


A previously healthy 21-year-old man presented to the emergency department with a 3-month history of lethargy and progressive abdominal pain and distention. He reported 6–8 watery, nonbloody bowel movements per day for the preceding month, along with anorexia and weight loss. He had no history of fever or chills. Our patient reported moderate alcohol consumption and he regularly smoked tobacco and marijuana. He had no history of intravenous drug use or sexually transmitted infections. He had travelled to Cabo San Lucas, Mexico, 8 months earlier, where he had had a 3-day self-limited episode of gastroenteritis. He also reported swimming in freshwater lakes in British Columbia.
On physical examination, our patient was cachectic. His vital signs were normal. He had decreased air entry to his lung bases bilaterally and his abdomen was distended, with shifting dullness. Genital and perianal examinations were normal. He had no active joints, rash, lymphadenopathy, or stigmata of chronic liver disease, aside from his ascites.
He had an elevated C-reactive protein of 196 (normal < 3.1) mg/L, eosinophilia of 2.2 (normal < 0.45) × 109/L, and normocytic anemia. Serum albumin was low at 17 (normal range n = 35–50) g/L without evidence of proteinuria. Liver enzymes were normal. Blood cultures, hepatitis B and C, and HIV serology were negative. Serum immunoglobulin E (IgE) was markedly elevated at 2100 (normal range n = 0–430) μg/L.
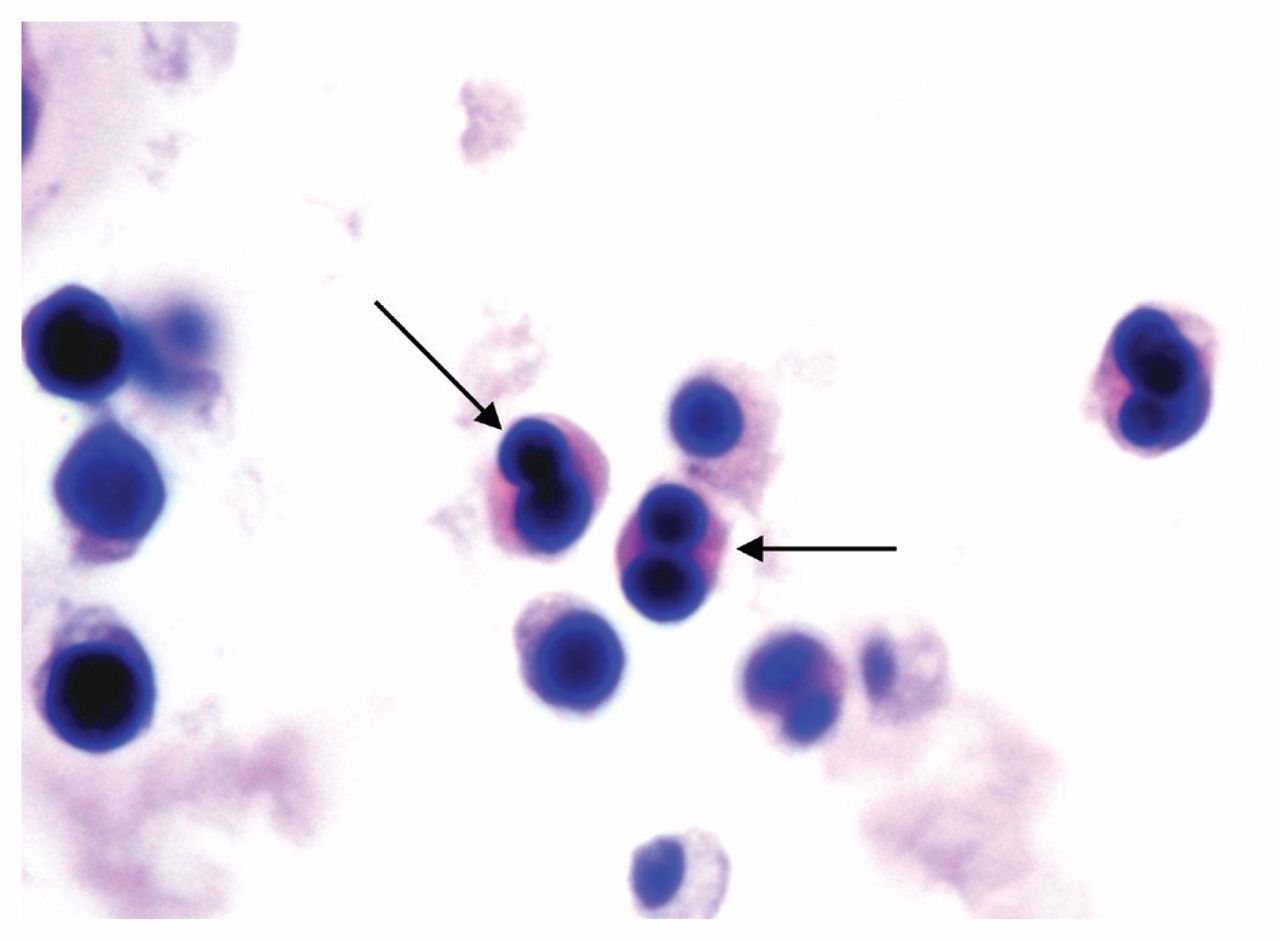
In hospital, our patient underwent an ultrasound-guided paracentesis for both diagnostic and therapeutic purposes, with drainage of 5 L. Ascitic fluid analysis showed 1608 × 106 nucleated cells (43% eosinophils, 23% lymphocytes, 31% macrophages, 3% neutrophils) (Figure 1). Bacterial culture was negative and fluid microscopy did not detect acid-fast bacilli or malignant cells. Fluid albumin count was low at 16 g/L, giving a serum ascites albumin gradient of 1g/L, arguing against a diagnosis of portal hypertension.

