


Article Figures & Tables
Figures
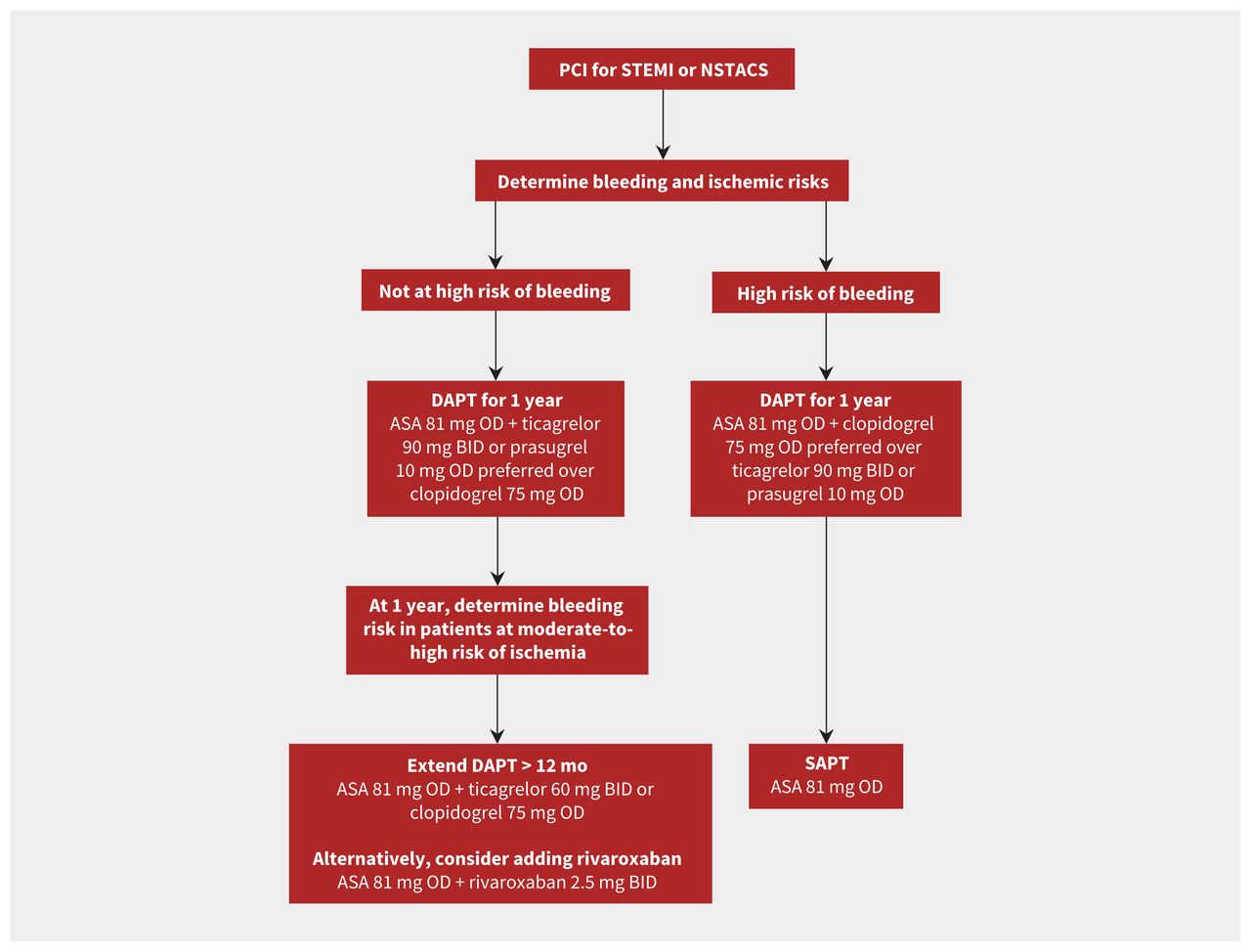
- Figure 1:
Antiplatelet recommendations in patients with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention (PCI). Note: ASA = acetylsalicylic acid, BID = twice daily, DAPT = dual antiplatelet therapy, NSTACS = non-ST segment elevation acute coronary syndrome, OD = once daily, SAPT = single antiplatelet therapy, STEMI = ST-segment elevation myocardial infarction.
- Figure 2:
Antiplatelet management in patients with acute coronary syndrome (ACS) and atrial fibrillation (AF). Direct oral anticoagulation (DOAC) is preferred over warfarin; however, if warfarin is to be used the recommended international normalized ratio target is 2.0–2.5. The timing of when to discontinue acetylsalicyclic acid (ASA) will depend on the individual patient’s ischemic and bleeding risk. Note: PCI = percutaneous coronary intervention.
