


Abstract
BACKGROUND: Reduced use of the emergency department during the COVID-19 pandemic may result in increased disease acuity when patients do seek health care services. We sought to evaluate emergency department visits for common abdominal and gynecologic conditions before and at the beginning of the pandemic to determine whether changes in emergency department attendance had serious consequences for patients.
METHODS: We conducted a population-based analysis using administrative data to evaluate the weekly rate of emergency department visits pre-COVID-19 (Jan. 1–Mar. 10, 2020) and during the beginning of the COVID-19 pandemic (Mar. 11–June 30, 2020), compared with a historical control period (Jan. 1–July 1, 2019). All residents of Ontario, Canada, presenting to the emergency department with appendicitis, cholecystitis, ectopic pregnancy or miscarriage were included. We evaluated weekly incidence rate ratios (IRRs) of emergency department visits, management strategies and clinical outcomes.
RESULTS: Across all study periods, 39 691 emergency department visits met inclusion criteria (40.2 % appendicitis, 32.1% miscarriage, 21.3% cholecystitis, 6.4% ectopic pregnancy). Baseline characteristics of patients presenting to the emergency department did not vary across study periods. After an initial reduction in emergency department visits, presentations for cholecystitis and ectopic pregnancy quickly returned to expected levels. However, presentations for appendicitis and miscarriage showed sustained reductions (IRR 0.61–0.80), with 1087 and 984 fewer visits, respectively, after the start of the pandemic, relative to 2019. Management strategies, complications and mortality rates were similar across study periods for all conditions.
INTERPRETATION: Although our study showed evidence of emergency department avoidance in Ontario during the first wave of the COVID-19 pandemic, no adverse consequences were evident. Emergency care and outcomes for patients were similar before and during the pandemic.
Avoidance of the emergency department for conditions that may require urgent surgery has been a global concern during the COVID-19 pandemic, and could result in higher case severity and morbidity.1–3 Resource constraints and provider concerns around the safety of surgery4–6 may influence rates of nonoperative management for abdominal and gynecological emergencies,7 even when existing nonoperative options are not optimal. Limited data suggest that patients with appendicitis and cholecystitis, the 2 most common abdominal emergencies that routinely require operative management,8,9 may be more likely to avoid the hospital,10 present with more severe illness9,10 and be managed nonoperatively during the pandemic, with uncertain consequences for patient outcomes.10–13 Similarly, the management of early pregnancy complications (i.e., miscarriage and ectopic pregnancy) may be medical or surgical, depending on patient preference and pregnancy characteristics (e.g., stability, gestational age).14 Up to 80% of women experiencing miscarriage routinely access emergency services; however, there are concerns that women requiring emergency care for miscarriages are avoiding the emergency department.15 Reduced access to emergency care for early pregnancy complications may result in more adverse outcomes; a study in Italy found an increased rate of ruptured ectopic pregnancy in the early months of the pandemic.16
We sought to characterize the impact of COVID-19 on emergency department visits for and management of appendicitis, cholecystitis, miscarriage and ectopic pregnancy. We aimed to determine if there was a difference in the rate of patients presenting to the emergency department before and during the pandemic, whether a reduction in emergency department visits for these conditions resulted in adverse patient outcomes and whether the proportion of patients undergoing operative management differed before and during the pandemic.
Methods
Study design and data sources
We conducted a population-based, repeat cross-sectional study of Ontario residents who presented to the emergency department with common abdominal or gynecological problems between Jan. 1, 2019–July 1, 2019, and Jan. 1, 2020–June 30, 2020. We used health administrative data held at ICES, which is authorized to collect and use health care data for the purposes of health system analysis, evaluation and decision support. Secure access to these data are governed by policies and procedures that are approved by the Information and Privacy Commissioner of Ontario. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.17
The Canadian Institute for Health Information National Ambulatory Care Reporting System captures demographic, diagnostic, procedural and discharge data for all emergency department visits in Ontario, Canada. The Discharge Abstract Database captures similar data for all acute care hospitalizations. The Registered Persons Database (RPDB) is a vital statistics registry that contains demographic data for all Ontario residents eligible for care under the Ontario Health Insurance Plan (OHIP), and captures date of death (in and out of hospital). We used RPDB eligibility files to determine population counts and person-weeks at risk. We used ICES-derived, validated cohorts to characterize patient comorbidities.18 We linked and analyzed data sets at ICES using unique encoded identifiers.
