


Clinical and outbreak management platforms have been essential tools during the COVID-19 pandemic, but expanded surveillance systems are needed to support effective and equitable public health policy-making and response efforts now and in the future.
A dynamic surveillance system encompassing waste-water testing, representative population-based testing and genomics should be implemented to efficiently monitor pan-respiratory disease trends, rapidly detect resurgences and emergence of novel variants, and respond with tailored and effective public health programs.
The funding and resources necessary to develop, initiate and sustain expanded surveillance systems will be substantial, but critical public health gains will include reducing morbidity and mortality, mitigating economic impact and decreasing societal disruption through public health action, policy decisions and programming.
Multidisciplinary implementation actors should ensure that participation, community engagement and data justice are embedded in the surveillance systems.
Infectious disease surveillance is fundamental to public health systems.1 However, Canada’s COVID-19 pandemic response relied on clinical and outbreak management (COM) platforms; i.e., public health institutions tracking case counts across a range of reasons for testing (e.g., symptoms) or screening (e.g., exposure, routine screening for health care workers).2 Although important for clinical care and providing broad COVID-19 population health metrics and trends, these COM platforms were not designed for infectious disease surveillance and have important limitations.2
We propose a tiered surveillance approach that encompasses waste-water testing, representative population-based testing (including data on potential transmission mechanisms; e.g., social determinants of health) and genomics to efficiently monitor disease trends, and rapidly detect resurgences and emergence of novel variants or strains. This information is crucial to inform the development of tailored and effective public health programs. The proposed system could, and ultimately should, be expanded beyond COVID-19 to support pan-respiratory pathogen surveillance.
Why does relying strictly on COM platforms limit a public health response?
The objectives of COM testing platforms are to support clinical care (e.g., patient diagnosis, determining appropriate treatment) and public health case and contact tracing (e.g., testing exposed individuals to determine isolation needs).3 Although these platforms are not intended for surveillance purposes, many jurisdictions have used them as ad hoc surveillance systems during the COVID-19 pandemic.2 However, the utility of these data are limited by biases due to changing case definitions and testing criteria over time and across jurisdictions, a lack of standardization to account for differences in the populations being tested, and inadequate capture of mild or asymptomatic infections.2,4
Long-term reliance on COM platforms creates challenges for public health response as a result of undercounting of cases, selection biases from health care–seeking behaviours, lagging epidemiological indicators and unmanageable case volumes.5 For instance, clinical platforms typically conduct diagnostic testing among symptomatic individuals and are therefore likely to miss individuals who do not seek testing owing to asymptomatic or mild illness, leading to an underestimation of community disease burden.6 Prevailing inequities in health care for marginalized and lower-income communities — such as lower access to and utilization of health care services — contribute to underestimating disease burden in these populations.7,8 Further, data on hospital admissions capture only severe cases, and because patients may present later in their course of illness, they are a lagging indicator of community transmission.9 Together, these limitations compromise effective and equitable policy-making.
What information do different surveillance systems provide to support public health decision-making?
Surveillance systems offering opportunities to move beyond COM platforms include waste-water, syndromic, sentinel and population-based surveillance.
Waste-water surveillance is a relatively low-cost, innovative method in which routine testing of waste-water samples provides early signals of changes in pathogen trends at the population level.10,11 Genomic sequencing of waste-water samples can be conducted to enable early detection of novel viral variants or strains.11 Because waste-water surveillance does not rely on health system interaction, it is not biased by health care–seeking behaviour. However, although these data can be analyzed at area levels (e.g., neighbourhoods), data cannot be linked to individual sociodemographic factors or immunization status. Therefore, they cannot identify who in the population is becoming infected or provide indicators of severity or immune escape properties for novel variants. Further, despite the rapid development of waste-water surveillance infrastructure as pilot projects for COVID-19, there remains an urban bias in implementation sites as jurisdictions continue to transition to sustainable widespread programs.10
Syndromic surveillance collects information on relevant symptoms (e.g., cough, fever) to provide early signals of changing disease dynamics in the population without relying on laboratory confirmation.12 Syndromic data can be generated through direct collection from patients (e.g., health care settings, telehealth platforms, and Web or mobile applications),13,14 pharmaceutical sales of relevant over-the-counter medications (e.g., antipyretics),15 or automated data streams such as search engine queries (e.g., Google Trends).16 However, the broad range and overlap in symptoms across many respiratory diseases means that syndromic data alone have limited diagnostic accuracy in identifying pathogen-specific trends for health care resource planning.17 Another key issue with syndromic data are population representativeness, particularly for data collected by Web or mobile applications.18 Further, not all syndromic surveillance data streams include associated individual-level sociodemographic factors, which, like waste-water surveillance, limits our understanding of who is infected.
