


Abstract
Background: Understanding the health care experience of people with dementia and their caregivers is becoming increasingly important given the growing number of affected individuals. We conducted a systematic review of qualitative studies that examined aspects of the health care experience of people with dementia and their caregivers to better understand ways to improve care for this population.
Methods: We searched the electronic databases MEDLINE, Embase, PsychINFO and CINAHL to identify relevant articles. We extracted key study characteristics and methods from the included studies. We also extracted direct quotes from the primary studies, along with the interpretations provided by authors of the studies. We used meta-ethnography to synthesize the extracted information into an overall framework. We evaluated the quality of the primary studies using the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.
Results: In total, 46 studies met our inclusion criteria; these involved 1866 people with dementia and their caregivers. We identified 5 major themes: seeking a diagnosis; accessing supports and services; addressing information needs; disease management; and communication and attitudes of health care providers. We conceptualized the health care experience as progressing through phases of seeking understanding and information, identifying the problem, role transitions following diagnosis and living with change.
Interpretation: The health care experience of people with dementia and their caregivers is a complex and dynamic process, which could be improved for many people. Understanding these experiences provides insight into potential gaps in existing health services. Modifying existing services or implementing new models of care to address these gaps may lead to improved outcomes for people with dementia and their caregivers.
See also editorial by Flegel at www.cmaj.ca/lookup/doi/10.1503/cmaj.131296
The global prevalence of Alzheimer disease and related dementias is estimated to be 36 million people and is expected to double in the next 20 years.1 Several recent strategies for providing care to patients with dementia have highlighted the importance of coordinated health care services for this growing population.2–5 Gaps in the quality of care for people with dementia have been identified,6–8 and improving their quality of care and health care experience has been identified as a priority area.2–5
Incorporating the health care experience of patients and caregivers in health service planning is important to ensure that their needs are met and that person-centred care is provided.9 The health care experience of people with dementia and their caregivers provides valuable information about preferences for services and service delivery.10 Matching available services to patient treatment preferences leads to improved patient outcomes11,12 and satisfaction without increasing costs.13 Qualitative research is ideally suited to exploring the experiences and perspectives of patients and caregivers and has been used to examine these experiences for other conditions.14 We performed a systematic review and meta-ethnographic synthesis of qualitative studies exploring the health care experience of people with dementia and their caregivers in primary care settings, and we propose a conceptual framework for understanding and improving these health care experiences.
Methods
Literature search
We searched MEDLINE, Embase, PsycINFO, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) from inception up to August 2011 using medical subject headings and free text terms (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.121795/-/DC1). We also searched the journals Qualitative Research and Qualitative Health Research. Two authors (J.C.P. and D.P.S.) evaluated the titles and abstracts of the citations to identify potentially relevant studies. The flow of studies through the review process was recorded using standard review guidelines.15
Selection criteria
We included qualitative studies that used either interviews or focus groups to examine the health care experience of people with dementia (as defined by standard criteria) or their caregivers in primary care. We defined care-givers as informal caregivers (e.g., friends or family members). We also included studies that used both qualitative and quantitative methods (i.e., mixed methods studies) within the same study. For these studies, we only included the qualitative data that met our inclusion criteria. We included only studies published in English because of concerns about translating qualitative data.16,17 We also only included studies that described the primary research question, context of the research, study sample and methods used for data collection and analysis. We excluded studies that did not provide information from primary care or that provided only data about the experiences of health care providers.
Quality of studies
We assessed the quality of reporting of included studies using the Consolidated Criteria for Reporting Qualitative Research (COREQ).18 The presence or absence of reporting of each of the 32 items on the COREQ checklist was assessed in duplicate by 2 authors (J.C.P. and D.P.S.) for 20 studies. Because there was a substantial degree of interrater agreement for each COREQ item (average Kappa value > 0.7), the remaining studies were assessed by 1 author (J.C.P.). This method has been used in published systematic reviews of qualitative research.19,20
Data extraction
Information from included studies was extracted by 2 authors (J.C.P. and D.P.S.) and included the following data: country in which the study was performed; number and type of study participants (people with dementia, caregivers or both); study design (interviews or focus groups); principal experiences explored; and the theoretical framework (e.g., grounded theory).
We reviewed the studies in chronological order, and data were extracted until saturation was reached.
Meta-ethnography
We used the qualitative synthesis method meta-ethnography to extract information and synthesize the literature.19,21 Meta-ethnography produces a systematic review that is interpretative, rather than aggregative.22
In a meta-ethnographic analysis, information is categorized as a first-, second- or third-order construct. We first reviewed each primary study and extracted relevant direct quotations (i.e., first-order constructs). The interpretations of the data by the primary study authors were then extracted as second-order constructs. We then used meta-ethnography to synthesize the second-order constructs into third-order constructs, which formed our interpretations of the overarching themes arising from the primary studies. Key themes across studies were derived from the first- and second-order constructs.