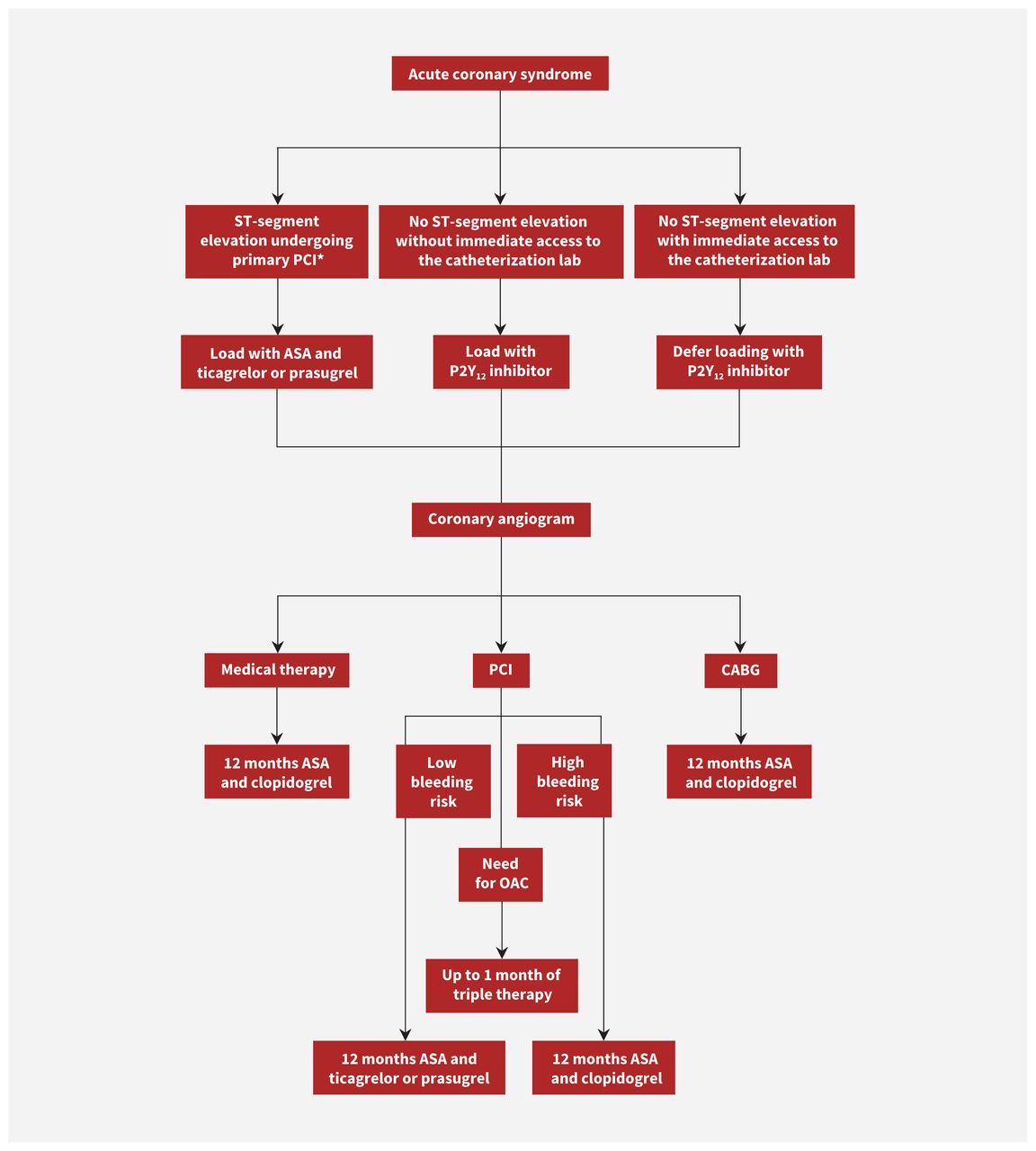
- Figure 3:
Flowchart for antiplatelet management in patients with acute coronary syndrome. Note: ASA = acetylsalicylic acid, CABG = coronary artery bypass grafting, OAC = oral anticoagulant, PCI = percutaneous coronary intervention. *Patients receiving fibrinolytic therapy should be loaded with ASA and clopidogrel. Switching to ticagrelor within 24 hours should be considered.