Health care–based sentinel surveillance is commonly used for monitoring respiratory pathogens by systematically sampling in health care settings (e.g., hospital wards, emergency departments, physician offices) to determine circulating pathogens and relative disease trends over time and across locations. 5 Surveillance case-reporting forms can provide detailed individual-level sociodemographic information on tests conducted for multiple pathogens (e.g., SARS-CoV-2, influenza, respiratory syncytial virus) and samples can be sequenced to determine circulation of new variants, and whether their clinical severity profiles warrant classification as variants of concern. However, as with existing clinical platforms, health care–based sentinel surveillance is biased by health care–seeking behaviour, is less generalizable outside of urban centres19 and likely underestimates disease burden among asymptomatic and mild cases, which is critical for understanding transmission dynamics of emerging pathogens.5
Population-based surveillance using repeated random sampling is a valuable option for estimating community disease burden and monitoring temporal trends. In these systems, individuals are sampled independently of their health care–seeking behaviours or symptom status, which provides a more accurate picture of community burden across the clinical and social spectrum. Similar to sentinel systems, population-based surveillance can provide detailed individual-level information including mechanistic risk factors for transmission, such as social determinants of health and race-based data;20 samples can be sequenced to determine circulation and severity of new variants; and the sampling frame can be leveraged for multiple pathogens. Modifications implemented in the design and analysis stages, such as oversampling of specific population groups, can also enable robust estimation of health outcomes and better inform equitable policy decisions.21 Although a representative population-based system provides the most robust information for decision-making, it does require substantial financial investment with survey design considerations implemented a priori to ensure adequate response rates and population representativeness.
What can we learn from the international experience?
Although many global jurisdictions have used patchwork clinical data streams based on COM platforms to monitor COVID-19 trends,3,5 selected jurisdictions have implemented robust population-based surveillance systems.
For instance, in 2020 Slovakia conducted multiple rounds of mass population-wide rapid antigen testing as a public health intervention to better understand community transmission and identify and reduce sources of transmission.22 Although this initiative may provide robust population prevalence estimates, its financial and laboratory resource-intensity is not sustainable in the long term.
The United Kingdom has employed 2 population-based surveillance systems using repeated random sampling: the Coronavirus Infection Survey (CIS) and the Real-time Assessment of Community Transmission (REACT).23,24 The CIS samples more than 100 000 individuals across the UK twice a month, with sampling permitted to vary proportionately across regions, occupations and ethnic groups to estimate subpopulation trends.23 During the Omicron surge, these systems identified a higher pediatric COVID-19 burden than that reported in previous waves and a persistent disproportionate burden among ethnic minority populations and those residing in lower-income neighbourhoods. 25 Results were made available in real time to support policy response and guide individual decision-making. These systems are a bedrock of the UK COVID-19 response and require substantial and sustainable investment.26
Waste-water surveillance has been successfully implemented in several settings, including Alberta, Yellowknife and Ontario, Canada; Dhaka, Bangladesh; and Rotterdam, Netherlands. 10,11,27 In Rotterdam, waste-water testing was performed 3 times a week at 9 sites. Results from waste-water testing provided a 6-day lead time on viral resurgence and identified postal codes with higher SARS-CoV-2 viral activity in waste water than by clinical testing; this information was used to add mobile testing locations and improve access in underrepresented areas.10 Although waste-water testing provides actionable results, it requires strong collaboration between public health and environmental ministries for implementation, data analysis and interpretation.10
What could a national surveillance system look like in Canada?
To enable Canada’s health systems to effectively prepare for — and efficiently respond to — infectious disease threats, a national surveillance system should be based on 4 key surveillance principles: population-representative disease detection based on standardized reporting; real-time data availability for use and interpretation; nimble platforms adaptive to changing epidemic dynamics; and platforms designed and implemented with engagement and leadership by communities disproportionately affected, to ensure that guiding principles of public health (i.e., participation, equity and social justice) are embedded.28,29
A dynamic, efficient and representative surveillance strategy using a tiered approach
An efficient and responsive national respiratory pathogen surveillance system should comprise 3 complementary tiers: wastewater testing, representative population-based testing and genomics (Figure 1).