Study population
We identified residents of Ontario with a valid OHIP number who presented to the emergency department with appendicitis, cholecystitis, ectopic pregnancy or miscarriage between Jan. 1, 2019–July 1, 2019, and Jan. 1, 2020–June 30, 2020. We identified diagnoses using the main presenting diagnosis codes of the enhanced Canadian version of the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CA), restricted by age and sex, where appropriate (Appendix 1, Section A, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.202821/tab-related-content). We followed all patients for 30 days from the index emergency department visit up to July 31, 2020.
Outcomes
Our primary outcome was weekly rates of emergency department visits per 100 000 person-weeks. For each condition and each week of the study period, we calculated the number of days at risk for emergency department visits for all OHIP-eligible people, restricted by age and sex as per Appendix 1, Section A. We divided the sum of the days at risk by 7 to obtain total person-weeks at risk for a given week and condition. If a patient was admitted to hospital for any condition, we did not include the duration of the hospital stay in days at risk.
We used Mar. 11, 2020, the date of the first reported death from COVID-19 in Ontario, to define the start of the COVID-19 period. We calculated weekly rates of emergency department visits in the pre-COVID-19 (Jan. 1, 2020–Mar. 10, 2020, week 1 to 10) and COVID-19 (Mar. 11, 2020–June 30, 2020, week 11 to 26) periods and compared these with an equivalent week in an historical control period (Jan. 1, 2019–July 1, 2019) to account for seasonal trends.
For each patient presenting to the emergency department, we ascertained patient characteristics (age, sex, neighbourhood income quintile,19 rurality,20 comorbidities), time of presentation (regular hours [weekdays from 7:00 to 17:00], after hours [weekdays 17:00–7:00] and weekend [Saturday, Sunday, statutory holidays]) and hospitalization after the index emergency department visit. We also identified management strategies using the Canadian Classification of Health Interventions, including diagnostically relevant surgical and interventional radiological procedures (e.g., abdominal abscess drain), surgical approaches (laparoscopic v. open) and medical management of miscarriage and ectopic pregnancy (e.g., antibiotics, misoprostol, or expectant management) (Appendix 1, Section B).
We ascertained total length of stay in hospital, repeat visits to the emergency department, hospital readmission, complications and deaths for all patients. We evaluated all secondary outcomes within 30 days of index emergency department visit. We defined length of stay as the total number of days in hospital from index visit, including readmissions, if any. We captured repeat emergency department visits and hospital readmissions for the same diagnosis. We defined complications based on the National Surgical Quality Improvement Program,21 as well as specific maternal morbidity indicators relevant to early pregnancy complications (Appendix 1, Section C).22–25
Statistical analysis
We used incidence rate ratios (IRRs) to compare the weekly rate of emergency department visits per 100 000 person-weeks in the historical control period with the corresponding weekly rate of emergency department visits in the pre-COVID-19 and COVID-19 periods (e.g., the first week in the pre-COVID-19 period was compared with the corresponding week in 2019). We calculated Wald-based 95% confidence intervals for IRRs assuming independent Poisson rates (2-sided, α = 0.05).26 An IRR with an upper confidence limit less than 1 denotes a statistically significant reduction in weekly emergency department visits. We compared baseline characteristics between equivalent time periods (e.g., weeks 1–10 in the pre-COVID-19 period v. weeks 1–10 in the 2019 control period) using the standardized difference. Standardized differences of < 10% represent a minimal imbalance between periods.27 We compared secondary outcomes between equivalent time periods using the χ2 test and the Kruskal–Wallis nonparametric test, where appropriate.
Ethics approval
ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from review of research ethics boards. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Results
A total of 39 691 emergency department visits occurred during the 2019 and 2020 study periods, including 15 964 (40.2%) visits for appendicitis, 12 733 (32.1%) visits for miscarriage, 8457 (21.3%) visits for cholecystitis and 2537 (6.4%) visits for ectopic pregnancy. The weekly number of patients presenting to the emergency department in the pre-COVID-19 period was similar to the equivalent weeks in the historical control period, across all conditions. However, the start of the COVID-19 period was accompanied by a decrease in weekly emergency department visits compared with equivalent weeks in the historical control period. Weekly relative rates are presented in Figure 1, and absolute differences in rates of emergency department visits are presented in Appendix 1, Section D.