Ascites fluid specimen containing predominantly eosinophils (arrows) and mononuclear inflammatory cells (hematoxylin and eosin stain; original magnification × 1000).
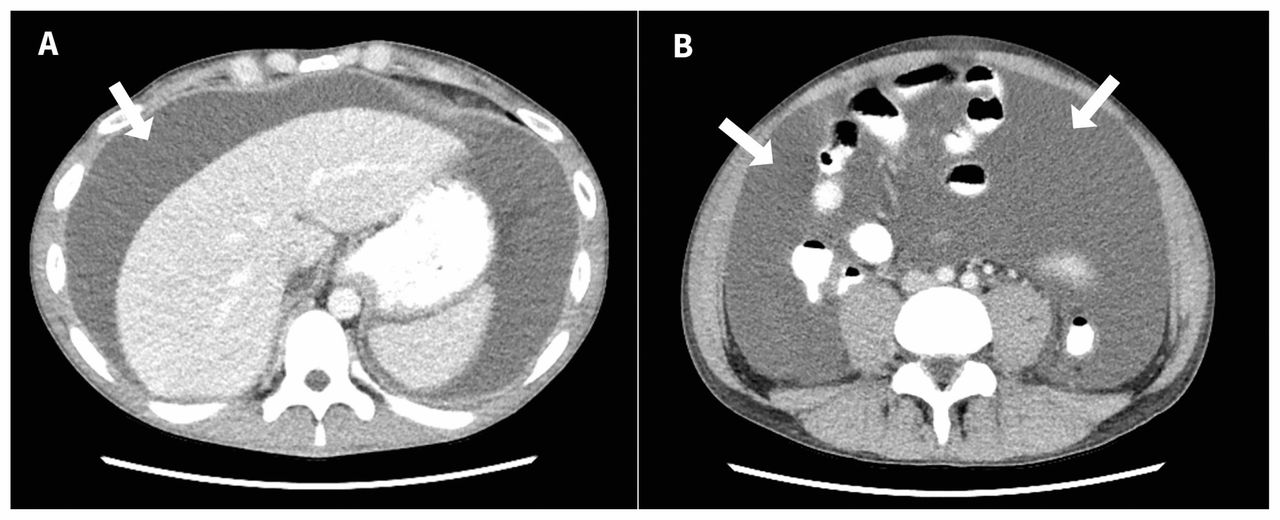
A computed tomography (CT) scan of the patient’s abdomen before the paracentesis showed large-volume ascites and bilateral pleural effusions (Figure 2). His liver, spleen and kidneys appeared unremarkable. A Doppler ultrasound showed no vascular abnormalities or evidence of Budd–Chiari syndrome.

Axial views showing large-volume ascites on computed tomography (CT) scan of the abdomen (A) and pelvis (B) of a 21-year-old man.
The differential diagnosis for this subacute gastrointestinal syndrome, characterized by eosinophilia and eosinophilic ascites, includes both infectious and noninfectious causes (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.181072/-/DC1). Among infectious causes, gastrointestinal parasitic infection by helminths and protozoa should be considered based on epidemiological risk. In this patient, stool and ascitic fluid ova and parasite testing, as well as strongyloides and Toxocara serology, were negative. Among bacterial infections, in the setting of negative stool cultures, less common causes of this syndrome include abdominal tuberculosis and Tropheryma whipplei enteritis.1 No risk of tuberculosis exposure was identified. Chest x-ray did not show granulomata, and ascitic fluid mycobacterial stains (and, ultimately, culture) were negative. Tropheryma whipplei histopathology and molecular testing of duodenal biopsy were negative.
