


Low-risk ankle injuries are the most common lower-extremity injuries in children
Low-risk injuries in the lower extremities among children include lateral ankle sprains and isolated nondisplaced distal fibular Salter–Harris I, II or avulsion fractures (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.170965/-/DC1). These injuries have excellent functional outcomes and are low risk for future complications.1
The Low Risk Ankle Rule is a clinical decision rule that helps to reduce the use of unnecessary radiographs in children
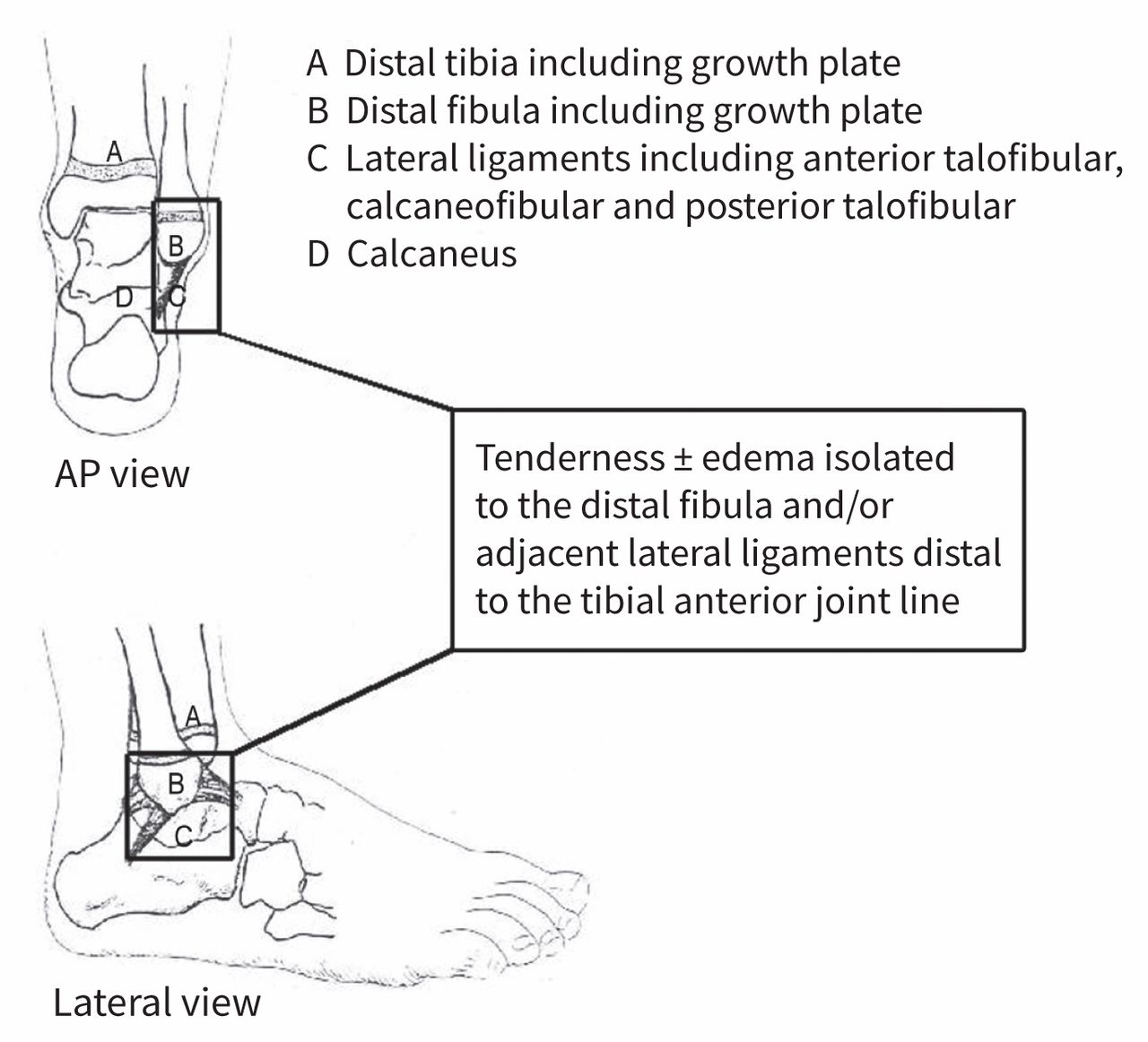
The rule (Figure 1), which is unique from the Ottawa Ankle Rules, identifies which ankle injuries in children are low risk. It was validated in children 3 to 16 years of age in six Canadian emergency departments. In a prospective multicentre implementation study that included 2151 children, this rule had 100% sensitivity and safely reduced imaging by 22%.1 This rule is also cost-effective.2 Before applying the rule, physicians should do a comprehensive ankle examination, including the anterior joint line, and above and below the joint, to avoid missing distal fractures of the tibia (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.170965/-/DC1).3

Low Risk Ankle Rule. If a child presents with a low-risk injury on examination (i.e., tenderness and swelling isolated to the distal fibula or adjacent lateral ligaments distal to the tibial anterior joint line), then radiography may not be necessary to exclude a clinically important ankle injury. Reproduced, with permission, from Boutis et al.6
Injuries suspected to be distal fractures of the fibular Salter–Harris I growth plate are almost always ankle sprain injuries
Because of presumed weakness of the growth plate relative to adjacent ligaments, children (who have immature skeletons) with isolated swelling and tenderness over the distal fibula and no radiographic evidence of fracture, are often diagnosed with Salter–Harris I fractures. However, a study that included 135 children who had this presentation showed that 97% actually had ligamentous injuries rather than growth plate fractures.4
Low-risk ankle fractures in children can be managed with symptomatic and supportive care
Randomized controlled trials have shown that management of these fractures with an ankle brace and a self-regulated return to activities was superior to a fibreglass cast or backslab for three weeks with respect to recovery.5
Follow-up of low-risk ankle fractures with a primary care physician is appropriate
Follow-up with an orthopedic surgeon is not necessary routinely and should be reserved for cases that are not improving as expected.4,5
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
In this issue

{kind=link}
Article tools



Jump to section
- Article
- Low-risk ankle injuries are the most common lower-extremity injuries in children
- The Low Risk Ankle Rule is a clinical decision rule that helps to reduce the use of unnecessary radiographs in children
- Injuries suspected to be distal fractures of the fibular Salter–Harris I growth plate are almost always ankle sprain injuries
- Low-risk ankle fractures in children can be managed with symptomatic and supportive care
- Follow-up of low-risk ankle fractures with a primary care physician is appropriate
- Footnotes
- References
- Figures & Tables
- Related Content
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

