is extrapolated from studies in which 1%–2% of contacts have active tuberculosis immediately after diagnosis of the index cases. The highest risk of active tuberculosis occurs in the first year after exposure and decreases to the baseline risk (0.1% per year) 5 to 10 years after exposure.2,23
The strongest predictors for active tuberculosis in immigrant populations are global region of origin, immigration category, the presence of underlying medical comorbidity and the time since arrival.
Region of origin
Rates of tuberculosis are highest in immigrant populations that originate from world regions with the highest rates of tuberculosis, such as sub-Saharan Africa and Asia. Immigrants from these regions (rates of smear-positive pulmonary tuberculosis of 200–300/100 000 population) are more likely to be heavily exposed to tuberculosis, to have positive results of tuberculin skin tests and to have recently been exposed to tuberculosis.29
Immigration category
The risk of active tuberculosis in refugee populations is about double that in immigrant populations (Table 1).34–37 This is likely due to both a higher prevalence of latent tuberculosis infection and having lived in crowded conditions that increase the likelihood of recent exposure to tuberculosis.38
Presence of underlying comorbidity
Underlying medical illnesses, especially any conditions that decrease local or systemic immunity, increase the rate of active tuberculosis to varying degrees, with HIV being the strongest risk factor. The issue of HIV screening in new immigrants and refugees is discussed in the HIV evidence review in this series.
Time since arrival
Rates of tuberculosis in immigrant and refugee populations, from all world regions, are highest within the first five years after arrival in a low-incidence region but decrease dramatically after the first year of arrival. Rates of active tuberculosis in the immigrant population, as compared with five years after arrival, are 5 to 10 times greater in the first year and two-fold greater one to four years after arrival (Table 1).8,32,33 This increase is most likely caused by the effect of recent exposure to tuberculosis before arrival.39 A practical Web-based tool can be used to help calculate the lifetime risk of active tuberculosis based on these factors (www.tstin3d.com/index.html)40 (Tables 1 and 2).41–80
Relative risk of developing active tuberculosis in the presence of underlying medical conditions
Do screening and treatment for latent tuberculosis decrease morbidity from active tuberculosis?
Screening tests
The tuberculin skin test and interferon gamma release assays (IGRAs) are available for diagnosing latent tuberculosis infection. The sensitivity of these tests is estimated to be 70%–90%, and the specificity for all tests is > 95% except for the tuberculin skin test in patients vaccinated with BCG (60%) owing to cross-reactivity.15 With tuberculin skin tests, the likelihood of a false-positive result caused by BCG decreases with time since vaccination, but it also depends on the age when the person was vaccinated. In the first 10 years after vaccination, up to 42% of patients vaccinated after age two will have positive results of tuberculin skin tests (even fewer of patients vaccinated as neonates), but data on the rate of decline conflict.17,81–84 In those receiving a tuberculin skin test more than 10 years after vaccination as a neonate, only 1%–2% of results will be positive, compared with 21% in those vaccinated after age two. Interpreting results of a tuberculin skin test is therefore particularly difficult in children less than 10 years of age. All HIV-positive patients should be screened for latent tuberculosis infection with a tuberculin skin test.2
Because there is no criterion standard for the diagnosis of latent tuberculosis infection, assessing and comparing the performance of these tests is challenging, especially when there are discrepancies. The major advantage of the tuberculin skin test over IGRAs is that the risk of active disease for different sizes of induration in tuberculin skin testing is well described, whereas very few prospective data exist for IGRAs. The most recent Canadian guidelines recommend using the tuberculin skin test as the primary screening tool for both adults and children and using IGRAs sequentially after tuberculin skin test in people with a high likelihood of a false-positive result from tuberculin skin test (i.e., low risk of tuberculosis infection).85 This recommendation is supported by a recent cost-effectiveness analysis.86 The major limitation of these tests is their inability to distinguish the 10% of people with latent tuberculosis infection in whom active tuberculosis will develop from the 90% in whom it will not.
Once a tuberculin skin test has been performed and the results found to be positive, all patients should undergo chest radiography to rule out active tuberculosis and be questioned for symptoms of active tuberculosis (chronic cough, weight loss, fever, night sweats). If there is any suspicion of active tuberculosis, three samples of sputa or specimens from other sites (e.g., lymph node, cerebrospinal fluid) should be gathered for smear and culture before treatment for latent tuberculosis infection is started.