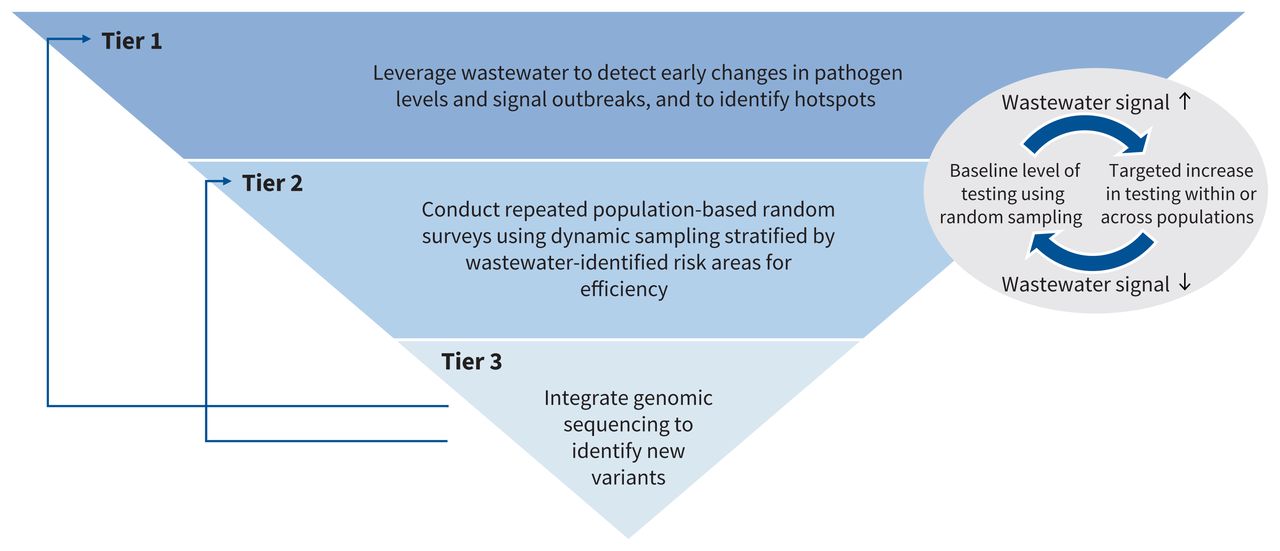
Tiered surveillance strategy encompassing waste-water testing, dynamic representative population-based testing and genomics.
The first tier tracks disease signals by testing samples from centralized waste-water facilities, to enable early detection of pathogen resurgence and epidemics. This requires collaboration across public health and environmental ministries, with coordinated data flow and standardized analytic and reporting methods to enable comparisons across jurisdictions.11
The second tier consists of representative population-based surveillance using mailed sample collection kits, paired with online surveys, to randomly selected households across Canada and among key population groups (e.g., underhoused individuals, long-term care homes and incarcerated populations) to understand the sociodemographic composition of populations being infected, particularly in regions with strong waste-water signals. Public health institutions should collaborate with groups with statistical expertise (e.g., Statistics Canada) to determine an appropriate sampling strategy and the baseline number of samples needed to produce robust population estimates that are representative at local, provincial and territorial, and federal levels. Leveraging insights from waste-water signals, the sampling scheme should be dynamic, with clear triggers to activate proportionate testing increases in regions or subgroups with increasing pathogen levels, thereby enabling more efficient sampling and better insight into transmission dynamics.
The third tier consists of genomic sequencing on a representative subset of samples from each data stream. Sequencing of waste-water samples can provide insight into the emergence of variants and their relative levels of circulation, whereas sequencing of population samples allows for analysis of variant severity, immune escape properties and transmission advantage. This could be implemented through collaborations between public health laboratories at federal and provincial and territorial levels.
The proposed tiered system provides an integrated approach to support adaptive responses to emerging respiratory pathogens using existing infrastructure, enabling unbiased estimates of incidence and prevalence over time and across geographical regions and subpopulations to inform public health response.
Implementation considerations: participation, community engagement and data justice
Although surveillance implementation requires coordinated efforts across jurisdictions and substantial sustained financial resources, returns on investment will be achieved by reducing morbidity and mortality, mitigating economic impact and decreasing societal disruption through public health response.30 The proposed system could be implemented at several levels, from regional to provincial and territorial to federal. A multitiered surveillance system knitted together by intergovernmental agreements and harmonized data structure and regulation has previously been recommended;28 this remains relevant and is critical for successful implementation of new systems.