The research team met throughout the review process to analyze and discuss the available first-and second-order constructs, resulting in continuous development and refinement of third-order constructs. These constructs were interpreted and organized into an overall health care experience framework.
Results
Selection of studies
Our electronic database search identified 3399 citations (Figure 1). Of these, we included 46 studies in the final review (Table 1).23–68 These studies included 7 studies involving people with dementia, 25 studies involving caregivers, and 14 studies that involved both groups. Thirty studies used interviews, 10 used focus groups, and 6 used both methods. Most of the included studies presented only qualitative data, but a few studies reported both qualitative and quantitative data.25,26,55 Most studies were conducted in the United Kingdom, United States, Canada or Australia. The total sample size of the studies was 1866, with a mean sample size of 41 participants.

Flow of studies through the analysis.
Study quality
The quality of information reported in the included studies varied (Table 2). The number of items reported on the COREQ checklist ranged from 3 items35 to 25 items63,64 (out of 32 items); the mean was 15 items. All but 1 of the studies reported consistent data and findings58 and clarity of major themes.35 Most studies included participant quotations, sampling methods, methods of approach and sample size. Few studies reported interviewer characteristics and participant knowledge of the interviewer, and none reported whether a relationship with the participants was established before the study.
Health care experiences
We identified 5 major themes and several sub-themes from the primary and secondary constructs. These themes included seeking a diagnosis; accessing supports and services; addressing information needs; disease management; and communication and attitudes of health care providers. Illustrative first- and second-order constructs are summarized in Table 3.
Seeking a diagnosis
The theme “seeking a diagnosis” addresses the early stages experienced by people with dementia and their caregivers. Throughout this process, the timeliness of diagnosis was found to be important. Earlier diagnosis led to easier subsequent transitions. Many people with dementia and their caregivers expressed frustration, uncertainty and disorganization throughout the diagnostic process. The reaction to the diagnosis ranged from shock when dementia was not suspected to relief when dementia was suspected.
Accessing supports and services
The theme “accessing supports and services” describe the experiences of people with dementia and caregivers when seeking assistance from medical and community services. Patients and their caregivers often felt that the path to finding assistance was unnecessarily prolonged. They perceived a lack of knowledge and support by primary care providers about these services, and they consequently experienced difficulty in obtaining help. Specialist services, such as memory clinics, were generally regarded positively, although delays in accessing these services were common. People with dementia and their caregivers stressed the importance of supports or services congruent with their current needs and care goals.
Addressing information needs
The theme “addressing information needs” encompasses how information is delivered and the quantity and content of information. Caregivers and people with dementia often expressed having to “push” to obtain information. They appreciated when information was provided in a clear fashion and when written information was provided. However, although receiving information was appreciated, it was important that the quantity was not overwhelming. Both people with dementia and their caregivers frequently requested information about cognitive testing, medications, disease progression, finances and behaviour.
Disease management
We found that the knowledge of health care providers was a significant factor in the perceived effectiveness of disease management. Patients and caregivers preferred that their physicians be knowledgeable about dementia and its management. Although initiating management is thought of as the responsibility of the health care provider, many caregivers reported that they needed to approach the providers to initiate certain aspects of management. At times people with dementia or their caregivers had to initiate discussions about medications and other concerns (e.g., driving safety).
Communication and attitudes
The theme “communication and attitudes” was important at every stage of the health care experience for patients and caregivers. Valuing the perspectives of people with dementia and their caregivers was viewed as important, and both groups were dissatisfied when they felt discounted. They appreciated when health care providers displayed sensitivity and validation of feelings, as well as treated them with dignity and respect. Poor communication and attitudes led to frustration and could be seen as barriers to treatment. Conversely, good communication and attitudes put patients at ease and facilitated open and compassionate interactions.
Interpretation
We found an extensive body of qualitative research literature examining various aspects of the health care experience of people with dementia and their caregivers. Although the individual studies were conducted in a range of settings, we found similar themes between studies, suggesting that there are certain experiences shared by people with dementia. Both positive and negative experiences were reported in the included studies, although areas of dissatisfaction predominated the literature, highlighting several areas for the improvement of health care services and supports.
