


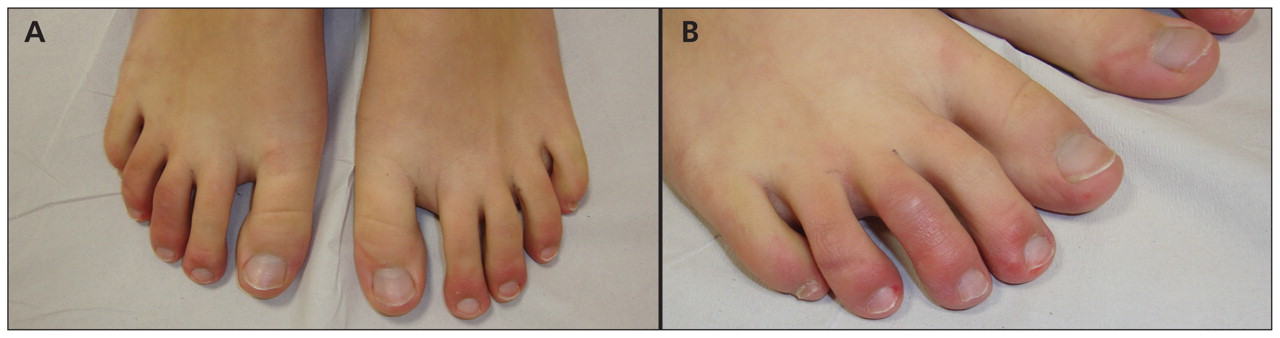
A 26-year-old woman presented with a three-year history of painful and itching skin lesions on both feet that worsened during the winter and improved during the summer (Figure 1). She was otherwise well and did not report any constitutional symptoms. Based on the relation of cold temperature to her skin lesions, we considered a diagnosis of chilblains. Results of laboratory analyses including a complete blood count, antinuclear antibodies, cryoglobulins, cryofibrinogen, cold agglutinins, antiphospholipid antibodies and serum protein electrophoresis were normal.

(A) Feet of a 26-year-old woman showing erythematous and violaceous papules and nodules over the distal portion of her toes. The lesions were cold and painful on palpation. (B) Detail showing erythema.
We prescribed topical mometasone, and after two weeks, our patient’s lesions had improved considerably. We suggested that she avoid exposure to cold as much as possible, using warm socks and gloves during the winter months. At her routine follow-up visit a year later, there had been no recurrence.
Chilblains, also called perniosis, are an inflammatory skin condition related to an abnormal vascular response to the cold. We are unaware of a reliable estimate of incidence. It typically presents as tender, pruritic red or bluish lesions located symmetrically on the dorsal aspect of the fingers, toes, ears and nose. Less commonly, reports describe involvement of the thighs and buttocks.1 The lesions present 12–24 hours after exposure to cold and usually resolve spontaneously in one to three weeks. Although more than half of published cases are idiopathic, a recent review suggests that up to 20%–40% of chilblains may be associated with more concerning conditions including systemic lupus erythematosus, cryoglobulinemia, antiphospholipid syndrome, macroglobulinemia and chronic myelomonocytic leukemia.2 This estimate is, however, prone to reporting bias and needs to be interpreted with caution.
Because it remains a diagnosis of exclusion, a minimal workup for chilblains includes a complete blood count, antiphospholipid antibody panel, cryoglobulins, cryofibrinogen, cold agglutinins, antinuclear antibodies and serum protein electrophoresis.1,2 In treatment-resistant or chronic chilblains, further testing, including a biopsy, may be indicated to rule out other inflammatory processes. Histology usually shows intense papillary dermal edema, superficial and deep perivascular lymphocytic infiltrates and edema of vessel walls.1 Prevention of idiopathic chilblains is based primarily on avoidance of cold.3 Case reports point to successful symptomatic management of idiopathic chilblains with potent topical steroids and, in the most severe instances, prevention with the calcium channel blocker nifedipine.4,5
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

