


Abstract
Background: Frailty is a multidimensional syndrome characterized by loss of physiologic and cognitive reserves that confers vulnerability to adverse outcomes. We determined the prevalence, correlates and outcomes associated with frailty among adults admitted to intensive care.
Methods: We prospectively enrolled 421 critically ill adults aged 50 or more at 6 hospitals across the province of Alberta. The primary exposure was frailty, defined by a score greater than 4 on the Clinical Frailty Scale. The primary outcome measure was in-hospital mortality. Secondary outcome measures included adverse events, 1-year mortality and quality of life.
Results: The prevalence of frailty was 32.8% (95% confidence interval [CI] 28.3%–37.5%). Frail patients were older, were more likely to be female, and had more comorbidities and greater functional dependence than those who were not frail. In-hospital mortality was higher among frail patients than among non-frail patients (32% v. 16%; adjusted odds ratio [OR] 1.81, 95% CI 1.09–3.01) and remained higher at 1 year (48% v. 25%; adjusted hazard ratio 1.82, 95% CI 1.28–2.60). Major adverse events were more common among frail patients (39% v. 29%; OR 1.54, 95% CI 1.01–2.37). Compared with nonfrail survivors, frail survivors were more likely to become functionally dependent (71% v. 52%; OR 2.25, 95% CI 1.03–4.89), had significantly lower quality of life and were more often readmitted to hospital (56% v. 39%; OR 1.98, 95% CI 1.22–3.23) in the 12 months following enrolment.
Interpretation: Frailty was common among critically ill adults aged 50 and older and identified a population at increased risk of adverse events, morbidity and mortality. Diagnosis of frailty could improve prognostication and identify a vulnerable population that might benefit from follow-up and intervention.
Frailty is a term widely used to describe a multidimensional syndrome characterized by the loss of physiologic and cognitive reserves that gives rise to heightened vulnerability to adverse outcomes.1,2 Adverse events associated with frailty include incident falls, susceptibility to acute illness, perioperative complications, unplanned hospital admissions, disability, need for institutional care, and death.3–10 Frailty has substantial implications for quality of life, functional autonomy and health services utilization, but it has not been evaluated in critically ill patients.
The development of critical illness may lead to frailty in vulnerable patients. Critical illness may also be a key factor impeding recovery and functional autonomy in those already considered to be frail.11 We hypothesized that frailty would identify vulnerable patients who are less likely to tolerate critical illness, who are more susceptible to complications and death, and who are less likely to fully recover after critical illness over the short or long term. We further hypothesized that this information would translate into more accurate prognostication, which might improve decision-making for frail patients and their families. To test these hypotheses, we performed a prospective multicentre study in an unselected cohort of critically ill patients.
Methods
Study design and population
This was a multicentre prospective cohort study. The study population comprised adults admitted to 1 of 6 participating intensive care units (ICUs) between Feb. 1, 2010, and July 31, 2011. The ICUs were located in 2 tertiary care academic hospitals and 4 community hospitals in the province of Alberta (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130639/-/DC1). These hospitals were selected to represent the province and capture academic and community settings to minimize selection bias.
Patients were included if they were aged 50 years or more (based on the low prevalence of frailty among younger patients12), were admitted to a participating ICU and were able to provide consent. Patients were excluded if their expected ICU stay or survival was less than 24 hours or if they had previously been enrolled in the study. Consecutive participants were identified by daily screening of new ICU admissions.
All participants or their surrogates provided informed consent. The study was approved by the Health Research Ethics Board at the University of Alberta and the Conjoint Health Research Ethics Board at the University of Calgary.
Determination of frailty
Frailty was defined with the use of the Canadian Study on Health and Aging Clinical Frailty Scale, a well-validated 9-point assessment tool designed to quantify frailty (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130639/-/DC1).3 Trained research coordinators masked to the study hypotheses determined the Clinical Frailty Scale scores by interviewing participants or surrogates and reviewing each participant’s medical record. We considered patients to be frail if they had a score greater than 4 (which represents mild, moderate, severe or very severe frailty3) immediately before the index hospital admission.