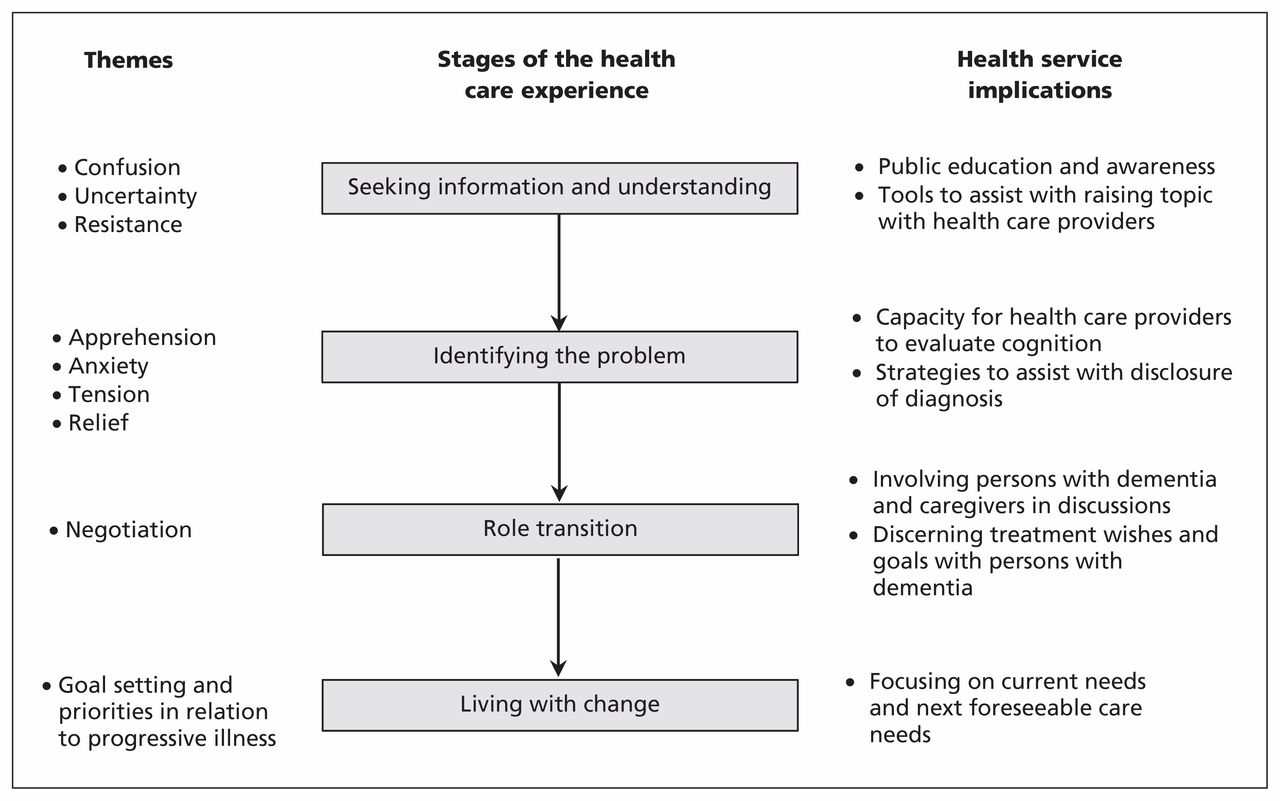
The overall health care experience of people with dementia and their caregivers can be conceptualized as progressing through several phases, each with unique challenges and opportunities for health care providers (Figure 2). The phases of this health care experience are seeking understanding and information; identifying the problem (diagnosis); role transitions following diagnosis; and living with the changes associated with this disease.

Conceptual framework for the health care experience of people with dementia and their caregivers.
The initial stages of this experience are characterized by a need to seek information and understanding when cognitive changes are noticed by people with dementia or their caregivers. Challenges during this phase included an overall lack of information about dementia in society,69 associated social stigma70 and difficulty on the part of the person with dementia in communicating their symptoms.71 Often this phase is experienced as an extended period of uncertainty and distress. A formal diagnosis of dementia signifies a new stage in the health care experience. Identifying the problem can bring about a mixture of anxiety and relief. Relief may result from finally determining the cause of cognitive and behavioural changes and potentially confirming suspicions. People with dementia and their caregivers may also fear the inevitable progression of the disease. Following diagnosis, the roles assumed by the person with dementia, caregivers and health care providers become more formalized as each begins to prepare to cope with the illness over the long-term. It is important that the patient, caregiver and physician are supported in these new roles. Living with change is often characterized by continuous lifestyle adjustments that allow home and community living. Both people with dementia and their caregivers need practical advice on how to manage everyday life during this time.