Tables
- Table 1:
Relative difference in ischemic and bleeding risks* among different P2Y12 inhibitors (16)
Drugs compared No. of studies (no. of patients) Ischemic risk Bleeding risk Ticagrelor v. clopidogrel 6 RCTs (21 828)† Ticagrelor associated with 18% reduction in cardiovascular mortality, 28% reduction in stent thrombosis and no difference in MI Ticagrelor associated with 27% increase in major bleeding Prasugrel v. clopidogrel 4 RCTs (25 740) Prasugrel associated with 10% reduction in cardiovascular mortality (95% CI 0.80–1.01), 50% reduction in stent thrombosis and 19% reduction in MI Prasugrel associated with 26% increase in major bleeding Prasugrel v. ticagrelor 2 RCTs (5248) Prasugrel associated with 32% reduction in stent thrombosis and no difference in cardiovascular mortality or MI No difference in major bleeding Note: CI = confidence interval, RCT = randomized controlled trial, MI = myocardial infarction.
↵* The reported ischemic and bleeding risks were all statistically significant except for the reduction of cardiovascular mortality of prasugrel compared with clopidogrel.
↵† PLATO trial provided 85% of patients to total number.
Model Derived population Score variables Score description Limitations CRUSADE (30) 71 277 community-treated patients with NSTEMI Hematocrit, creatinine clearance, baseline heart rate, baseline systolic blood pressure, female sex, signs of CHF on presentation, previous vascular disease and diabetes mellitus Each independent variable was assigned weighted integers according to its coefficient value in the regression model. The sum of the weighted integers (range 1 to 100 points) estimates the risk of in-hospital major bleeding, with a curvilinear relation between CRUSADE bleeding score and predicted probabilities of major bleeding Patients who died within 48 hours were excluded and early bleeding events may be underestimated. Patients on oral anticoagulation were excluded; similarly those with previous bleeding events or bleeding disorders were not included. CRUSADE is designed to predict in-hospital bleeding events ACUITY (31) 17 421 patients with ACS (UA, NSTEMI and STEMI) Age, female sex, serum creatinine, white blood cell count, anemia, NSTEMI, STEMI and the use of heparin plus glycoprotein IIb/IIIa inhibitor (rather than bivalirudin alone) Each independent variable was assigned weighted integers according to its coefficient value in the regression model. The sum of the weighted integers (range 1 to 52 points) estimates the risk of 30-day non-CABG major bleeding, with curvilinear relation between ACUITY bleeding score and predicted probabilities of bleeding Posthoc analysis of patients included in 2 RCTs. Potential variables of interest were not available to be incorporated in the model. Potent P2Y12 inhibitors were not studied REACH (32) 64 589 at risk of CAD or with stable CAD Age, peripheral arterial disease, CHF, diabetes, hypertension, smoking, antiplatelets, oral anticoagulants, hypercholesterolemia Each factor was assigned a single point, except for CHF, hypertension, smoking and non-ASA antiplatelet therapy, which were assigned 2 points. Oral anticoagulation or DAPT were assigned 4 points. A score > 10 was associated with 6-fold increase in risk of serious bleeding over 2 years The definition of serious bleeding used for the analyses was either a hemorrhagic stroke or bleeding leading to both hospitalization and transfusion. This may underestimate the rate of major bleeding events. Data regarding potent P2Y12 inhibitors were limited. The exposure to oral anticoagulation was extrapolated and did not account for potential changes over study follow-up DAPT (33)* 11 648 patients who tolerated DAPT for 1 year without ischemic or bleeding events Age, cigarette smoking, diabetes mellitus, MI at presentation, previous PCI or previous MI, paclitaxel-eluting stent, stent diameter < 3 mm, CHF or LVEF < 30%, and vein graft stent Each variable was assigned a single point except for age (65 to < 75 yr and ≥ 75 yr, for which patients were assigned −1 or −2, respectively). Those with CHF, LVEF or vein graft stent were assigned 2 points. Total scores ranged from −2 to 10, and those with scores ≥ 2 were considered high risk and extended DAPT was recommended. Patients with low scores (< 2) were considered low risk and extended DAPT was not recommended DAPT score showed moderate accuracy in the derivation and validation cohort. It is designed to inform the duration of DAPT rather than predicting future bleeding events PARIS (34) 4190 patients treated with DES (almost 60% had stable presentation) Age, body mass index, triple therapy at discharge, anemia, current smoking and renal dysfunction An integer-based risk score was developed for major bleeding (and ischemic events) at 2 years by assigning each variable a score of 2, except for anemia (score of 3) and age (higher score proportional to older patients). The score ranges from 0 to14 and ≥ 8 is considered high bleeding risk Most patients were treated with clopidogrel, which limits generalizability to potent P2Y12 inhibitors. Duration of DAPT was not randomized and decision to stop antiplatelet was according to the clinician’s discretion PRECISE-DAPT (35)* 14 963 patients treated with DAPT after PCI were pooled from 8 RCTs with independent adjudication of events Age, creatinine clearance, hemoglobin, white blood cell count and previous spontaneous bleeding. Independent predictors of bleeding events that were identified in the multivariate regression model were assigned points based on the magnitude of association of each predictor with bleeding. A score ≥ 25 is considered HBR, and extended DAPT has been associated with increased bleeding in this group, unlike patients with low scores. PRECISE-DAPT showed improved integrated discrimination and reclassification performance compared with the PARIS score The accuracy of the model in the validation cohort ranged from moderate to good. Frailty was not included as part of the risk model. Most patients were treated with clopidogrel and those on oral anticoagulation were excluded. Prediction of bleeding events in patients on prasugrel was poor ARC-HBR trade-off model (36), (37) 6641 patients who underwent PCI and were identified as HBR were pooled from 6 studies Age, hemoglobin, renal dysfunction, liver disease, cancer, planned major surgery, COPD, current smoker, complex PCI procedure, oral anticoagulation at discharge Variables were classified as a major or minor criterion for HBR. Major criterion is considered to confer risk of major bleeding of ≥ 4% or ≥ 1% intracranial hemorrhage at 1 year. This score outperformed PARIS and PRECISE-DAPT (alternative model without white blood cell count) The criteria used were modified from those proposed in the ARC consensus to allow the use of available data. Infrequent, but wellrecognized, predictors were pooled as a single variable in the model (i.e., liver disease, cancer and planned surgery) PRAISE (38)* 19 826 patients presenting with ACS from 2 registries Age, sex, diabetes, hypertension, hyperlipidemia, PAD, eGFR, previous MI, previous PCI, previous CABG, previous stroke, previous bleeding, malignancy, STEMI, LVEF, multivessel disease, complete revascularization, vascular access, DES and treatment with BBs, ACE inhibitors, ARBs, statins, oral anticoagulation and PPIs Four machine learning models that used different classifiers were developed to predict occurrence of all-cause death, recurrent MI and major bleeding 1 year after discharge. Each model’s performance was assessed using a range of learning metrics and the best performing model was selected. When calculated, PRAISE provides 3 outcomes of the calculated score for death, MI, and major bleeding. It was not possible to fully compare PRAISE with PARIS or PRECISE-DAPT given the insufficient clinical data. Although PRAISE has been prospectively validated in external cohorts, it has not been used in RCTs to aid decision-making of DAPT duration Note: ACE = angiotensin-converting enzyme, ACS = acute coronary syndrome, ACUITY = Acute Catheterization and Urgent Intervention Triage Strategy, ARB = angiotensin-receptor blocker, ARC = Academic Research Consortium, ASA = acetylsalicylic acid, BB = beta-blocker, CABG = coronary artery bypass graft, CAD = coronary artery disease, CHF = congestive heart failure, COPD = chronic obstructive pulmonary disease, CRUSADE = Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines, DAPT = dual antiplatelet therapy, DES = drug-eluting stent, HBR = high bleeding risk, eGFR = estimated glomerular filtration rate, LVEF = left ventricle ejection fraction, MI = myocardial infarction, NSTEMI = non-ST segment elevation myocardial infarction, PAD = periphral artery disease, PARIS = Patterns of Nonadherence to Antiplatelet Regimen In Stented Patients, PCI = percutaneous coronary intervention, PPI = proton pump inhibitor, PRAISE = Predicting with Artificial Intelligence Risk after Acute Coronary Syndromes, PRECISE-DAPT = Predicting Bleeding Complications in Patients Undergoing Stent Implantation and Subsequent Dual Antiplatelet Therapy, RCT = randomized controlled trial, REACH = Reduction of Atherothrombosis for Continued Health Registry, STEMI = ST-segment elevation myocardial infarction, UA = unstable angina.
↵* DAPT score is available at https://tools.acc.org/daptriskapp/#!/content/calculator/, PRECISE-DAPT is available at http://precisedaptscore.com/predapt/ and PRAISE is available at https://praise.hpc4ai.it/.