Careful consideration should be given to data governance, including harmonization across local, federal, and provincial and territorial levels, while ensuring data justice with regard to Indigenous self-determination and sovereignty is embedded. Implementation actors should cross public health, microbiology and environmental domains, along with community-led leadership roles, which will be vital in ensuring population engagement and acceptance. Furthermore, implementation at all levels must include and be guided by meaningful engagement of communities disproportionately affected by the infectious diseases the system is monitoring.
Enabling decision-making based on surveillance
To enable timely insights and inform evidence-based, equitable and responsive public health measures, surveillance data must be made available to the public health community and the general public in real time. Open-access real-time reporting needs to be matched with improved communication and data visualizations; this could include updated analytics and reports shared with all stakeholders and the public on a regular basis. Clear messaging from public health and community leaders on how surveillance indicators are being used to inform policy is critical.30 Evaluations of surveillance programs must include not only the costs but also the benefits for population health and societal function.31
Benefits of surveillance now and areas for future expansion
Initiating this surveillance system for SARS-CoV-2 provides a baseline understanding of the changing COVID-19 epidemiological situation to inform a tailored public health response — including updated vaccination strategies — across Canada. In the longer term, the proposed infrastructure should be leveraged for multiple pathogens to support panrespiratory pathogen surveillance. Waste-water methods can detect a variety of respiratory and nonrespiratory pathogens, including — but not limited to — adenoviruses, enteroviruses, influenzas, noroviruses and poliovirus. 32 Innovations in multiplex polymerase chain reaction–based assays could support the use of several primer pairs in a single reaction, and advancements in batch and pooled testing could lower costs and improve system efficiency.33 However, additional considerations should be given to detection probability and appropriate thresholds for triggering subsequent tiers for different target pathogens.
The tiered approach can also be expanded to include zoonotic surveillance, such as for SARS-CoV-2 and influenza. Harmonization between human and animal health agencies using a One Health approach could enable early identification of novel pathogens or viral variants and potential animal-tohuman transmission.34 Expanded tiers to support early detection of novel pathogens could also include cross-border coordination and systematic testing of travellers or residents entering the country.35 Finally, other data streams, including COM platforms, can be integrated into the tiered system to inform public health response.
Conclusion
Strengthening surveillance in Canada remains critical. Although COM platforms are essential for clinical care and contact tracing, robust population-based surveillance systems can better provide actionable data on community transmission of SARS-CoV-2 and other emerging and re-emerging respiratory pathogens to inform proactive and equitable public health policy.
Acknowledgement
The authors thank Dr. Ashleigh Tuite for helpful discussions on this topic and manuscript.
Footnotes
Competing interests: Beate Sander reports receiving funding from the Ministry of Colleges and Universities as Principal Investigator of a COVID-19 Rapid Research Fund. Until March 2022, Dr. Sander served as co-chair of the Ontario COVID-19 Modelling Consensus Table. Sarah Buchan reports being the co-investigator on grants to support COVID-19 epidemiology and immunization-related research funded by the Canadian Institutes of Health Research (CIHR) and the Public Health Agency of Canada (PHAC). Jeffrey Kwong reports receiving grants to support COVID-19 epidemiology and immunization-related research funded by CIHR and PHAC. Dr. Kwong has also received a University of Toronto Department of Family and Community Medicine Clinician-Scientist Award. Sharmistha Mishra reports receiving grants to support COVID-19 epidemiology and modelling research funded by CIHR. Dr. Mishra is also a member of the Ontario COVID-19 Modelling Consensus Table and is funded by a Tier 2 Canada Research Chair in Mathematical Modelling and Program Science. Laura Rosella is funded by a Canada Research Chair in Population Health Analytics and the Stephen Family Chair in Community Health, Trillium Health Partners Foundation. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work. Isha Berry and Beate Sander drafted the manuscript. All authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This research was supported, in part, by a Canada Research Chair in Economics of Infectious Diseases held by Beate Sander (CRC-950-232429).
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue
{kind=link}
Article tools



Jump to section
- Article
- Why does relying strictly on COM platforms limit a public health response?
- What information do different surveillance systems provide to support public health decision-making?
- What can we learn from the international experience?
- What could a national surveillance system look like in Canada?
- Acknowledgement
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

