


A 59-year-old man with diabetes and alcoholic cirrhosis presented to the emergency department after three weeks of difficulty in walking and two weeks with impaired speech. He had been taking moxifloxacin (400 mg taken orally daily) and metronidazole (750 mg taken orally every six hours) for osteomyelitis for six weeks. On examination, he had dysarthria, ataxia, and symmetric dysmetria and dysdiadochokinesia, but his strength, sensation and reflexes were all normal. On magnetic resonance imaging (MRI) of the brain, he had diffusion restriction and fluid-attenuated inversion recovery (FLAIR) signal changes in the dentate nuclei bilaterally (Figure 1A), structures that are involved in voluntary movement and cognition.
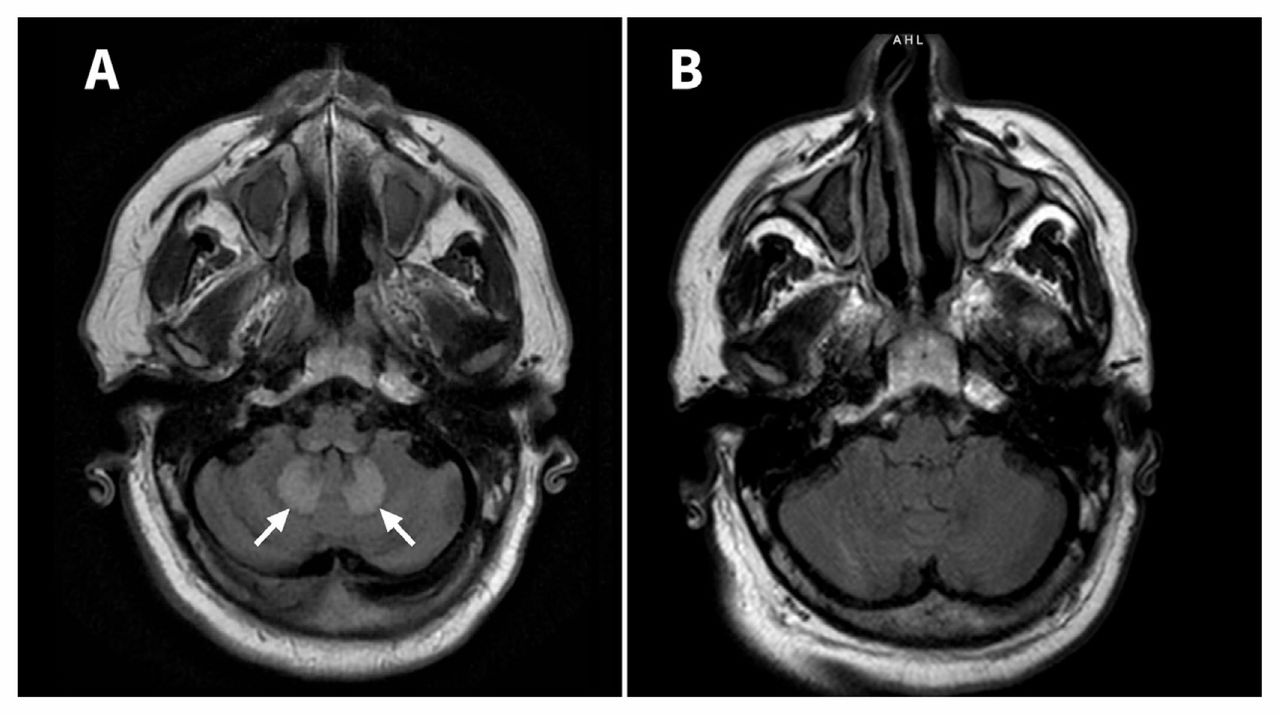
A) Magnetic resonance image (axial view) of the brain in a 59-year-old man with cerebellar neurotoxicity induced by metronidazole, showing fluid-attenuated inversion recovery (FLAIR) signal changes in the dentate nuclei bilaterally( arrows). FLAIR signal hyperintensity is also seen in the inferior aspect of the cerebellar peduncles bilaterally, which is an artifact. Diffusion restriction was seen in the dentate nuclei on the dedicated diffusion weighted imaging sequence (not shown). B) Axial section of the brain of the same patient four weeks after he stopped taking metronidazole, showing resolution of the abnormalities in the dentate nuclei.
This pattern on imaging has a broad differential diagnosis, but is typical of metronidazole neurotoxicity1 and is partially or completely reversible after withdrawal of the offending agent.2 After discontinuation of metronidazole and intensive physiotherapy, the patient’s symptoms had improved substantially. Four weeks after stopping treatment with metronidazole, his symptoms had completely resolved, and repeat MRI of the brain showed resolution of the abnormalities in the bilateral dentate nuclei (Figure 1B). Although both diabetes and alcoholic cirrhosis can cause or contribute to neuropathy, the rapid onset and pattern of injury seen in our patient are not typical of these conditions, and the complete resolution of symptoms after stopping the antibiotics is more suggestive of drug toxicity. Wernicke encephalopathy may also affect the dentate nuclei; however, our patient had been abstinent from alcohol for nine years.
Despite being in common use, metronidazole rarely causes cerebellar neurotoxicity.2 Damage can occur even at therapeutic doses, and although our patient received a higher dose than typically prescribed (125 g in total), the literature suggests that cerebellar neurotoxicity is unrelated to cumulative dose exposure or duration of treatment.3 Metronidazole toxicity can be diagnosed clinically or with an MRI demonstrating characteristic findings of symmetrically increased signal intensity for T2-, FLAIR- and diffusion-weighted imaging signal intensity in the supratentorial white matter and the deep cerebellar nuclei, in particular the dentate nuclei.1,4
Other neurologic adverse effects include peripheral neuropathy, encephalopathy, seizures and optic neuropathy, which are partially or completely reversible within weeks of stopping the medication.2,3
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

