


Women in Canadian medicine consistently earn less than men.
The pay gap between women and men exists within every medical specialty and also between specialties, with physicians in male-dominated specialties receiving higher payments.
The gender pay gap in medicine is not explained by women working fewer hours or less efficiently but, rather, relates to systemic bias in medical school, hiring, promotion, clinical care arrangements, the fee schedule itself and societal structures more broadly.
Actions for closing the gap include antioppression training, challenging the hidden curriculum in medical education, fair and transparent hiring and referral processes, changing the relative value of fee codes and transparent reporting of physician payments stratified by gender.
The gender pay gap, defined as the difference between what men and women earn for roughly equivalent work, has remained a core challenge in employment equity despite decades of activist effort and the substantial movement of women into the workplace. The Canadian government is taking steps to address the issue broadly,1 but there has been little action thus far from health care leadership to address pay equity within the medical profession. In this article, we summarize evidence on the gender pay gap in medicine in Canada and abroad, and discuss common myths, likely root causes and possible solutions. We start with the premise that equal pay for equal work is a matter of fairness2 and is necessary for the profession to move from aspirations of gender inclusion to equity and justice for women.3 Gender is not binary; however, we focus on differences in pay between groups defined in the data as men and women. Currently, there is little research on the experiences of nonbinary physicians.4 In the broader Canadian workforce, the pay gap is larger for women who are Indigenous, racialized or newcomers, or are living with a disability.5 However, there are few comparable data in medicine,6 and discussing how the intersection of different identities may affect pay disparity is beyond the scope of this article.
Is the gender pay gap real?
Numerous studies, mostly from the United States and the United Kingdom, have shown a clear gender pay gap among physicians.7–13 This effect is seen in clinical,14 research15 and academic16,17 environments. Inequities start at the early stages of a medical career,18,19 deepen with time,20 continue into retirement21 and affect lifetime wealth,22 with estimates as high as $2.5 million over a 30-year career.23 The pay gap in medicine persists after adjustment for factors like physician age, specialty, number of hours worked and practice characteristics.24,25
The limited data available in Canada suggest a similar situation. The proportion of women among Canadian physicians has grown rapidly, from 11% in 1978 to 43% in 2018.26 Yet data from Ontario show that women account for only 8% of the province’s highest-billing physicians.27 Our own analysis of Canadian data, along with analysis done by others, suggest that some pay differences are driven by specialty but that there are also gender pay differences within specialties.
We used publicly available data to assess the relation between the proportion of women in a specialty and 1) the average gross payments by specialty across Canada and 2) the estimated net income by specialty (payments minus self-reported overhead) (see Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.200375/tab-related-content, for methods). Women made up less than 35% of physicians among 10 specialties with the highest gross and net incomes (Figure 1). In contrast, women accounted for 47%, 48% and 62% of physicians in the 3 specialties with the lowest estimated net income: family medicine, psychiatry and pediatrics. Other investigators have noted a trend in the feminization of specialties such as family medicine,28 and some have expressed concern that this represents a new “pink collar” tier of medicine that is relatively underpaid.29–31

(A) Scatterplot of the proportion of women in a specialty and the average gross payments per physician by specialty. (B) Scatterplot of the proportion of women in a specialty and the estimated average net income by specialty. Psychiatry includes geriatric psychiatry, child psychiatry and general psychiatry. Cardiac, cardiothoracic and thoracic surgery were combined into a single category. Pediatrics, internal medicine, and obstetrics and gynecology represent their general, but not subspecialty, categories.