Outcome measures
The primary outcome measure was all-cause in-hospital mortality. Secondary outcome measures included the following: death in ICU, hospital or at 6 months; health-related quality of life at 6 and 12 months (as measured by the 12-item Short-Form Health Survey [SF-12]13 and the EuroQol Health Questionnaire [EQ-5D]);14 intensity of treatment in the ICU (as determined by whether vasoactive therapy, mechanical ventilation, renal replacement therapy or blood transfusion was provided); major adverse events (defined as a composite of serious medication errors, self-extubation or re-intubation, or nosocomial infection [e.g., catheter-related bloodstream infection] during the hospital stay); and health services utilization (as measured by durations of stay in ICU and hospital as well as readmission to hospital within 12 months after enrolment).
Other covariables
At enrolment, the trained research coordinators collected information through interviews with the participants (or surrogates) and chart reviews. The collected data included age, sex, race/ethnicity, education level, marital status, ability to perform instrumental and functional activities of daily living, comorbid conditions and degree of comorbidity (e.g., defined according to Elixhauser score15,16), number of prescription medications,17 number of hospital and ICU admissions in the year before enrolment, source of transfer to ICU (e.g., ward, emergency department, other hospital, operating theatre), illness severity (e.g., defined according to Acute Physiology and Chronic Health Evaluation [APACHE] II score18), and presence and severity of organ dysfunction (e.g., defined according to Sequential Organ Failure Assessment [SOFA] score19). In addition, the research coordinators determined whether limitations in the provision of ICU-specific, life-sustaining therapy (e.g., cardiopulmonary resuscitation, advanced cardiac life support, mechanical ventilation, use of vasoactives and renal replacement therapy) were documented in the medical record.
The research coordinators contacted surviving participants by telephone at 6 and 12 months after enrolment to determine vital status, disposition and health-related quality of life using a scripted text.20,21
Data were captured on standardized case report forms and entered into an electronic database.
Statistical analysis
Based on data from a pilot study involving 50 patients, we expected a prevalence of frailty of 30% (unpublished data). To confirm this magnitude of prevalence within 5% binomial confidence limits, we required a sample of at least 400 participants. With an anticipated 1-year mortality of 40% (160 events), this sample size would permit up to 16 covariates in multivariable models of 1-year mortality with a 2-tailed α value of 0.05 and would have at least 80% power to detect 15% differences between frail and nonfrail participants.
Descriptive statistics according to frailty status were tabulated, and univariable comparisons of means, medians and proportions were performed. Kaplan–Meier survival curves were constructed, and multivariable logistic regression (in-hospital mortality) and Cox regression (1-yr mortality) analyses were used to determine the association between frailty and mortality. The models were adjusted for potential confounding factors, which were included based on their clinical importance, evidence from the literature or their significance at p < 0.20 in the univariable analysis.
For the logistic regression analysis, model fit and calibration were assessed with the Hosmer–Lemeshow goodness-of-fit test and the C statistic. For the Cox regression analysis, time-dependent covariates and log(–log) plots were used to test for violations of the proportional hazards assumptions; no violations were observed. Analogous analyses were undertaken for the other study outcomes.
Using the Student t test, we compared participants’ health-related quality-of-life measures at 6 and 12 months against normative SF-12 and EQ-5D data for the general population in Alberta.22
A p value of less than 0.05 was considered statistically significant for all comparisons. All analyses were performed with the use of Stata 11.2 (StataCorp).
Results
A total of 421 patients were enrolled in our study (Figure 1). Their mean age (± standard deviation) was 67 ± 10 years; 163 (39%) were female, and 402 (95%) were living at home independently or with assistance. At the time of ICU admission, the mean APACHE II score was 20 ± 7, the SOFA score was 7 ± 4, and 142 (34%) of the participants had had surgery within 48 hours before the admission. There were no clinically important or statistically significant differences in baseline sociodemographic characteristics or illness severity between enrolled participants and patients who were eligible but were not enrolled (Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.130639/-/DC1).

Selection of critically ill patients for the study cohort.
