


Abstract
BACKGROUND: Although aggregate data suggest a link between snowfall and myocardial infarction (MI), individual risk has yet to be assessed. We evaluated the association between quantity and duration of snowfall and the risk of MI using nonaggregated administrative health data.
METHODS: We used a case–crossover study design to investigate the association between snowfall and hospital admission or death due to MI in the province of Quebec, Canada, between November and April during 1981–2014. The main exposure measures were quantity (in centimetres) and duration (in hours) of snowfall by calendar day. We computed odds ratios (ORs) and 95% confidence intervals (CIs) for the association between daily snowfall and MI, adjusted for minimum daily temperatures.
RESULTS: In all, 128 073 individual hospital admissions and 68 155 deaths due to MI were included in the analyses. The likelihood of MI was increased the day after a snowfall among men but not among women. Compared with 0 cm, 20 cm of snowfall was associated with an OR of 1.16 for hospital admission (95% CI 1.11–1.21) and 1.34 for death (95% CI 1.26–1.42) due to MI the following day among men. Corresponding ORs among women were 1.01 (95% CI 0.95–1.07) and 1.04 (95% CI 0.96–1.13). Similar but smaller associations were observed for snowfall duration (0 h v. 24 h) and MI.
INTERPRETATION: Both the quantity and duration of snowfall were associated with subsequent risk of hospital admission or death due to MI, driven primarily by an effect in men. These data have implications for public health initiatives in regions with snowstorms.
Myocardial infarction (MI) is a leading cause of morbidity and death.1,2 Ischemic heart disease accounted for an estimated 6 million years lived with disability and 8 million deaths worldwide in 2013 alone.3,4 However, MI prevention is challenging, in part because known risk factors explain only a fraction of cases. Determinants such as advanced age, smoking and diabetes are well established,2,5 but environmental risk factors, including the contribution of weather, are not well characterized. Many countries with a high incidence of MI have climates where extreme weather is common.4 Much attention has been given to temperature, since exposure to excessive heat increases the risk of hospital admission and death due to MI.6 New data suggest that cold temperatures may be associated with an even greater risk of death,7 in addition to documented peaks in MI incidence during winter months.6,8–11 Associations with other weather conditions, including snowstorms, however, have received less attention.
Snowstorms could affect the risk of MI, given the evidence that snow-related exertion, including shovelling, can excessively strain the cardiovascular system in susceptible individuals.12–14 Snowfall is flagged as a possible MI risk factor in northern countries, 9,10,15,16 but evidence based on aggregate patient data is conflicting. 9,10,12,15–20 Because the analysis of aggregate data can result in a loss of statistical power21 and carries a risk of ecologic bias,22 conclusive evidence of an association between snowfall and MI has yet to be established. Extreme weather patterns, including blizzards, are predicted to increase with climate change;23 thus, an increased risk of MI in connection with snowfall has clear public health implications.
We undertook an analysis of the likelihood of hospital admission or death due to MI following snowstorms using environmental and administrative health data for individuals in the province of Quebec, Canada, over a period of more than 2 decades.
Methods
Study design
We designed a time-stratified case–crossover study to test whether snowfall was associated with MI in Quebec, a northern region between the 45th and 62nd latitudes characterized by cold winters with subzero temperatures. Case–crossover designs are ideal when the event (MI) is acute and occurs shortly after the exposure (snowfall).24 The case–crossover design is a variant of the case–control study, with the principle difference that cases serve as their own controls.25 Instead of matching cases to other individuals, the case is defined as the calendar day that the MI occurred, and the case day is matched to nearby control days when MI did not occur. The weather for case days is subsequently compared with the weather for control days. Because each MI patient is their own control, characteristics such as smoking, socioeconomic status, comorbidity and season are identical between cases and controls. Thus, the case–crossover design automatically adjusts for both known and unknown confounders. 25 As such, weather is the primary characteristic that differs between cases and controls.
Data sources
We analyzed hospital admissions and deaths due to MI in Quebec from 1981 to 2014 using 2 different health administrative databases. We restricted data to the months of November through April, because snowfalls are rare during the other months. We obtained individual hospital admission records for MI from MED-ÉCHO (the provincial hospital discharge database) from 1989 (when collection of data in MED-ÉCHO began) to 2014 regardless of residency. Data on deaths due to MI were obtained from death registration certificates for Quebec residents between 1981 and 2013.