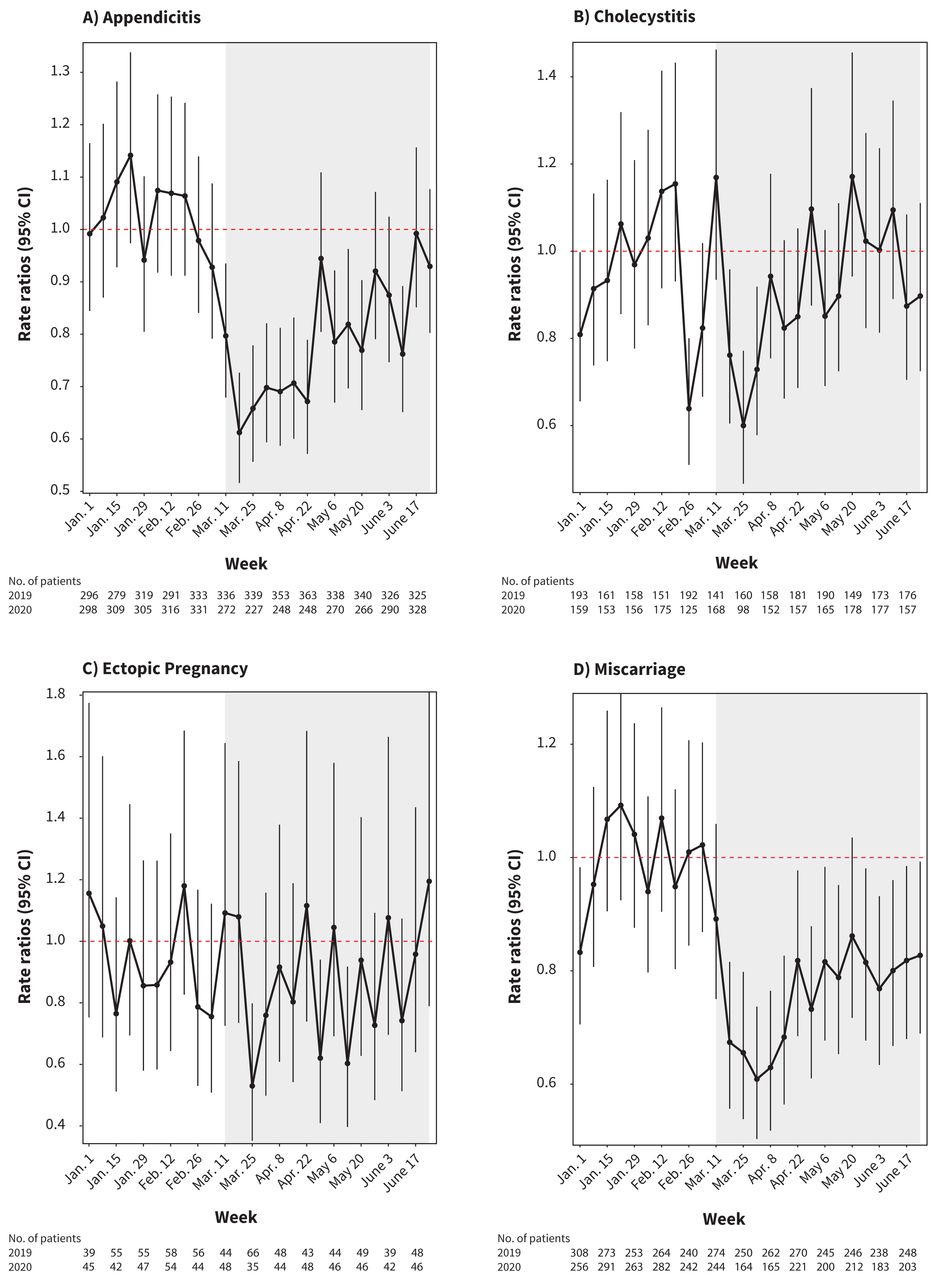
Incidence rate ratios (95% confidence intervals [CIs]) comparing the rate of weekly emergency department (ED) visits for (A) appendicitis, (B) cholecystitis, (C) ectopic pregnancy and (D) miscarriage per 100 000 person-weeks in the pre-COVID-19 (Jan. 1, 2020–Mar. 10, 2020, week 1–10) and COVID-19 periods (Mar. 11, 2020–June 30, 2020, week 11–26) with the weekly rate of ED visits per 100 000 person-weeks in the historical control period (Jan. 1, 2019–July 1, 2019). Note: The COVID-19 period is shaded in grey. An incidence rate ratio where the upper confidence limit of the 95% CI is below 1 (dashed red line) denotes a statistically significant reduction in weekly ED visits compared with the equivalent week in 2019. Conversely, an incidence rate ratio where the lower confidence limit is above 1 denotes a statistically significant increase in weekly ED visits compared with the equivalent week in 2019.