Given the negative work-up for infectious etiology, which noninfectious cause is most in keeping with the patient’s clinical picture?
Celiac disease
Primary eosinophilic gastroenteritis
Eosinophilic granulomatosis with polyangiitis
Drug-induced eosinophilia
Carcinoid (neuroendocrine) tumour
The correct answer is (b). Celiac disease was high on the differential diagnosis, owing to the patient’s clinical picture of malabsorption — including weight loss, diarrhea, anemia and hypoalbuminemia — as well as his white race (Box 1). We excluded this diagnosis on the basis of a negative serum anti-tissue transglutaminase antibody (95% sensitivity).4
| Disease | Clinical signs and symptoms |
|---|---|
| Celiac disease | Abdominal pain, steatorrhea, flatulence, weight loss |
| Primary eosinophilic gastroenteritis | Nausea, vomiting, diarrhea, dyspepsia, weight loss; uncommonly, obstructive-type symptoms (e.g., pyloric stenosis, intestinal obstruction) or ascites |
| Eosinophilic granulomatosis with polyangiitis | Pulmonary symptoms most common, with asthma as the cardinal feature (> 90% of patients). Fatigue, weight loss, fever, arthralgias, rhinosinusitis, urinary abnormalities (e.g., hematuria, proteinuria) with or without renal dysfunction, neurologic dysfunction, purpura |
| Carcinoid (neuroendocrine) tumour | Carcinoid syndrome, which may involve facial flushing, wheezing, diarrhea, abdominal cramping or peripheral edema; advanced small bowel disease may present with obstruction or ascites |
| Drug-induced eosinophilia | Ranges from asymptomatic to life threatening; uncommonly, drug reaction with eosinophilia and systemic symptoms, including triad of skin eruption, fever and organ involvement (kidneys, heart, liver, lung). |
* Many of the disease entities listed are most commonly asymptomatic, or patients may present with only some of the listed clinical manifestations. Although the aim of this table is to cover the more common clinical features, it is not a fully comprehensive list. Refer to Appendix 1 (www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.181072/-/DC1) for the complete table, including infectious causes.
We also considered eosinophilic granulomatosis with polyangiitis, particularly in the context of the patient’s peripheral eosinophilia and elevated serum IgE. A detailed review of systems showed no clinical features consistent with atopic disease, such as asthma and allergic rhinitis. A chest x-ray showed no evidence of pulmonary opacities or nodular disease. We also ordered an antineutrophil cytoplasmic antibody, which can be positive in some patients with eosinophilic granulomatosis with polyangiitis. This test was negative. Additional evidence arguing against this condition was a lack of skin manifestations in the patient, a normal echocardiogram and normal urinary sediment without hematuria or red cell casts.
We considered an advanced carcinoid (neuroendocrine) tumour of the small bowel. To rule this out, we sent our patient’s ascitic fluid for cytology, which showed no malignant cells. We also ordered carcinoid tumour markers, including 5-hydroxyindoleacetic acid and chromogranin A, which were both negative. These results, combined with the lack of peritoneal thickening on the CT scan of the patient’s abdomen and pelvis, reassured us that a carcinoid tumour was less likely.
Moreover, given the subacute nature of this gastrointestinal illness, the possibility of drug-induced eosinophilia had to be addressed. On detailed history, the patient said he had not used any prescription medications, supplements or herbal remedies over the preceding 12 months. The 2 most common clinical features of drug reaction with eosinophilia and systemic symptoms (DRESS), fever and rash, were not seen in our patient, making a severe drug-induced eosinophilia unlikely.
At this point, primary eosinophilic gastroenteritis was highest on the differential. We proceeded with further investigations to confirm this diagnosis.
Which diagnostic test is most appropriate next?