Detailed data on weather conditions, including daily snowfalls and temperatures, were obtained from Environment Canada for 18 meteorologic stations representative of each health region of the province.26 Regional weather data were matched directly to the region of residence.
Patient population
For cases, we identified individuals with MI using diagnostic codes of the International Classification of Diseases (ICD-9 code 410 and ICD-10 codes I21–I22). We included patients for whom MI was a reason for the hospital admission or the primary cause of death. For deaths, the case day was defined by the date of death. For hospital admissions, the case day was the date of presentation to the emergency department. For the 17% of patients who were admitted directly without initially presenting to an emergency department, the first day of the hospital admission was used as the case day.
We identified the sex and age (< 55, 55–64, 65–74, ≥ 75 yr) for all MIs. We used ICD codes to determine if cardiovascular comorbidity (heart, cerebrovascular, arterial, other cardiovascular disease) or risk factors (hypertension, diabetes, obesity, dyslipidemia, tobacco/chronic obstructive pulmonary disease) were present (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.161064/-/DC1). Data on cardiovascular comorbidities and risk factors were obtained from other causes of hospital admission in MED-ÉCHO, or from secondary causes of death in the death registration certificates. For deaths, data on secondary causes became available in 2000. We determined the level of material deprivation using an index of neighbourhood income, education and employment from census data linked with the postal code.27 We determined the tertile of material deprivation but could do so only beginning in 1989, when this indicator became available.
We selected controls using a time-stratified approach,24 such that control days were the same day of the week in the same calendar month as case days. For example, for a case day on a Friday in the first week of January, the control days were all remaining Fridays in January of the same year. Each case therefore had up to 4 controls. The time-stratified method for selecting controls minimizes bias due to seasonality, temporal trends in weather or medical care, and effects of the day of week.24,28 Also, bias due to unidirectional sampling is avoided by selecting controls before and after the date of the case.24
Exposure
Quantity of snowfall was defined as the total number of centimeters of snow during a calendar day, available as daily counts. Duration was defined as the total number of hours of snowfall during the day, computed from hourly data. To ensure that snowfall was measured before the occurrence of MI, we defined the primary exposure as the quantity or duration of snowfall during the calendar day before hospital admission or death.
As secondary exposures, we evaluated the quantity and duration of snow on the same calendar day as the MI, as well as snowfall 2 and 3 days before the MI. Both quantity and duration of snowfall were measured as continuous variables, expressed using splines with knots at the 5th, 50th, and 95th percentiles. To evaluate cumulative effects, we further analyzed 0, 1 and 2–3 consecutive days of snowfall of 5 cm or more (or 6 h or longer). This lag covers potentially delayed effects of snowfall, or delayed presentation for care.
The coldest daily temperature expressed as splines was used as a covariate in all analyses, with knots at the same percentiles.
Statistical analysis
The primary analysis was conducted for all individuals, and secondarily stratified according to sex, age and presence of cardiovascular comorbidity or risk factors. We considered that men might be at different risk for MI than women, both a priori and because of a potentially greater propensity for shovelling. We also sought to determine whether characteristics such as age and cardiovascular comorbidity modified the risks associated with snowfall. We used conditional logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between quantity (or duration) of snowfall and hospital admission (or death) due to MI the following day. Similarly, we estimated associations with MI events on the same day and 2 days following a snowfall, as well as the number of consecutive days of snowfall. We adjusted all models for the coldest daily temperature.
To ensure that associations were not masked by periods with relatively little snowfall, we carried out sensitivity analyses for the months of December through February. We verified the association between snowfall and MI stratified by tertile of material deprivation using an index of neighbourhood income, education and employment.27
We performed analyses with SAS version 9.3 (SAS Institute Inc.) using the restricted cubic spline macro.29
Ethics approval
Given that patient data were de-identified, the institutional review board of the Centre hospitalier de l’Université de Montréal provided a waiver for ethics review.