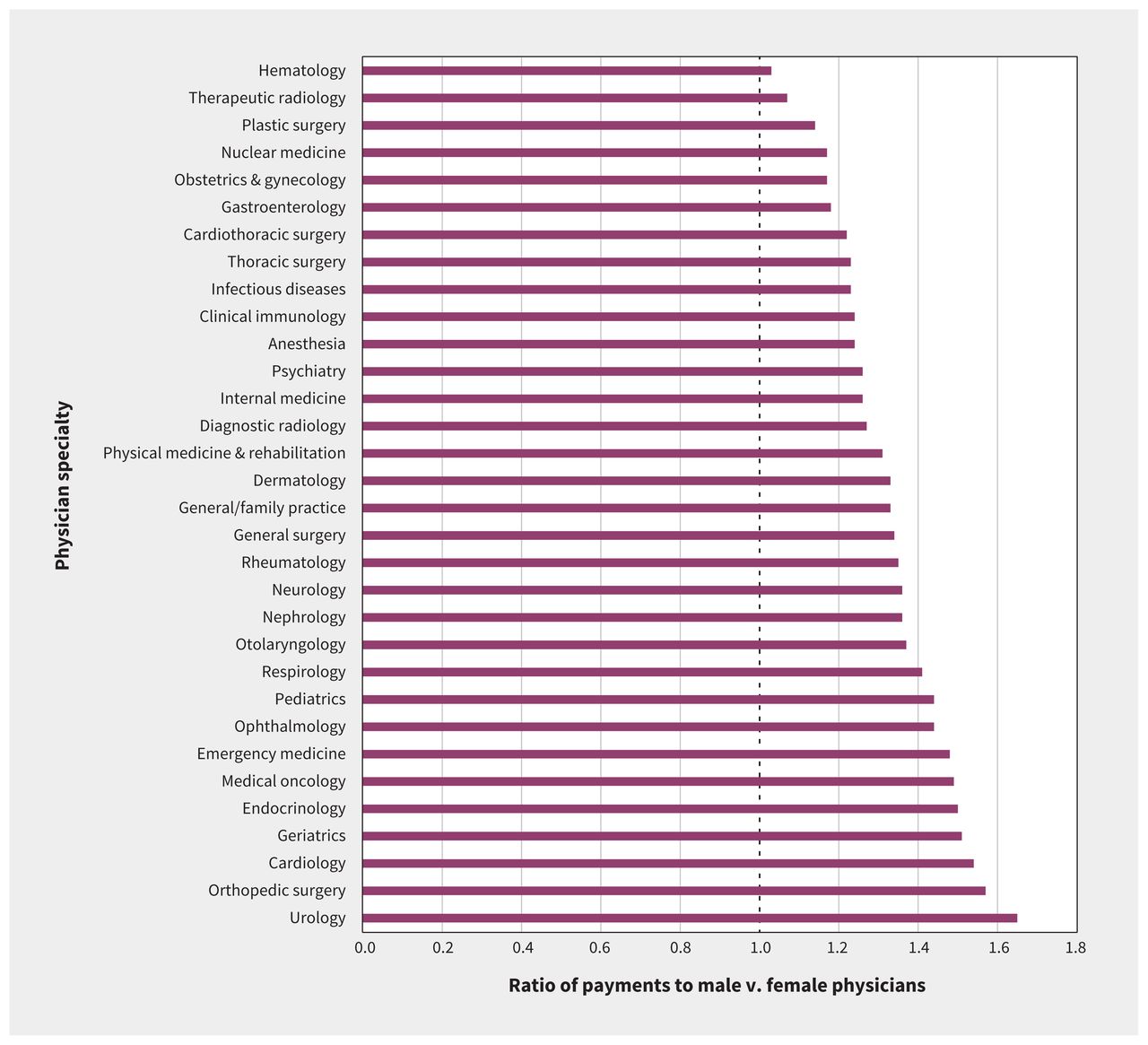
Recent Ontario analyses highlight the gender pay gap within specialties. An analysis of data from the Ontario Medical Association showed that, on average, male family physicians earn 30% more and male specialists earn 40% more than their female counterparts.32 Moreover, men earn more than women within every specialty (Figure 2). A more sophisticated cross-sectional analysis of billing data showed that female surgeons were paid less than male surgeons in Ontario even after adjustment for age, years in practice, patient factors and surgical specialty.33

Ratio of average gross fee-for-service payments to male versus female physicians in Ontario in 2016 by specialty. Only physicians billing more than $100 000 in payments are included in the analysis. A ratio of 1.0 denotes equality in gross fee-for-service payments between male and female physicians; a ratio greater than 1.0 denotes higher payments to males versus females. Data and analysis provided by Dr. Boris Kralj, Faculty of Social Sciences, McMaster University, based on Ontario Health Insurance Plan fee-for-service payments in 2016.
Do women just work less (or less efficiently) than men?