Relative benefits and harms of treatment
The efficacy of isoniazid compared with placebo in decreasing the likelihood of active tuberculosis developing in people with latent tuberculosis infection has been established in a Cochrane review (relative risk 0.40, 95% confidence interval 0.31–0.52) of 11 randomized controlled trials (Tables 3 and 4).24,87 The overall efficacy of isoniazid is 62% after 12 months of treatment but increases to 93% in those who adhere to treatment (i.e., take > 80% of their doses).88 Although a direct comparison of the efficacy of treatment for 9 versus 12 months has not been done, in a recent reanalysis, the maximal benefit of isoniazid was achieved at 9 months (Tables 5 and 6).89 A study on the effect of isoniazid resistance on efficacy of isoniazid chemoprophylaxis found that, at a mean prevalence of 7%–10% isoniazid resistance (the level in the immigrant population), isoniazid was the drug of choice and that only at very high rates (> 15%–20%) of isoniazid resistance were other regimens preferred.90,91
Summary of findings table on isoniazid to prevent active tuberculosis
Summary of findings for using isoniazid among all age groups with latent tuberculosis infection
Estimated numbers needed to treat for latent tuberculosis infection to prevent one case of active tuberculosis by age, time since arrival and adherence
Estimated numbers needed to treat for latent tuberculosis infection to prevent one case of active tuberculosis in those with high and intermediate risk for development of active tuberculosis by age, time of arrival and adherence
Hepatoxicity is a limitation of isoniazid therapy. It most commonly manifests as a transient asymptomatic increase in liver function (10%–20%), rarely causes clinical hepatitis (0.5%) — which resolves when treatment with isoniazid is stopped92,94,95 — and very rarely causes fulminant hepatitis and liver failure (< 0.01%) leading to death or liver transplantation.28,96–98 Initial higher overall rates of hepatotoxicity (1%) were reported among adults in the 1970s but were likely confounded by unrecognized underlying cirrhosis.99,100 Hepatoxicity among patients taking isoniazid is increased in those with pre-existing liver disease, alcoholism, concomitant use of hepatotoxic drugs and older age (Table 7). Although clinical and fulminant hepatitis are rare, they can occur at any age; this possibility underscores the importance of monthly monitoring for all patients and of teaching them to recognize symptoms of hepatitis (nausea, vomiting, abdominal pain, jaundice) and to stop medication as soon as worrisome symptoms occur.28,96 Adequate time must be taken, through interpreters if necessary, to ensure that all patients are appropriately informed and understand the risks and benefits of isoniazid, and they must be given a clear description of what to do if symptoms arise.
Estimated number needed to harm with increasing risk of isoniazid hepatoxicity
Clinical considerations
How are immigrants screened for tuberculosis before and after arrival to Canada?
All people applying for permanent residency, people claiming refugee status, and students and workers staying for more than six months are screened for active tuberculosis infection with chest radiography, followed by sputum culture if radiographic results are abnormal. Those found to have active tuberculosis must prove that they have been adequately treated and have negative results of culture before entry to Canada. Patients with previously treated tuberculosis or inactive tuberculosis (defined as those with latent tuberculosis infection and scarring visible on chest radiograph) are required to begin monitoring within 30 days after arrival in Canada in the Post-Landing Surveillance Program.2,10,20 There are no routine postlanding screening programs for latent tuberculosis infection for immigrants in Canada, but several programs exist (managed by different organizations) — for example, school-based screening, contact investigations, immigrant and refugee clinics, services for migrant workers and targeted screening of high-risk and undocumented migrants.106–123
Effectiveness of screening programs
The preimmigration radiographic screening and the Post-Landing Surveillance Program have relatively little effect on controlling tuberculosis in Canada. Of all immigrants screened for tuberculosis before immigration, less than 1% are found to have active tuberculosis, and 3%–5% (8000–13 000 people/yr) are found to have inactive tuberculosis.2,9 Despite forming a high-risk group for active tuberculosis, they account for only a small proportion of all cases of tuberculosis in the foreign-born population (8% in a study in Alberta), which could in part be due to program limitations.107,124–126
All the domestic screening programs (school-based, targeted immigrant or refugee, or contact tracing) for latent tuberculosis infection perform suboptimally; only about 47% (range 11%–72%) of people with positive results of tuberculin skin tests actually complete treatment.106,123 This suboptimal performance is caused by losses and dropouts at the many different steps in the process, including failure to present for or complete screening, failure to report for medical evaluation if screening test is positive, physicians’ failure to prescribe chemoprophylaxis for those eligible, patients’ refusal to start treatment and failure to complete a course of isoniazid.7 Suboptimal screening is compounded by the fact that there is a large pool of foreign-born patients with latent tuberculosis infection (30%–50% of all immigrants from countries in which tuberculosis is endemic) currently living in Canada or arriving in Canada each year. This pool includes not only one million people arriving annually from countries in which tuberculosis is endemic (visitors, students, temporary workers, etc.) but also the approximately four million people originating from countries in which tuberculosis is endemic who already live in Canada.127–129 Finally, exposure to tuberculosis caused by ongoing mobility of this population through travel to their countries of origin to visit family and friends could be substantial.130,131
What should be considered when screening and treating?