Results
In all, 128 073 individual hospital admissions and 68 155 deaths due to MI were analyzed for the association with the region-specific quantity and duration of snowfall. About 60% of the hospital admissions and deaths involved men (Table 1). One-third of MIs occurred the day following a snowfall, and about 10% occurred after snowfalls of 5 cm or more.
Distribution of myocardial infarctions the day after a snowfall and according to patient characteristics
Quantity of snowfall was associated with an increased likelihood of hospital admission or death due to MI the following day among men (Figure 1). The association between snowfall and MI was stronger among men, and weaker or absent among women. Compared with 0 cm, 20 cm of snowfall was associated with an OR of 1.16 for hospital admission due to MI the following day among men (95% CI 1.11–1.21) but no increased risk among women (OR 1.01, 95% CI 0.95–1.07). Similar associations were present for death due to MI the following day when stratified by sex (men: OR 1.34, 95% CI 1.26–1.42; women: OR 1.04, 95% CI 0.96–1.13). The p values for statistical tests of interaction between sex and quantity of snowfall were < 0.001 for both hospital admission and death due to MI.
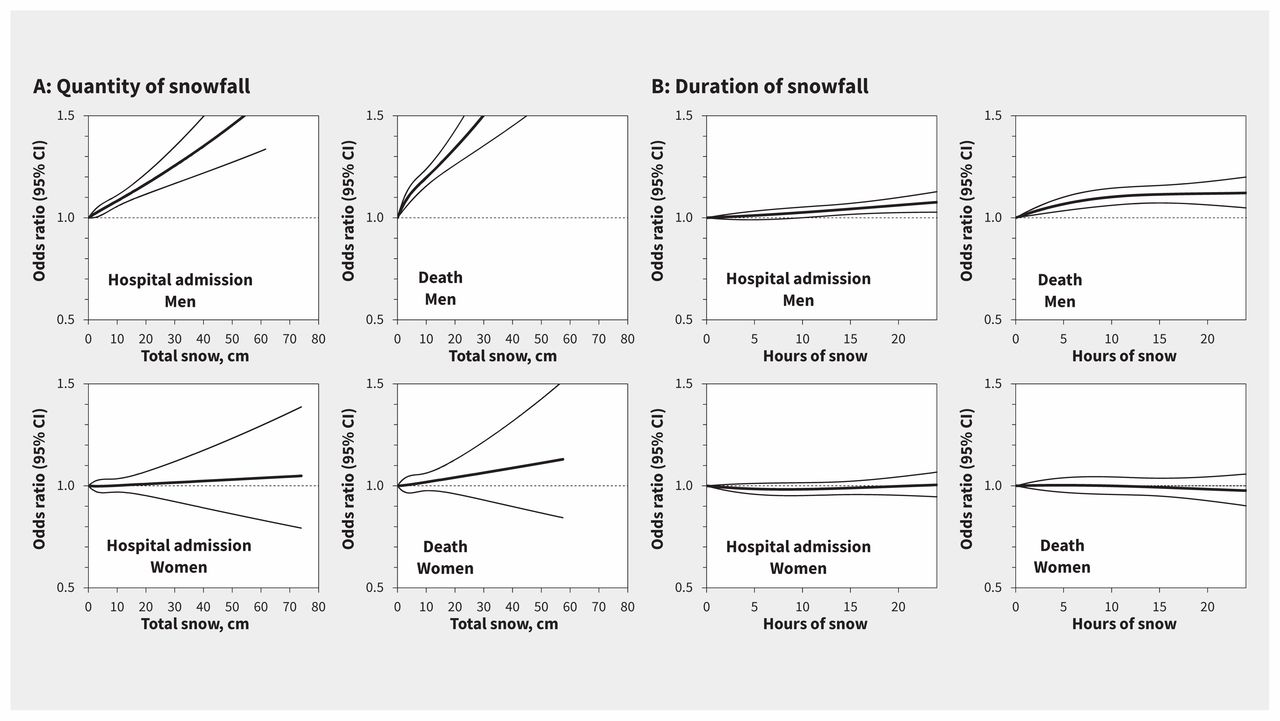
Association between (A) quantity and (B) duration of snowfall and hospital admission or death due to myocardial infarction (MI) among men and women the day after a snowfall. Odds ratios (central lines) and 95% confidence intervals (outer bands) were adjusted for temperature. Panels for duration of snowfall exclude MI events with missing data on duration. Values above 1.0 indicate an increased risk of hospital admission or death. CI = confidence interval.