Most physician remuneration in Canada is based on a fee-for-service model, so it seems natural to presume that lower income is a result of women working less. However, the differences in work hours are not enough to fully explain the income gap. The Canadian Medical Association 2019 National Physician Survey (which included part-time and semiretired physicians) showed that, compared with men, women worked 4.7% fewer hours per week and 8.6% fewer hours on-call — small differences compared to the disparity in income.34 A study of primary care physicians in British Columbia in 2017 showed that women made 36% less than their male colleagues despite a patient care workload that differed by only 3.2 hours per week.35
Surveys of UK and US physicians showed that women were more likely to work part-time, but primarily if they had young children.36,37 Moreover, existing data suggest that having children results in a temporary decrease in work hours and that, over the course of their careers, women as a group do not work substantially less than men. A Canadian cohort analysis of general and family practitioners in 2008 showed a U-shaped curve in hours of direct patient care over the length of a woman’s career, declining until roughly age 38 and then increasing to previous levels, a pattern consistent with child-bearing and early-stage child-rearing.38 A study using American Medical Association data from 2010 to 2014 showed minimal gender difference in the retirement age of primary care physicians.39
Disparities in income likely relate more to the type of work women do compared to men than to work volume or efficiency. For example, Dossa and colleagues33 found that, between 2014 and 2016 in Ontario, female surgeons earned 24% less per hour spent operating than male surgeons. Across the 200 most common surgical procedures, there was no appreciable gender difference in time spent performing the procedure. Rather, women generally performed less lucrative procedures. The findings strongly suggest that, even when women work equal hours, they do not receive equal pay.
What are some of the root causes of the gender pay gap?
Women in medicine face discrimination throughout their careers. This discrimination is rooted in the history of women’s exclusion from the profession, along with the institutional legacies of sexism in medical schools, clinical care arrangements, health care organizations and the fee system itself. In the early stage of their careers, the “hidden curriculum” both subtly and overtly encourages women trainees to enter specific, often lower-paid, specialties.40–43 Once female physicians have graduated, they face subtle and often unconscious biases in recruitment and hiring.44 There are fewer women in medical leadership roles45,46 and of higher academic rank.47,48 Men in leadership benefit from the higher income associated with leadership and can also perpetuate the policies and informal support networks that recruit, retain and promote other men at disproportionately higher rates.49,50 Women in medicine are more likely to experience imposter syndrome and to have lower salary expectations than men,51 but this may result from the anchoring of expectations and feelings of self-worth that go along with lower starting salaries.52 Likewise, women see themselves as less capable of negotiating higher pay than men51 but are also more likely to experience consequences from trying to do so.53
Biases in clinical care arrangements also lead to pay inequity. A recent report from the UK showed that female general practitioners earn 35% less than male general practitioners.54 Age and hours worked were minor contributing factors. Rather, fewer women were in higher-paying partnership positions. Dossa and colleagues33 found a gender distribution in surgical cases to be the major driver of pay inequity between male and female surgeons. Female surgeons disproportionately operate in women,55 and these procedures are often remunerated at a lower level. For example, in Ontario, surgeons are paid $50.90 for incision under general anesthetic of a vulvar abscess, compared to $99 for a scrotal abscess. Similarly, payment for a biopsy is $39.60 for the penis and $26.85 for the vulva.56 That procedures performed mainly in female patients are lower paying is itself suggestive of systemic bias.57–60
Referral bias from primary care physicians also contributes to the gender pay gap in surgery. A 2017 study using US Medicare data showed that female surgeons received fewer referrals overall and that, if a patient had a poor outcome after surgery performed by a woman, his or her primary care physician was less likely to refer to any women in that specialty.61 However, if a poor outcome occurred at the hands of a male surgeon, an equivalent drop in referrals to men was not seen.
The type of work more likely to be performed by women in medicine is relatively undervalued, which contributes to gender pay disparities.62 In outpatient settings, women generally spend more time per patient and deal with more issues per visit than men, which leads to lower billing in a fee-for-service model.63,64 Moreover, patients expect women physicians to provide more emotional support.65,66 In primary care, women are more likely to address psychosocial issues and provide counselling, whereas men are more likely to deliver procedural services.67 Procedures generate more revenue per hour than nonprocedural, or “cognitive,” services.68 Indeed, most male-dominated, top-grossing specialties involve procedures, whereas female-dominated, lower-paid specialties are largely nonprocedural. Notably, men are overrepresented in medical professional associations and negotiation committees, which likely perpetuates these biases.56
Finally, the pay gap in medicine is influenced by broader societal attitudes toward women’s domestic roles. For example, survey data show that female physicians with young children spend more time doing domestic work than their male counterparts, even in dual-physician households.37,69–71 Independent of having children, simply living in a domestic partnership has been shown to have a gender effect on physician work hours, increasing the odds that a woman will work part-time but decreasing the odds of part-time work for men.72 Because of the disparities in domestic responsibilities, women with children face more obstacles to academic progression and slower self-perceived career advancement.73 These factors influence the proportion of women in leadership roles, which, in turn, affects not just income but also hiring and promotion.