The rate of patients presenting to the emergency department for appendicitis and miscarriage showed sharp, sustained decreases in the COVID-19 period. Weekly IRRs for both appendicitis and miscarriage ranged from 0.61 to 0.80 during the COVID-19 period compared with the corresponding week in the previous year, indicating a 20%–39% reduction in emergency department visits. Emergency department visits for appendicitis were below expected volumes for 11 of the 16 weeks of the COVID-19 period, with an absolute decrease of 1087 visits. The absolute difference in the weekly rate of emergency department visits for appendicitis ranged from −0.81 to −0.18 per 100 000 person weeks. Emergency department visits for miscarriage during the COVID-19 period were below expected volumes for 14 of the 16 weeks. Overall, 984 fewer patients presented to the emergency department with a miscarriage during the COVID-19 period compared with the equivalent period of the historical control. The absolute difference in the weekly rate of emergency department visits for miscarriage ranged from −3.1 to −1.3 per 100 000 person weeks.
Visits to the emergency department for cholecystitis showed an initial decrease in the COVID-19 period, with weekly IRRs that ranged from 0.60 to 0.76 for 3 weeks; however, emergency department visits returned to expected volumes after week 5 of the COVID-19 period. Visits for ectopic pregnancy were below expected volumes for 3 nonconsecutive weeks of the 16-week COVID-19 period, with IRRs ranging from 0.53 to 0.60 during those weeks versus the historical control period. There was no subsequent increase in emergency department visits for cholecystitis or ectopic pregnancy above expected volumes; weekly emergency department visits remained consistent with the historical control period for the remainder of the pandemic period.
Baseline characteristics of patients presenting to the emergency department were similar between study periods, both overall (Table 1) and by condition (Appendix 1, Section E). Over the entire study period, 52.1% (n = 20 831) of patients were admitted to hospital; admission rates varied by condition, from 80.1% (n = 12 793) for appendicitis to 34.2% (n = 868) for miscarriage. Similarly, although 48.4% (n = 19 208) of patients received an intervention (surgical or image-guided), the proportion receiving an intervention varied from 76.2% (n = 12 167) of patients with appendicitis, to 37% (n = 949) of patients experiencing a miscarriage. The overall mortality rate was 0.24% (0.12% for patients with appendicitis, 0.91% for patients with cholecystitis); at 30 days, no patients with ectopic pregnancy or miscarriage had died.
Baseline characteristics of patients presenting to the emergency department for appendicitis, cholecystitis, ectopic pregnancy or miscarriage in Ontario
We did not observe any differences across study periods in rates of hospitalization after the index visit to the emergency department, in frequency or type of interventions (i.e., open v. laparoscopic), in repeat visits to the emergency department, in hospital readmission, in total length of stay, in complications or in mortality rates for any of the conditions (Table 2). In addition, there were no differences in outcomes when the first 6 weeks of the COVID-19 period were compared with the equivalent period in the historical control. A slight increase in interventions was seen in all 2020 compared with 2019 for both the pre-COVID-19 and COVID-19 periods.
Outcomes of patients presenting to the emergency department for appendicitis, cholecystitis, ectopic pregnancy or miscarriage in Ontario
Interpretation
In this population-based study, we observed an initial reduction in emergency department visits for appendicitis, miscarriage, cholecystitis and ectopic pregnancy during the first wave of the COVID-19 pandemic in Ontario. Following the initial drop, visits for cholecystitis and ectopic pregnancy quickly returned to expected levels, but emergency department visits for appendicitis and miscarriage showed sustained reductions. We did not identify any change in patient management; specifically, we did not observe an increase in the number of patients managed medically rather than surgically. We also did not observe a difference in the proportion of surgically managed patients undergoing laparoscopic compared with open procedures, or undergoing image-guided techniques such as percutaneous drains. Importantly, in spite of the sustained decrease in emergency department visits for appendicitis and miscarriage, no increase in adverse patient outcomes was observed during the study period. Patients did not appear to present with higher acuity or suffer higher morbidity. Similar management strategies were used throughout the study periods, and case morbidity was unchanged, as evidenced by similar rates of hospitalization, length of stay, repeat emergency department visits and complications. Our findings are reassuring, suggesting that patients with these common conditions who needed emergency care at the beginning of the pandemic continued to present to hospital in spite of overall decreased rates of emergency department visits.