Children
Children less than 11 years of age do not undergo prearrival radiographic screening; for this and several other reasons, they could benefit greatly from screening for latent tuberculosis infection. There are many years of life in which active tuberculosis could develop in children, and children have a relatively low potential for hepatotoxicity (Table 7).99 If active tuberculosis develops, it is often difficult to diagnose because it is more often paucibacillary or extrapulmonary, and young children (especially those younger than five years of age) are more likely susceptible to severe or rapidly progressive disease.132,133
Refugees
Refugee populations have consistently had about a two-fold increased risk of active tuberculosis compared with the immigrant population, at least within the first year after arrival (Table 1).34–37 A higher prevalence of latent tuberculosis infection in the refugee population and having lived in crowded conditions that increase the likelihood of recent exposure to tuberculosis are contributing factors.38
What are potential implementation issues?
Barriers to uptake of screening and completion of treatment for latent tuberculosis infection include a combination of patient, provider and institutional factors. Patient barriers include the stigma of tuberculosis and its association with HIV, linguistic barriers and difficulties coming to appointments because of inconvenient clinic locations or limited clinic hours.121,134–136 Provider barriers to offering screening to migrants are related to inadequate knowledge of which migrants should be screened or how they should be followed up.137–139 Low adherence to treatment for latent tuberculosis infection is associated with barriers similar to those with screening latent tuberculosis. They include linguistic barriers, cultural taboos and stigmatization, low education level, perceived low risk of progressing from latent tuberculosis infection to active disease, belief that positive results from tuberculin skin tests are due to BCG, not wanting to have venipunctures, and economic factors (costs of travel, lack of insurance, delays in obtaining insurance, missed days at work).134,136,140–142
Increased adherence to tuberculin skin test screening has been seen with patient reminders (e.g., letters, phone calls), education of patients and physicians, and novel strategies, such as drive-by tuberculin skin test readings for taxi drivers.137,139,143 One study educating primary care providers on how and whom to screen for tuberculosis not only increased screening and identification of people with latent tuberculosis, but also increased identification of those with active tuberculosis. In this randomized clinical trial, screening was 0.4% and 57% in the nonintervention and intervention groups respectively, and identification of both those with latent tuberculosis infection (9% to 19%) and those with active tuberculosis (34% v. 47%) increased.137 Strategies that have increased adherence to treatment for latent tuberculosis infection in immigrant and refugee populations include patient reminders (calendar stickers for self-monitoring, phone calls, letters and directly observed therapy), adherence coaches who speak the same language as the patient, ongoing education of patients and providers, and cultural case management.25,144–146 Goldberg and colleagues found that when case managers were matched to the ethnic and linguistic background of patients and provided treatment for latent tuberculosis and monitoring during monthly home visits, adherence with treatment was substantially improved (82% v. 37%), as compared with standard clinic-based management before the intervention.146
Other recommendations
The Canadian Tuberculosis Committee, the Canadian Thoracic Society and the Canadian Paediatric Society recommend screening with a tuberculin skin test the following people from countries with high incidence of tuberculosis: children younger than 15 years living in Canada for less than two years, and people 15 years of age or older with factors that increase the risk of active tuberculosis or within two years after arrival if they have a known contact with tuberculosis (Table 2).2,147 The US Centers for Disease Control and Prevention, the Infectious Disease Society of America and the American Thoracic Society recommend screening for latent tuberculosis infection with a tuberculin skin test or an IGRA for all immigrants and refugees who have arrived in the US within the previous five years, regardless of age, but with priority screening for refugees flagged for postlanding surveillance and children less than 15 years of age.5,27,148
The cases revisited
Ousman and his daughter Nene should be screened for latent tuberculosis infection. Patients with positive results of tuberculin skin tests should be offered treatment if their risk of active tuberculosis outweighs the low risk of hepatotoxicity. Mariama should not be offered screening or treatment because, at her age, the risk of hepatotoxicity outweighs the benefit of treatment with isoniazid. Because the family speaks only Wolof, a translator must be used to ensure that family members understand the risks and benefits of isoniazid and know to stop treatment if symptoms of hepatitis arise.