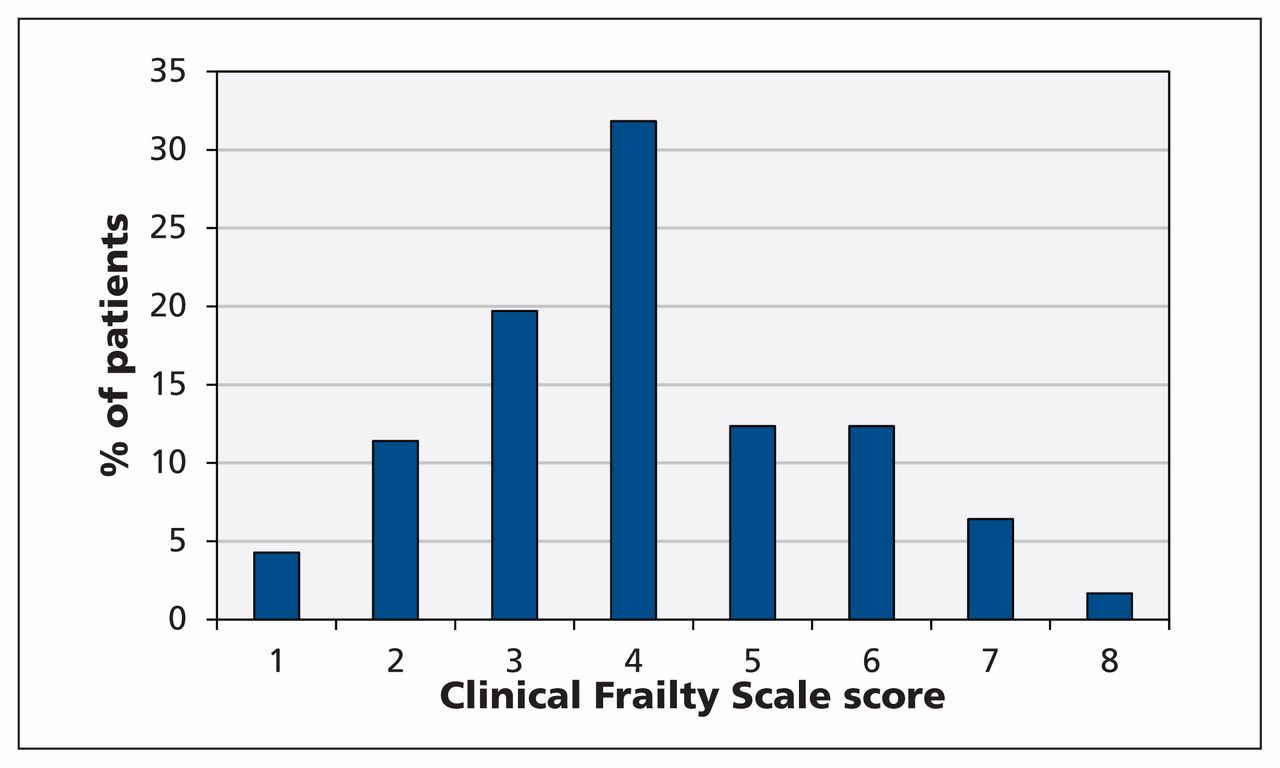
Overall, 138 of the 421 participants were considered to be frail (Clinical Frailty Scale score > 4), for a frailty prevalence of 32.8% (95% confidence interval [CI] 28.3%–37.5%). The median frailty score was 4 (interquartile range 3–5) (Figure 2). Compared with nonfrail patients, frail patients were older, were more likely to be female, had more comorbid disease and greater functional dependence, and tended to have fewer social supports (Table 1).

Distribution of Clinical Frailty Scale scores and prevalence of frailty (score > 4) among the participants.
Baseline characteristics of patients admitted to intensive care unit (ICU), by frailty status
Frail patients were more likely than nonfrail patients to be admitted for nonsurgical reasons and to have higher APACHE II scores, although baseline and daily SOFA scores were not significantly different between the two groups (Table 1). Irrespective of frailty, all patients received similar intensity of treatment (Table 2). Compared with nonfrail patients, those with frailty were more likely to have limitations of medical therapy at ICU admission (34% v. 12%; p < 0.001).
Treatment intensity and use of resources associated with admission to intensive care unit, by frailty status
Mortality during the ICU stay did not differ according to frailty, but in-hospital mortality was higher among frail patients (32% v. 16%; adjusted odds ratio [OR] 1.81, 95% CI 1.09–3.01) (Table 3). In the multivariable analysis, over the 12-month follow-up period, frailty was independently associated with all-cause mortality (48% v. 25%; adjusted hazard ratio [HR] 1.82; 95% CI 1.28–2.60). In a dose-dependent manner, an increasing frailty score (rather than the cutpoint of 4 used in the primary analysis) was independently associated with incremental mortality in adjusted analyses (Figures 3 and 4).