Duration of snowfall was also associated with an increased likelihood of hospital admission or death due to MI among men. Compared with 0 hours, 24 hours of snowfall was associated with an OR of 1.08 for hospital admission (95% CI 1.03–1.13) and 1.12 for death (95% CI 1.05–1.20) the following day among men. No association with 24 hours of snowfall was observed among women (hospital admission: OR 1.00, 95% CI 0.95–1.07; death: 0.95, 95% CI 0.90–1.06). The p values for interaction of sex and duration of snowfall were 0.02 for hospital admission and < 0.001 for death due to MI. Similar results were found for snowfall the day of MI (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.161064/-/DC1). There was no association between snowfall and MI 2 or 3 days later.
In analyses stratified by age, there was no compelling evidence that associations were more important in any particular age group (Figure 2). Associations with snowfall were present regardless of the presence of cardiovascular comorbidity or risk factors, although individuals without comorbidity or risk factors had a higher risk of hospital admission with longer durations of snowfall (Figure 3).

Association between (A) quantity and (B) duration of snowfall and hospital admission or death due to myocardial infarction (MI) by age group the day after a snowfall. Odds ratios (central lines) and 95% confidence intervals (outer bands) were adjusted for temperature. Panels for duration of snowfall exclude MI events with missing data on duration. Values above 1.0 indicate an increased risk of hospital admission or death. CI = confidence interval.

Association between (A) quantity and (B) duration of snowfall and hospital admission or death due to myocardial infarction (MI) the day after a snowfall, according to presence of cardiovascular (CV) comorbidity or risk factors. Odds ratios (central lines) and 95% confidence intervals (outer bands) were adjusted for temperature. Panels for duration of snowfall exclude MI events with missing data on duration. Values above 1.0 indicate an increased risk of hospital admission or death. CI = confidence interval.
The likelihood of MI among men increased with the consecutive number of days of snow (Table 2). Compared with 0 days, 2–3 consecutive days of 5 cm or more of snowfall was associated with an OR of 1.09 for hospital admission due to MI among men (95% CI 1.04–1.14), whereas 1 day of 5 cm or more was associated with an OR of 1.06 (95% CI 1.03–1.08). Similarly, 2–3 consecutive days of 5 cm or more was associated with an OR of 1.20 for death due to MI among men (95% CI 1.12–1.28), whereas 1 day of snowfall was associated with an OR of 1.14 (95% CI 1.10–1.18). A dose–response trend among men was also present for 2–3 consecutive days of snowfall lasting 6 hours or more. Among women, 2–3 consecutive days of 5 cm or more of snowfall was not associated with hospital admission (OR 0.98, 95% CI 0.92–1.04) or death (OR 1.08, 95% CI 0.99–1.17) due to MI.
Association of number of days of consecutive snowfall with myocardial infarction among men and women
In the sensitivity analyses, data restricted to the months of December through February yielded similar results (Appendix 3). The association between snowfall and MI was present in all deprivation tertiles (Appendix 4). Temperature was not associated with hospital admission or death due to MI in models adjusted for snowfall (Appendix 5). (Appendices available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.161064/-/DC1.)