Harjit likely had latent tuberculosis infection upon arrival to Canada and at that time had an approximately 6% lifetime risk of active tuberculosis. When diabetes developed, the risk increased 2- to 4-fold, and chronic renal failure with dialysis increased the risk 15-fold. Educating patients and practitioners to recognize subgroups that would benefit from targeted screening and treatment for latent tuberculosis infection will be essential to avoid missed opportunities for prevention.
Conclusions and research needs
The magnitude of human migration from regions with high to low incidence of tuberculosis has reached an unprecedented level. Control of tuberculosis in low-incidence settings will require novel strategies to ensure increased uptake of screening and completion of treatment for latent tuberculosis in the foreign-born population. These strategies will need to consider the challenges of accessing all foreign-born groups at risk of latent tuberculosis infection. Investment in tuberculosis education programs for patients and providers and in infrastructure is needed, so that screening and treatment programs for latent tuberculosis can be offered in a culturally sensitive manner with good access to translators. Consideration should be given to developing tuberculosis prevention programs in the context of comprehensive and integrated preventive health care in primary care, where a long-term trusting relationship can be established. Key future needs include new diagnostic tests to identify the few patients with latent tuberculosis infection in whom active tuberculosis will develop, and to develop well-tolerated, short-course treatment regimens for latent tuberculosis. Ultimately, the long-term solution will be to invest in global tuberculosis control to decrease the burden of tuberculosis in migrants to Canada.
Key points-
Foreign-born people account for 65% of all those with active tuberculosis in Canada, and subgroups have up to a 500-fold increased risk of active tuberculosis compared with the non-Aboriginal Canadian-born population.
-
The Canadian Collaboration for Immigrant and Refugee Health recommends screening certain groups as soon as possible on arrival in Canada with a tuberculin skin test and treating for latent tuberculosis infection in those found to be positive, after ruling out active tuberculosis.
-
Although isoniazid is highly efficacious in decreasing the development of active tuberculosis in those with latent tuberculosis infection, monitoring for hepatotoxicity is required for all ages; close monitoring is required for those over 50 years of age and those with pre-existing liver disease, alcoholism or concomitant use of hepatotoxic drugs.
-
Adherence to screening and treatment for latent tuberculosis infection can be increased if delivered in a culturally sensitive manner.
Clinical preventive guidelines for newly arrived immigrants and refugees to Canada
This article is part of a series of guidelines for primary care practitioners who work with immigrants and refugees. The series was developed by the Canadian Collaboration for Immigrant and Refugee Health.
Acknowledgements
The authors thank Peter Tugwell, John Feightner and Vivian Welch for their invaluable methodologic support throughout this project.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
-
Contributors: All authors contributed to conception and refinement of the study design and to analysis and interpretation of the data. Christina Greenaway drafted the initial manuscript, and all other authors provided critical revisions. All authors approved the final manuscript submitted for publication.
-
Funding: Christina Greenaway and Dick Menzies receive salary support from the Fonds de la Recherche en Santé du Québec through the Chercheur Boursier Clinicien and Chercheur National programs, respectively. The Canadian Collaboration for Immigrant and Refugee Health Steering Committee acknowledges the funding support of the Chronic Disease Branch of the Public Health Agency of Canada and Canadian Institutes of Health Research (Institute of Health Services and Policy Research), the Champlain Local Health Integrated Network and the Calgary Refugee Program. The views expressed in this report are the views of the authors and do not necessarily reflect those of the funders.
REFERENCES
In this issue

{kind=link}
Article tools



Jump to section
- Article
- Abstract
- The cases
- Introduction
- Methods
- Results
- What is the burden of tuberculosis in immigrant populations?
- Do screening and treatment for latent tuberculosis decrease morbidity from active tuberculosis?
- Clinical considerations
- Other recommendations
- The cases revisited
- Conclusions and research needs
- Acknowledgements
- Footnotes
- REFERENCES
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- Usefulness and practicality of a multidisease screening programme targeting migrant patients in primary care in Spain: a qualitative study of general practitioners
- Better data to drive more effective care for people with latent tuberculosis infection in Canada
- Demographic predictors of active tuberculosis in people migrating to British Columbia, Canada: a retrospective cohort study
- Diagnosis and management of pediatric tuberculosis in Canada
- Predicting tuberculosis risk in the foreign-born population of British Columbia, Canada: study protocol for a retrospective population-based cohort study
- Domestic impact of tuberculosis screening among new immigrants to Ontario, Canada
- An unusual case of appendicitis
- Screening immigrants for latent tuberculosis: Do we have the resources?
More in this TOC Section
Similar Articles
Collections