Liver biopsy
Capsule endoscopy
Upper endoscopy with multiple biopsies
Omental biopsy
Diet modification and symptom monitoring
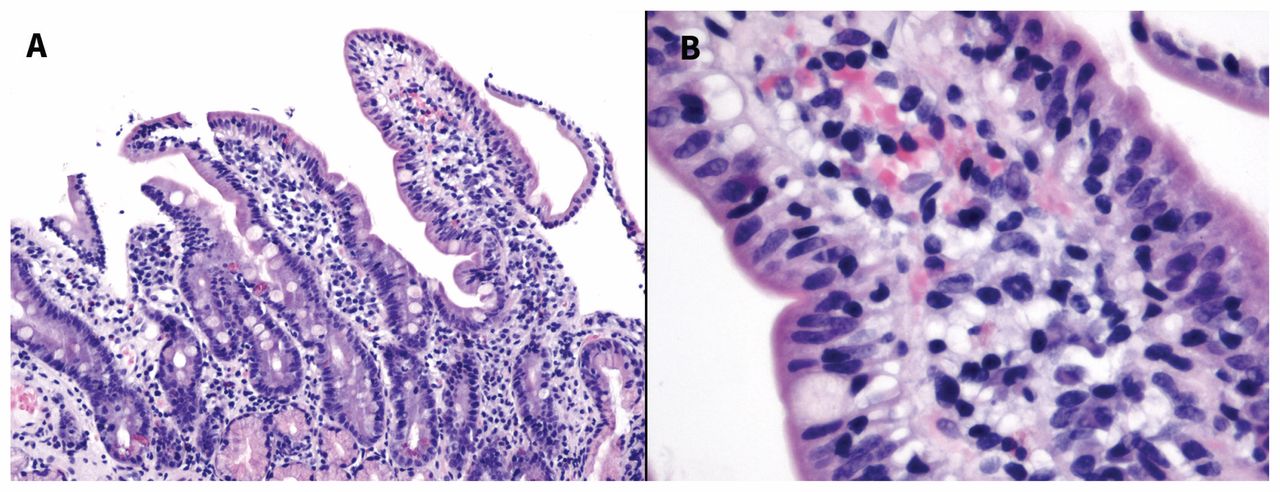
The correct answer is (c). In addition to clinical symptoms and laboratory investigations, upper endoscopy with multiple biopsies from both normal- and abnormal-appearing mucosal areas must be taken. Upper endoscopy showed mild Los Angeles grade A esophagitis with no features of eosinophilic esophagitis, such as esophageal rings, linear furrows or white papules. The patient also had a small hiatus hernia, mild gastritis and a normal duodenum. There was no evidence of malignancy, inflammatory bowel disease or celiac disease. Esophageal histology showed no features of eosinophilic esophagitis, and small bowel mucosal biopsies were normal (Figure 3).
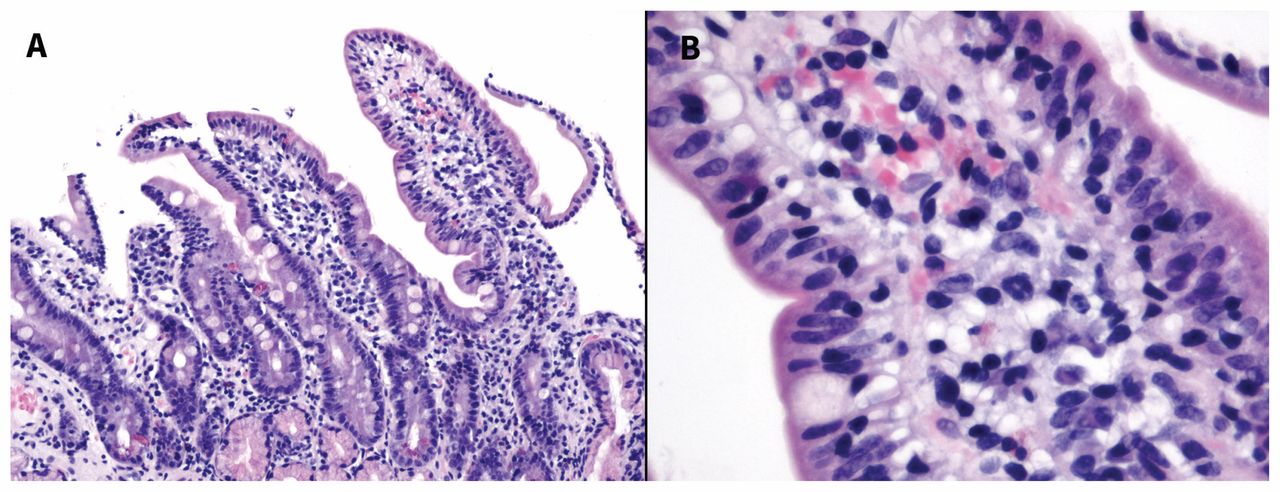
Histological image showing (A) small bowel mucosa of a 21-year-old man, with normal villous architecture and without inflammatory infiltrates (hematoxylin and eosin stain; original magnification × 100); (B) with normal epithelium (hematoxylin and eosin stain; original magnification × 400).