Decreased emergency department attendance during the pandemic has been explained by 2 hypotheses: underusage of the emergency department, and a true reduction in acute pathologies.28 Our study suggests a third possibility: potential over-usage of the emergency department before the pandemic. Avoidance of the emergency department during the pandemic may have resulted in miscarriages being managed through outpatient or virtual clinics without an emergency department visit. For some patients with mild symptoms of uncomplicated appendicitis, their symptoms may have resolved without presenting to the emergency department or they may have used virtual visits for conservative management. We did not observe any rebound increases in case volumes or case severity, which supports this hypothesis.29 After the initial weeks of the pandemic, it is also possible that the reduction in emergency department visits for miscarriage occurred because of reduced incidence of miscarriage, reduced natural conceptions30 or limited access to reproductive endocrinology services.31 However, as no change was seen in visits for ectopic pregnancy, fewer pregnancies is an unlikely explanation. Similarly, it is plausible that some reductions in appendicitis occurred in parallel with diminished air pollution32,33 or reductions in infectious causes given increased attention to hygiene,34 although these factors are unlikely to account for the magnitude of the observed difference.
Limited literature provides insight into whether lower rates of emergency department attendance at the beginning of the pandemic had serious consequences for patients. Observational studies in the United States found a reduction of 39%–64% in all emergency department visits and admissions early in the pandemic,2,35–37 but did not specifically evaluate for consequent increased case severity. Our population-based findings further strengthen earlier reports that suggested a decrease in emergency department volumes without an associated increase in case severity.38,39 Although there was a drop in emergency department attendance for these common abdominal and gynecological conditions, the provision of emergency services was maintained for the patients who required them. These observations have direct relevance to the maintenance of care in future waves of the pandemic. Telemedicine, which became widely available early in the pandemic, may facilitate safe delivery of care outside the emergency department for certain conditions or may be used as part of a pre-emergency department triage strategy.40,41 Public messaging around the importance of seeking emergency care when needed during the pandemic should be accompanied by information on alternative options, particularly services that may be accessed after hours. Digital clinical algorithms and chatbots may also be explored for initial management of common conditions before involvement of a clinician, similar to the use of artificial intelligence in triaging patients with COVID-19 who require emergency care.42
Limitations
Although we were able to capture all emergency department visits at Ontario hospitals, allowing comprehensive follow-up for each patient, our study has some limitations. We compared volumes before and during the pandemic to a 2019 historical control period, but cannot verify whether a true reduction in the incidence of acute pathology occurred; however, given the nature of the conditions of interest, it is unlikely that the magnitude of the reduction in emergency department visits reflects only a change in incidence. We did not observe an increase in case morbidity, but were limited in our ability to capture some outcomes. For example, we were unable to differentiate between ruptured and stable ectopic pregnancies. Reassuringly, no temporal pattern was observed for ectopic pregnancy and we did not observe an increase in other important outcomes, such the need for blood transfusion or surgery. Similarly, we were unable to capture the severity of cholecystitis or appendicitis, though there was no increase in the use of percutaneous drains. Finally, our study window might not have captured all rebound presentations or adverse outcomes. However, all patients were followed for 30 days from their index emergency department visit, and given the acute nature of these conditions, most events should have been captured.
Conclusion
During the first wave of the COVID-19 pandemic in Ontario, a sharp and sustained initial drop in emergency department visits was seen for common abdominal and gynecological emergencies. We did not observe any resultant increase in patient morbidity for these conditions. These findings are reassuring, as patients who required emergency care in the first wave of the pandemic continued to present to the emergency department, received similar care and had similar outcomes to patients presenting in the prepandemic period.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: David Gomez and Andrea Simpson conceived and designed the study. Andrew Wilton acquried the data, which all authors analyzed and interpreted. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by the Ontario Health Data Platform, as well as a foundation grant (148470) from the Canadian Institutes of Health Research (Nancy Baxter). Colin Sue-Chue-Lam is supported by a Ministry of Health Clinician Investigator Program Award. Dr. Austin is supported by a Mid-Career Investigator Award from the Heart and Stroke Foundation.
Data sharing: The data set from this study is held securely in coded form at ICES. Although legal data sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
- Accepted April 14, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Hospital admission from the emergency department for selected emergent diagnoses during the first year of the COVID-19 pandemic in Ontario: a retrospective population-based study
- Changes in emergency department use in British Columbia, Canada, during the first 3 years of the COVID-19 pandemic
- Visits to the emergency department by community-dwelling people with dementia during the first 2 waves of the COVID-19 pandemic in Ontario: a repeated cross-sectional analysis
- To Fight or to Flee? A Systematic Review of Ectopic Pregnancy Management and Complications During the Covid-19 Pandemic
- Changes in ischemic stroke presentations, management and outcomes during the first year of the COVID-19 pandemic in Alberta: a population study
- Changes in ischemic stroke presentations and associated workflow during the first wave of the COVID-19 pandemic: A population study in Alberta, Canada
More in this TOC Section
Similar Articles
Collections