Interpretation
In our analysis of nearly 200 000 MI events in the province of Quebec, quantity and duration of snowfall were associated with an increased likelihood of hospital admission or death due to MI. The association was observed among men but not among women and was strongest the day following a snowfall. Two or 3 days of consecutive snowfall increased the risk of MI further. Risks were elevated regardless of age, cardiovascular comorbidity or cardiovascular risk factors. These results call for caution after snowfalls, particularly for men who may be at higher risk, and may have increasing relevance over time, considering climate change and predictions that extreme weather will increase.23
Several ecologic studies have highlighted the possibility that snowfall is associated with MI risk. Daily counts of death due to MI were associated with snowfalls in Pennsylvania, Rhode Island and Minneapolis–St. Paul, all located in the northern regions of the United States.9,16 A correlation between snowfall and incidence of MI was also reported in Switzerland,15 which has a climate somewhat comparable to Quebec’s. In contrast, the frequency of hospital admission due to MI was not associated with snowfall in a Swedish sample of 382 patients.19 Other ecologic analyses similarly failed to find an increased incidence of MI the day of a snowfall, but they may well have been underpowered.17,18,20
In our study, the increased risk of hospital admission or death due to MI was primarily among men. We suspect that shovelling was the main mechanism linking snowfall with MI. Men are potentially more likely than women to shovel, particularly after heavy snowfalls. Snow shovelling is a demanding cardiovascular exercise requiring more than 75% of the maximum heart rate,12,14 particularly with heavy loads.14 It is a unique activity with both static and dynamic components, involving the Valsalva manoeuvre and increased systolic blood pressure.12,13 Intense arm effort, repetitive motion, static upright posture, peripheral vasoconstriction14 and greater myocardial afterload all increase the risk of coronary plaque rupture and thrombus formation.12,14 Risks may be exacerbated by exposure to cold temperatures,13,14 which increases vasoconstriction and blood pressure, and consequently the preload, cardiac output and oxygen demand of the heart.30 Sudden exposure to cold temperatures has been shown to lead to sympathovagal activation and arrhythmia,31 and breathing cold air has been shown to reduce coronary blood flow.32
Limitations
Although our study represents a large analysis of MI in a region where snowfall is common, a number of limitations deserve attention. Use of administrative data to identify MI events may have resulted in misclassification for a proportion of cases. Diagnostic criteria for MI, as well as the sensitivity of biochemical assays for MI detection, changed during the study period. However, misclassification and evolving diagnostic criteria are unlikely to vary with degree of snowfall, or the short 1-month span within which controls were identified.
We measured snowfall and temperature levels on the basis of regional estimates from weather stations, which may have led to imprecision in the exposure assignment in some cases. We do not have information on sex-specific shovelling habits, the size of areas shovelled or whether snow removal was automated (snow blowers v. manual shovelling). Although these are potentially important considerations, the hypothesis that shovelling is associated with an increased risk of MI events among men remains plausible. Some researchers have even reported that cardiac demands are elevated with automated snow removal.12
Finally, the generalizability of the findings to areas with different levels of snowfall remains to be investigated.
Conclusion
Both the quantity and duration of snowfall were associated with subsequent risk of hospital admission or death due to MI in the province of Quebec, particularly among men. These findings are most likely related to the increased cardiac demands of snow shovelling. Climate change and the predicted increase in the frequency and intensity of winter storms raise the possibility of a greater incidence of MI in the future. Clinicians and public health practitioners should consider awareness campaigns before the winter season to inform individuals of the risk of MI after a snowfall, and possibly advise against shovelling for the most at risk patients.
Footnotes
CMAJ Podcasts: author interview at https://soundcloud.com/cmajpodcasts/161064-res
See related article at www.cmaj.ca/lookup/doi/10.1503/cmaj.170022
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Nathalie Auger conceived and designed the study. Marianne Bilodeau-Bertrand and Clément Paris analyzed the data under guidance of Nathalie Auger. Brian Potter, Audrey Smargiassi and Tom Kosatsky helped interpret the results. Nathalie Auger, Brian Potter and Marianne Bilodeau-Bertrand drafted the manuscript, and Audrey Smargiassi, Clément Paris and Tom Kosatsky revised it for critical intellectual content. All of the authors approved the final version of the manuscript to be published and agreed to act as guarantors of the work.
Funding: The study was funded by the Canadian Institutes of Health Research (grant no. MOP-142277) and Fonds de recherche du Québec-Santé (career award no. 25128). Clément Paris was supported by a bursary from the Conseil Régional de Provence-Alpes-Côte-d’Azur.
- Accepted January 4, 2017.
References
In this issue
Article tools






{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Snowfall and myocardial infarction. What is the effect of barometric pressure?
- The cardiovascular risk of snowfall and snow shovelling in Canada
- Response to "Its not just the snow; its also the cold"
- Its not just the snow; its also the cold
- The eco-biological-behavioural perfect storm that follows heavy snowfall
More in this TOC Section
Similar Articles


Podcast