The patient was discharged home after the preliminary diagnostic work-up and ascitic fluid drainage. Two weeks later, he returned to the emergency department with symptomatic reaccumulation of his ascites. The consulting gastroenterologist started him on a 2-week course of 40 mg of oral prednisone, followed by a 2-week dose taper. Given the risk of triggering strongyloides hyperinfection, serology and stool examination were confirmed negative before initiating steroids. The patient was also instructed to start a food elimination diet, removing the 6 most common food allergies: wheat, milk, soy, tree nuts, shellfish and eggs.10 Over the next few days, his ascites and abdominal discomfort started to resolve.
At 2-month follow-up, the patient had no ascites, abdominal pain or diarrhea. He remained adherent to the recommended food elimination diet. His laboratory values paralleled his symptomatic improvement (Box 2).
| Marker | On | admission 2-month follow-up | 4-month follow-up | Normal values |
|---|---|---|---|---|
| Leukocyte count, × 109/L | 11.1 | 9.4 | 5.1 | 4.0–11.0 |
| Eosinophils, × 109/L | 2.2 | 1.0 | 0.4 | < 0.45 |
| C-reactive protein, mg/L | 196 | 50 | 0.5 | < 3.1 |
Discussion
Eosinophilic gastroenteritis is an uncommon, chronic disease affecting the gastrointestinal tract in both children and adults.5 The estimated prevalence of primary eosinophilic gastroenteritis is fewer than 10 in 100 000 people.2 Eosinophilic gastroenteritis is more common in white men. The disease can involve any part of the gastrointestinal tract, from the esophagus to the rectum; however, the stomach is most commonly affected, followed by the small intestine and colon.5 The disease was first described by Kaijser in 1937.6 Because it is uncommon, epidemiology and pathophysiology are not yet well characterized.
Based on the depth of eosinophil penetration, eosinophilic gastroenteritis can be divided into 3 subtypes that vary in clinical presentation: mucosal, muscularis and subserosal.7 The mucosal subtype most commonly presents as a malabsorption syndrome, with symptoms of nausea, vomiting, diarrhea, dyspepsia and weight loss. The muscularis subtype often presents with obstructive-type symptoms, such as pyloric stenosis, intestinal obstruction or, rarely, intussusception. The subserosal subtype is the least common subtype, in which patients often have eosinophilic ascites; this subtype best correlates with the presentation of our patient.2,7
The 4 criteria required for the diagnosis of eosinophilic gastroenteritis include gastrointestinal symptoms, eosinophilic infiltration of the gastrointestinal tract, absence of extraintestinal eosinophilic end organ disease, and exclusion of parasitic disease.5,8 Laboratory findings that support the diagnosis of eosinophilic gastroenteritis often include peripheral eosinophilia, hypoalbuminemia, elevated IgE and microcytic anemia.9
Given that eosinophilic gastroenteritis commonly involves eosinophilia and elevated serum IgE and responds to corticosteroids, it has been postulated that eosinophilic gastroenteritis may be hypersensitivity mediated.10 For this reason, food-elimination diets can be trialled.2,10 However, the evidence in support of elimination diets in eosinophilic gastroenteritis is based predominantly on studies from eosinophilic esophagitis, a related but distinct eosinophilic disease that has been more extensively studied.11
There have been no large placebo-controlled trials comparing various pharmacologic therapies for eosinophilic gastroenteritis. The natural history of this disease appears to be a chronic waxing and waning course, often requiring steroids at initial presentation and during “flare-ups” for symptom management.7,10 Various steroidsparing medications have been proposed with the allergic hypothesis in mind, such as montelukast (a leukotriene receptor antagonist), ketotifen (an antihistamine), suplatast tosilate (anti-interleukin 4 and 5) and omalizumab (anti-IgE monoclonal antibody). Case reports have suggested variable benefit of these drugs.10,11
Physicians should be aware of this disease, as making the diagnosis requires a high index of clinical suspicion. An appreciation of key clinical features, specifically gastrointestinal symptoms with eosinophilia, and without evidence of parasitic infection, is central to diagnosis. This case also highlights the importance of maintaining a broad differential for eosinophilia. Early diagnosis and treatment may prevent more serious complications, such as gastrointestinal obstruction or ascites.
Acknowledgement
The authors thank Dr. Robert Wolber for his contribution regarding pathology images and their interpretation, in order to provide a further layer of depth to this interesting case.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: All authors contributed to the conception and design of the work, drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