Comparison with other studies
Our study is consistent with other recently published syntheses of studies exploring the experience of people with dementia during the process of diagnostic disclosure,72 the experiences of caregivers of people with cognitive impairment,73 and the experiences of health care providers in caring for patients with dementia.73 Together, these studies and our review suggest that the health care experience of patients and caregivers is less than optimal and that several areas of this experience could be improved. Similar findings have also been identified in other patient populations.19,20,74
There are several implications of our findings for health service delivery that may improve the health care experience of patients and caregivers throughout these stages. Given that most of the care for patients with dementia can be provided in primary care settings75 and the limited access to geriatric specialist services,76 there are several ways that primary care providers may be able to improve the care provided to patients with dementia and their caregivers. First, improving communication and attitudes around dementia were identified as important to patients and caregivers, and primary care providers should be aware of person-centred approaches to care.77 Additional education about dementia and its management may help provide health care providers with these skills.73,74,76,78,79
There are several specific changes to dementia care that may improve the health care experience of patients and their caregivers. Outreach and public education strategies can be successful in raising awareness of dementia and helping people identify cognitive changes sooner in order to bring these changes to the attention of primary care providers earlier.80,81 The introduction of screening programs for people at risk of dementia may aid in the early detection in primary care or community settings,82,83 but this requires further study. Education and interventions to equip people with self-management skills and resources have been shown to improve outcomes for a variety of chronic diseases in primary care, and these strategies may also be of benefit in coping with dementia.84 The introduction of services, such as dementia care managers, in primary care teams are promising ways to assist providers in improving the quality of dementia care and behavioural management strategies.85 Psychoeducation for caregivers, including information about dementia and management strategies in primary care or through facilitating linkages to community agencies (e.g., Alzheimer societies66) have been shown to have a major effect on caregiver burden and depression86 and delayed admission to a long-term care facility.87,88 Many of these strategies may be beneficial across the stages of the dementia experience, although some strategies may be more relevant during certain stages. Efforts to improve access to these services and strengthen the quality of dementia care in primary care may facilitate a more positive health care experience.
Strengths and limitations
The strengths of our study include the systematic method (meta-ethnography) used to identify and synthesize studies.89 Meta-ethnography added more depth than a typical systematic review by providing additional analysis and generation of comprehensive frameworks.89,90 We also evaluated the quality of studies using standard criteria previously used in meta-ethnographic studies.19,20
Although there is debate about the appropriateness of synthesizing qualitative information from different theoretical frameworks,90 we sought to provide a comprehensive understanding of the health care experience by including as many relevant articles as possible in our review. Moreover, there are other examples of published meta-ethnographic studies that have been synthesized across theoretical frameworks to create overarching syntheses.19,20 The quality of reporting of the included studies varied, and some studies may provide more accurate reflections of this health care experience than others.
Conclusion
We found several opportunities to improve the health care experiences of people with dementia and their caregivers. Many of the strategies we suggest for improving service delivery are in keeping with the emphasis on enhancing person-centred care. Through understanding and improving health care experiences, we hope that quality of life and other outcomes will be improved for people with dementia.
Characteristics of the included studies
Quality of reporting in the 46 included studies according to Consolidated Criteria for Reporting Qualitative Research (COREQ) criteria
Themes derived from studies included in the review
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Jeanette Prorok and Dallas Seitz designed the study, with contributions from Salinda Horgan. Jeanette Prorok and Dallas Seitz performed the systematic review. All of the authors participated in the synthesis of data. Jeanette Prorok wrote the manuscript, which was revised for important intellectual content by all authors. All of the authors approved the final version of the manuscript submitted for publication.
Funding: Funding for this project was provided through a Knowledge-to-Action grant (no. 114493) from the Canadian Institutes of Health Research. The study sponsors had no role in the design of the study, collection, analysis or interpretation of data, the writing of the report or the decision to submit the article for publication.
References
In this issue

{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- 'Ive never been so stressed in my life: a qualitative analysis of young adults lived experience amidst pandemic restrictions in Prince Edward Island, Canada
- Methods for the involvement of people living with dementia in research focused on the built environment: a protocol for a scoping review
- Effectiveness-implementation hybrid type 2 study evaluating an intervention to support 'information work in dementia care: an implementation study protocol
- Care of community-dwelling older adults with dementia and their caregivers
- Lexperience dune patiente qui recoit des soins pour la demence: Utiliser << lexperience vecue >> pour ameliorer les soins
- A patients experience in dementia care: Using the "lived experience" to improve care
- Medication-related burden and patients lived experience with medicine: a systematic review and metasynthesis of qualitative studies
More in this TOC Section
Similar Articles
Collections