Clinical outcomes, by frailty status

Adjusted hazard ratios for death within 12 months after admission to an intensive care unit, stratified by Clinical Frailty Scale score (score > 4 indicates frailty). Hazard ratios greater than 1.0 indicate an increased risk of death. The models were adjusted as follows: model 1 for age and sex; model 2 for age, sex and Elixhauser score (comorbidity indicator); model 3 for age, sex, Elixhauser score and non–age-specific Acute Physiology and Chronic Health Evaluation (APACHE) II score (illness severity); model 4 for age, sex, Elixhauser score and Sequential Organ Failure Assessment (SOFA) score (presence and severity of organ dysfunction); and model 5 for age, sex, Elixhauser score, non–age-specific APACHE II score and hospital type (tertiary care/academic v. community). CI = confidence interval, ref = reference group.

Kaplan–Meier survival curves stratified by Clinical Frailty Scale score.
Among the survivors, frailty was associated with significantly longer durations of stay in both ICU and hospital (Table 3). Frail patients also had a 1.5-fold higher odds of major adverse events during their hospital stay compared with their nonfrail counterparts (OR 1.54, 95% CI 1.01–2.37). In the 12 months after hospital discharge, frail patients had a greater rate of hospital readmission than nonfrail patients had (56% v. 39%; OR 1.98, 95% CI 1.22–3.23).
After hospital discharge, frail patients were less likely than nonfrail patients to be living at home independently (22% v. 44%; OR 0.35, 95% CI 0.20–0.61) (Table 3). This difference persisted at 6 months (28% v. 61%; OR 0.25, 95% CI 0.14–0.43) and at 12 months (31% v. 67%; OR 0.22, 95% CI 0.12–0.40). Among survivors who were living independently at baseline, frail patients were more likely than nonfrail patients to become functionally dependent (71% v. 52%; OR 2.25, 95% CI 1.03–4.89) (Table 3). In a sensitivity analysis, this association was stronger when stratified by a baseline frailty score of more than 5 or of 3 or lower (78% v. 46%; OR 4.14, 95% CI 1.34–12.73). Health-related quality of life was generally lower among the frail patients than among the nonfrail patients at 6 and 12 months, and across all physical and mental health domains; however, both groups had lower health-related quality of life compared with the general population of Alberta22 (Table 4).
Summary of health-related quality of life
Interpretation
In this prospective multicentre study of a representative cohort of critically ill patients over the age of 50, we found that frailty was common, affecting one-third of the participants. Frail patients differed from nonfrail patients in many sociodemographic and clinical characteristics, including having a greater burden of comorbid illness and functional impairment at ICU admission. Despite both groups having similar treatment intensity, frail patients were more likely to experience adverse events, had longer lengths of stay in ICU and hospital, and were more likely to die while in hospital and within 12 months after admission. Among survivors, frail patients were more likely than nonfrail patients to have new functional dependence at hospital discharge and had higher rates of hospital readmission. There was a similar disadvantage for frail patients for worse health-related quality of life across all domains measured. These associations were stronger with increasing severity of frailty and persisted even after adjustment for sociodemographic factors, premorbid health status, comorbidities and illness severity.
Our data suggest that frailty can be measured in patients admitted to the ICU using a simple bedside assessment tool and is an important prognostic factor in both the short and long term.23 Similar to acute care hospital admission contributing to an increased likelihood of cognitive impairment, an episode of critical illness may have a sustained impact on the capacity for frail patients to recover and regain or maintain functional independence.24,25
In the context of critical illness, a degree of frailty seems to identify a vulnerable population whose risk of poor outcomes is heightened. This risk may be further exacerbated by frail patients having fewer social supports, as shown in our study. The interplay of frailty and critical illness may provide an opportunity to target and evaluate interdisciplinary programs of care and rehabilitation, with the aim of improving recovery and avoiding mortality, functional dependence, reduced quality of life and added health service utilization.23,26,27 For frail critically ill patients, such an integrated program may have elements addressing the minimization of unnecessary sedation,28 screening for delirium,29 early assessment for weaning from mechanical ventilation, nutritional support,30 medication reconciliation31 and early mobilization.32,33 In addition, the measurement and diagnosis of frailty could translate into better informed decision-making for patients, their families and clinicians around issues related to the provision of advanced life support and designation of goals of care.
