


A 67-year-old woman and United Kingdom resident originally from Equador had a 5-month history of unsteadiness, lower limb weakness and urinary incontinence during which she had 2 episodes of thunderclap headache. On examination, the patient had right upper motor neuron facial weakness and symmetrically brisk reflexes. Brain magnetic resonance imaging (MRI) showed hydrocephalus and a cyst (23 mm in diameter) with a small nodule at its posterior-superior wall in the frontal horn of the left lateral ventricle (Figure 1, top left image). We inserted an extraventricular drain. Results for cysticercus antigen were positive in both serum and cerebrospinal fluid, and a diagnosis of neurocysticercosis was made. The cyst was inoperable, and we prescribed steroids and antiparasitics as treatment.
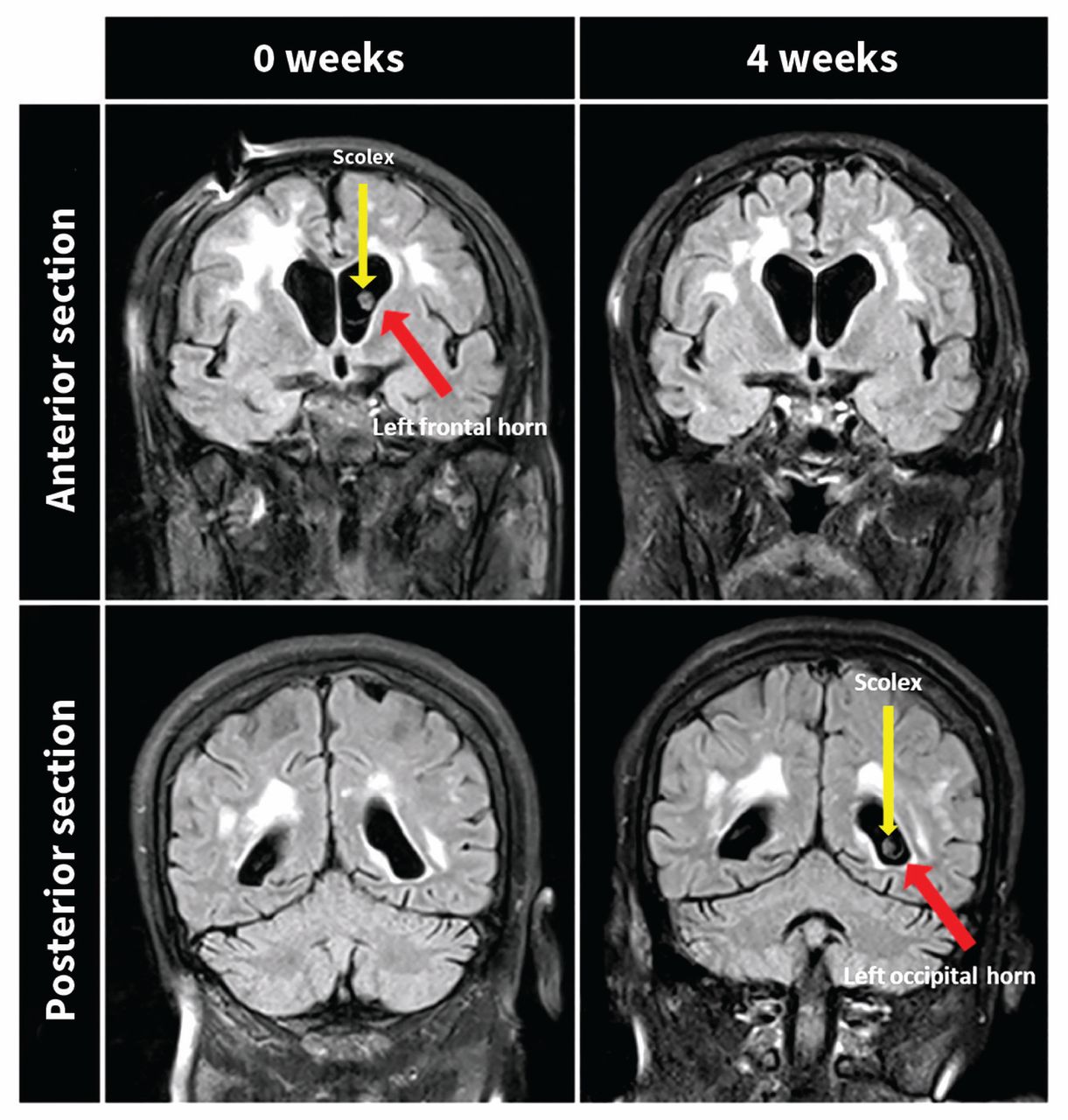
Magnetic resonance images of the brain of a 67-year-old woman with neurocysticercosis showing the shift of the intraventricular larval cyst from the frontal horn (week 0) to the occipital horn (week 4) of the left lateral ventricle. The scolex is visible in the anterior section of the brain at week 0 and the posterior section of the brain at week 4 as a small solid nodule emerging from the posterior-superior wall of the cyst.
Repeat MRI of the brain 4 weeks later showed migration of the cyst to the left occipital horn and inflammatory changes along its ependymal surface, consistent with ventriculitis (Figure 1, bottom right image).
Neurocysticercosis caused by the pork tapeworm Taenia solium is endemic in Central and South America, India, China, Southeast Asia and sub-Saharan Africa.1 Intraventricular neurocysticercosis occurs in 10%–20% of cases, and symptoms of increased intracranial pressure are caused by blockage of ventricular outflow tracts, resulting in obstructive hydrocephalus, cysticercotic arachnoiditis or mass effect produced by cysts in basal subarachnoid cisterns.2 Mortality is about 20%.2 The incubation period varies substantially (up to several years),2 and prognosis varies according to the location and burden of the parasite.
Computed tomography is preferred for identifying parenchymal lesions, and MRI is better for intraventricular cysts.3 A scolex (anterior end of the tapeworm appearing as a 2–4 mm rounded and elongated nodule within the cyst) is pathognomonic radiographically. 3 If serologic testing is nonconfirmatory and radiographic appearances are nonspecific, a biopsy is required.1
Intraventricular neurocysticercosis can be managed surgically or with antiparasitic and anti-inflammatory agents, preferably by endoscopic removal of the cyst with immediate drainage of cerebrospinal fluid or shunt placement as needed for most cases of hydrocephalus. Our patient responded well to treatment, with amelioration of her neurological symptoms.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