What can we learn from other jurisdictions?
Most research on the gender pay gap in medicine comes from the US, where there is consistent inequity across a variety of remuneration models. In 2018, the American Medical Association adopted a multipronged policy to address the pay gap, including measures to identify disparities, push for pay structures based on gender-neutral criteria, advocate for training on implicit bias and implement routine gender-based pay audits.74 Research on interventions to address hiring and promotion inequities can provide useful outcome measures to guide policy development.75,76 For example, when policies addressing gender bias were implemented at the Stanford University School of Medicine, increases were seen in the representation, rank and job satisfaction of women in its faculty.77
Internationally, research shows a persistent gender pay gap, including in medical systems organized differently from the Canadian single-payer, mainly fee-for-service model. In the UK, physicians are salaried employees of the National Health Service, which should eliminate many of the time-related issues present in the Canadian billing model. Yet, since 2008, female physicians have consistently earned one-third less than their male colleagues.78 In 2017, legislation made it mandatory for the National Health Service to publish data on the gender pay gap, and the British Medical Association has committed to eliminating the pay gap. In 2018, the UK government commissioned a review of the gender pay gap in medicine that is expected to advise on strategies to resolve the gap.79
What can be done to close the gender pay gap in Canadian medicine?
Addressing the gender pay gap requires a multipronged approach (Box 1). Medical associations must commit to closing the pay gap. A recent report from the Canadian Medical Association acknowledging the need to correct the gender pay gap is an important step.80 However, progress will require accurate, transparent reporting on physician payment by specialty in Canada, stratified by gender, to better understand the current state and report on changes over time. Collection and reporting of data should move beyond a binary view of gender and also include information on race, country of origin and disability in order to understand how multiple forms of discrimination intersect and contribute to pay inequity.
| Action | Stakeholder | ||||
|---|---|---|---|---|---|
| Provincial/territorial governments | Professional associations | Faculties of medicine | Clinical leaders | Individual physicians | |
| Provide transparent aggregate data stratified by gender and other demographic characteristics | Transparent reporting of physician payments | Transparent reporting of salary support and promotion of physicians within an institution | Transparent reporting of physician income within a practice plan | Ask for data stratified by gender and demographic characteristics | |
| Provide antioppression training | Training for leadership and those on negotiation committees | Training for all faculty | Training for all clinical leaders | Act as role models by doing training | |
| Maintain standard, fair and transparent hiring and promotion practices | E.g., for physician leadership roles | E.g., for committees and executive | E.g, for new hires, salary support and promotion | Advocate for open, advertised competitions with transparent process | |
| Actively seek women for leadership roles | Gender representation on negotiation committees | Gender representation on negotiation committees, executive and board |
| Actively mentor and sponsor women | |
| Provide better maternity and parental leave programs | Improve maternity and parental benefit programs | Support colleagues who are taking maternity and parental leave | |||
| Other |
|
|
| Support women by sharing household labour more equitably | |
Addressing relativity within the medical profession has historically been fraught, but is an important path to closing the gender pay gap. The value of nonprocedural work, including counselling and psychosocial support, should be reflected in fee codes. Time modifiers or complexity add-on codes would more fairly compensate physicians who see patients with challenging conditions and spend more time per visit. There should not be a fee disparity between surgical procedures performed predominantly in women and equivalent procedures performed predominantly in men. Alternative payment models such as capitation and salary may avoid some of the inequities inherent in fee-for-service remuneration but would require careful implementation to prevent related pay inequities, as seen in the US and UK. Finally, medical associations and governments need to include more women on negotiating teams with a lens attuned to gender equity.