Frailty is generally viewed as an age-associated loss of reserve across multiple physiologic and cognitive systems that give rise to susceptibility to adverse events.1,2 A variety of operational definitions have been applied to encapsulate the frail state across clinical contexts; however, none has been used to describe frailty among a generalizable cohort with critical illness.34 Similarly, other measures of performance status have been integrated into studies involving critically ill patients, generally for risk adjustment; however, they have not been evaluated in the context of frailty.35,36 Data from the Canadian National Population Health Survey showed that the prevalence of frailty was about 7% and that it increased exponentially with age.4 In a vulnerable cohort of older outpatients, the prevalence of frailty was 59%.3 We found frailty in 33% of the critically ill patients enrolled in our study, an estimate between the extremes of the general population and an older outpatient population. Notably, our cohort was relatively young compared with these cohorts, implying the susceptibility to critical illness may be “age-shifted” in those with frailty. This suggests that an episode of critical illness in a frail patient may herald a momentous transition toward greater homeostatic instability, disability and risk of death.11
Frailty is a common state preceding death.37 Two-thirds of frail patients have disabling trajectories at the end of life.37 In a recent population-based study, 26.7% of deaths were associated with frailty.38 Frailty is associated with high health service utilization, with most expenditures related to long-term care and in-patient care at the end of life.38 Indeed, health expenditures for frail people increase 2.4-fold on average in the final 3 months of life.38 Consistent with these observations, frail patients in our study had longer stays in ICU and hospital, had more acquired disability and had higher hospital readmission rates than their non-frail counterparts. Frail participants also had higher in-hospital and 12-month mortality. Moreover, we found graded increases in the risk of death associated with increasing severity of frailty.
We observed no differences between the frail and nonfrail patients in the intensity of treatment provided or in ICU mortality. These data suggest that frail patients, once admitted to ICU, received therapy commensurate with their illness severity, and perhaps only later had goals of care readdressed following a time-limited trial.39
Limitations
Our study has several limitations. First, the Clinical Frailty Scale, although a well-validated bedside assessment tool,3,10 has an inherent element of informed subjectivity. However, we believe we mitigated this by ensuring all research personnel were trained to use it systematically and were masked to the study hypotheses. This was reinforced by patients classified as frail having numerous features consistent with the frail phenotype.1,23
Second, we recruited participants after admission to ICU. Thus, we did not have reliable measures of health-related quality of life before admission, and all of our analyses were anchored to assessments that started in the ICU.
Third, we were unable to integrate dynamic functional measures such as mobility, grip strength and cognition before the development of critical illness that may have further informed on survival and trajectory relative to baseline. Similarly, we did not have markers of inflammation or nutritional status or other laboratory measures that might have helped with a mechanistic understanding of why frailty was associated with adverse events.
Conclusion
Frailty was common among critically ill adults aged 50 years or more and identified a vulnerable population at increased risk of adverse events, morbidity and mortality. Our findings suggest that routine assessment of frailty could provide more accurate prognostication and identify a vulnerable population that might benefit from follow-up and intervention.
Acknowledgements
Participating centres and investigators: Edmonton sites: University of Alberta Hospital: Sean Bagshaw, Robert McDermid, Darryl Rolfson, Ross Tsuyuki, Nadia Baig, Quazi Ibrahim and Sumit Majumdar; Grey Nuns Community Hospital: Daniel Stollery; Misericordia Community Hospital: Ella Rokosh. Calgary sites: Foothills Medical Centre: Thomas Stelfox; Rockyview General Hospital: George Alvarez; Peter Lougheed Hospital: Luc Berthiaume. The authors acknowledge the coordinators whose work was essential to completion of this study: Tracy Davyduke, Maliha Muneer, Kristen Reid, Gwen Thompson, Robin Scheelar, Jennifer Barchard and Samantha Taylor.
Footnotes
Competing interests: Ross Tsuyuki has served on advisory boards for Bristol-Myers Squibb, PharmaSmart International and Abbott Laboratories, and a data monitoring board for dabigatran studies for Boehringer Ingelheim; he has received consultant fees from Merck; and his institution has received grants from Sanofi and AstraZeneca. No competing interests were declared by the other authors.
This article has been peer reviewed.
Contributors: Sean Bagshaw, Thomas Stelfox, Robert McDermid, Darryl Rolfson, Ross Tsuyuki and Sumit Majumdar helped conceive and design the study and interpreted the data. Sean Bagshaw, Thomas Stelfox, Nadia Baig, Barbara Artiuch, Daniel Stollery and Ella Rokosh acquired the data. Sean Bagshaw and Quazi Ibrahim analyzed the data. Sean Bagshaw drafted the manuscript; all of the authors revised it critically for important intellectual content and approved the final version submitted for publication.
Funding: This study was supported by grants from the Canadian Intensive Care Foundation, the University Hospital Foundation and the Canadian Institutes of Health Research (CIHR grant no. MOP 111044). The funding agencies had no role in the design or conduct of the study, in the collection, management, analysis or interpretation of the data, or in the preparation, review or approval of the manuscript.
Sean Bagshaw holds a Canada Research Chair in Critical Care Nephrology and is a Clinical Investigator supported by Alberta Innovates – Healthx Solutions. Thomas Stelfox is supported by a New Investigator Award from CIHR and a Population Health Investigator Award from Alberta Innovates. Sumit Majumdar is a Health Scholar (supported by Alberta Innovates – Health Solutions and the Alberta Heritage Foundation for Medical Research) and holds the Endowed Chair in Patient Health Management (supported by the Faculties of Medicine and Dentistry and Pharmacy and Pharmaceutical Sciences, University of Alberta).
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- The association of demographics, frailty and multiple health conditions with outcomes from acute medical admissions to hospitals in England: exploratory analysis of an administrative dataset
- The impact of frailty on the outcomes of COVID-19 patients with persistent critical illness: A population-based cohort study
- Optimisation des soins chez les personnes agees gravement malades
- Optimizing care for critically ill older adults
- Association between preoperative frailty and outcomes among adults undergoing cardiac surgery: a prospective cohort study
- Measuring frailty in younger populations: a rapid review of evidence
- ERS International Congress 2020 Virtual: highlights from the Allied Respiratory Professionals Assembly
- Economic evaluation alongside the Probiotics to Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT): study protocol
- Threats to safe transitions from hospital to home: a consensus study in North West London primary care
- Pre-arrest and intra-arrest prognostic factors associated with survival after in-hospital cardiac arrest: systematic review and meta-analysis
- Evaluating probiotics for the prevention of ventilator-associated pneumonia: a randomised placebo-controlled multicentre trial protocol and statistical analysis plan for PROSPECT
- Selection and Receipt of Kidney Replacement in Critically Ill Older Patients with AKI
- Surrogates and Researchers Assessments of Prehospital Frailty in Critically Ill Older Adults
- Intensive care: balancing risk and benefit to facilitate informed decisions
- PREHAB study: a protocol for a prospective randomised clinical trial of exercise therapy for people living with frailty having cancer surgery
- Frailty in Critical Care: Examining Implications for Clinical Practices
- Risk of 12-month mortality among hospital inpatients using the surprise question and SPICT criteria: a prospective study
- Impact of frailty on outcomes after discharge in older surgical patients: a prospective cohort study
- PReventing early unplanned hOspital readmission aFter critical ILlnEss (PROFILE): protocol and analysis framework for a mixed methods study
- CYCLE pilot: a protocol for a pilot randomised study of early cycle ergometry versus routine physiotherapy in mechanically ventilated patients
- Do Self-Management Interventions Work in Patients With Heart Failure?: An Individual Patient Data Meta-Analysis
- Developing and validating a risk prediction model for acute care based on frailty syndromes
- Association between frailty and 30-day outcomes after discharge from hospital
- Frailty and Mortality in Dialysis: Evaluation of a Clinical Frailty Scale
- Frailty: Identifying elderly patients at high risk of poor outcomes
- La fragilite: Detecter les patients ages a risque eleve d'issues defavorables
More in this TOC Section
Similar Articles
Collections