Leaders in medical school and clinical care need to expose and challenge gender bias in these settings. Medical schools should address the negative hidden curriculum, starting with faculty education.81–83 Female trainees should not be directed to enter “family-friendly” specialties, nor should they be warned away from male-dominated specialties or specialties with long hours or demanding physical work. More fundamentally, medical educators should apply a feminist critique to medical education and examine what is taught and whose voices are amplified.84
Clinical leaders should be encouraged to take antioppression training and address the institutional systems that perpetuate bias.85 Hiring processes should be transparent and formalized. Female candidates should be encouraged to apply for positions,86 and hiring committees should be diverse, with roughly equal numbers of women and men. Starting salaries should be standard and transparent, obviating the need for negotiation. Organizations should track and report on the gender pay gap within their institution and within leadership. Similarly, practice groups should share earnings internally with a view to gender pay equity. Men in leadership roles should not just mentor women but should also actively sponsor their careers.87 Physician groups should consider centralized, objective and transparent referral and triage systems to reduce the effects of referral bias.
Medical associations, government and health care organizations should develop programs and policies supporting everyone to take parental leaves, regardless of gender, and should adjust advancement criteria to account for such leaves. Partners need to support women in medicine by taking on a larger share of household labour.
Finally, work to address gender pay equity in medicine cannot be done in isolation. The medical profession should remain mindful of the relative privilege of physicians in society and support advances for women struggling in precarious, lower-paid work; solutions for the medical profession should not exacerbate broader societal income inequity. Efforts to close the gender pay gap in medicine should embrace efforts to measure and reduce pay gaps related to other intersecting forms of discrimination, including race and disability.
Conclusion
Women continue to be paid less than men in medicine. The gender pay gap exists within every specialty and also between specialties, with physicians in male-dominated specialties receiving higher payments. The gap is not explained by women working less but, rather, relates more to systemic bias in medical school, hiring, promotion, clinical care arrangements, mechanisms used to pay physicians and societal structures more broadly. Progress in Canada will require a commitment from medical associations and governments to close the pay gap, starting with transparent reporting of physician payments stratified by gender. We need to go further as a profession to understand how gender, race, disability and other identities intersect to affect gaps in pay and then take action to address these gaps to realize the vision of pay equity for all in medicine.
Acknowledgements
The authors thank Dr. Boris Kralj for sharing data from his research. They also thank Dr. Fahima Dossa, Dr. Ritika Goel, Dr. Irfan Dhalla, Dr. Nancy Baxter, Dr. Sharon Straus, Dr. Lesley Barron, Dr. Reena Pattani and Dr. Malika Sharma for reviewing the manuscript and providing feedback.
Footnotes
CMAJ Podcasts: author interview at https://www.cmaj.ca/lookup/doi/10.1503/cmaj.200375/tab-related-content
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Michelle Cohen conducted the data analysis and drafted the manuscript. Both authors conceived of and designed the work, revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Tara Kiran is the Fidani Chair in Improvement and Innovation at the University of Toronto. She is supported as a Clinician Scientist by the Department of Family and Community Medicine at the University of Toronto and at St. Michael’s Hospital. She is also supported by Health Quality Ontario and the Canadian Institutes of Health Research as an Embedded Clinician Researcher.
References
In this issue

Article tools



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Gender based disparities in Medicare physician reimbursement persist across years and specialty
- Eliminer les causes profondes de lecart salarial entre les sexes en medecine au Canada
- Addressing the root causes of the sex-based pay gap in medicine in Canada
- The impact of targeted fee increases on the pay disparity between female and male general surgeons in British Columbia
- Women in medicine--strength in leadership
- Ecart salarial entre les genres : le nombre dheures travaillees nest pas toujours le coupable
- Gender pay gap in medicine: not always an hours worked issue
- Diversite dans la haute hierarchie des organisations de sante au Canada: etude transversale sur la perception de la race et du genre
- Gender imbalance in gynecologic oncology authorship and impact of COVID-19 pandemic
- Physician variation in opioid prescribing: the importance of sex and gender
- Diversity among health care leaders in Canada: a cross-sectional study of perceived gender and race
- Gender-based differences in physician payments within the fee-for-service system in Ontario: a retrospective, cross-sectional study
- Promouvoir lequite entre les genres en medecine
- Advancing gender equity in medicine
More in this TOC Section
Similar Articles


Podcast