- Table 3:
Management of bleeding events in patients with acute coronary syndrome receiving antithrombotic therapy
Bleeding event Event description Antithrombotic treatment modification Original treatment Modification Trivial bleeding A bleeding event not requiring medical attention or further evaluation (e.g., skin bruising, self-resolving epistaxis, minimal conjunctival bleeding) DAPT Continue DAPT
Concomitant OAC* Consider continuation of the regimen or skip a single dose of OAC
Mild bleeding A bleeding event requiring medical attention without need for hospital admission (e.g., major epistaxis, moderate conjunctival bleeding, genitourinary or gastrointestinal bleeding without substantial blood loss, mild hemoptysis) DAPT Continue DAPT
Consider shortening DAPT or de-escalation to a less potent P2Y12 inhibitor
Concomitant OAC* In patients on VKA: consider holding drug until INR < 2
In patients on DOAC: skip a single dose
In patients on TT: consider switching to dual therapy (clopidogrel and OAC)
Moderate bleeding A bleeding event requiring hospital admission or associated with substantial blood loss (≥ 3 mmol/L hemoglobin) without hemodynamic instability (e.g., genitourinary, respiratory, upper or lower gastrointestinal bleeding with substantial blood loss or requiring transfusion) DAPT Consider stopping DAPT and continuing with a single P2Y12 inhibitor
Resume DAPT within 3 days if considered safe to do so
Consider shortening DAPT or de-escalation to a less potent P2Y12 inhibitor
Concomitant OAC* Consider stopping OAC or reversing VKA with vitamin K (unless CHA2DS2-VASc ≥ 4 or a cardiac assist device or mechanical heart valve is present)
If DOAC was taken within 2–4 hours, charcoal or dialysis (for patients on dabigatrtan) can be used
Consider resuming treatment within 1 week, if patient is clinically stable
In patients on VKA: consider a target INR 2.0–2.5 (unless mechanical heart valve or cardiac assist device is present)
In patients on DOAC: consider the lowest effective dose
In patients on TT: consider switching to dual therapy (clopidogrel and OAC)
Severe bleeding A bleeding event associated with severe blood loss (≥ 5 mmol/L hemoglobin) in a hemodynamically unstable patient requiring hospital admission (e.g., severe genitourinary, respiratory or gastrointestinal bleeding, bleeding into critical spaces such as pericardium, retroperitoneum, intraocular spinal or intracranial spaces) DAPT Consider stopping DAPT and continue with SAPT (preferably with P2Y12 inhibitor)
Consider stopping all antithrombotic agents if bleeding persists
Once bleeding has ceased, reassess the need for DAPT or SAPT; if DAPT is resumed, consider shortening length of treatment or de-escalating to a less potent P2Y12 inhibitor
Concomitant OAC* Stop or reverse OAC until bleeding stops (except for patients with an extreme thrombotic risk, i.e., with a mechanical heart valve in mitral position or cardiac assist device)
In patients on VKA: administer FFP or 4F-PCC
In patients on DOAC: administer 4F-PPC
In patients on dabigatran: consider administering idarucizumab
Consider resuming treatment within 1 week, if clinically stable
In patients on VKA: consider target INR of 2.0–2.5 (except for patients with mechanical heart valves and cardiac assist devices)
In patients on DOAC: consider the lowest effective dose
In patients on TT: consider switching to dual therapy (clopidogrel and OAC)
Life-threatening bleeding Any severe active bleeding that poses a threat to a patient’s life (e.g., massive genitourinary, respiratory or gastrointestinal bleeding, active intracranial, spinal or intraocular hemorrhage, any bleeding causing hemodynamic instability) DAPT Stop all antithrombotic agents immediately
Once bleeding has ceased, reassess the need for DAPT or SAPT, preferably with clopidogrel (particularly in patients who had upper GI bleeding)
Concomitant OAC* Stop and reverse OAC
In patients on VKA: use FFP or 4F-PCC
In patients on dabigatran: consider administering idarucizumab
Note: 4F-PCC = 4-factor prothrombin complex concentrate, ACS = acute coronary syndrome, CHA2DS2-VASc = score that evaluates risk of ischemic stroke, DAPT = dual antiplatelet therapy, DOAC = direct oral anticoagulant, FFP = fresh frozen plasma, GI = gastrointestinal, INR = international normalized ratio, OAC = oral anticoagulant, SAPT = single antiplatelet therapy, TT = triple therapy, VKA = vitamin K antagonist.
↵* Concomitant OAC with antiplatelet therapy, including both SAPT and DAPT.
In this issue
{kind=link}
{kind=link}
{kind=link}
Article extras
Article tools



Jump to section
- Article
- What are the options for oral antiplatelet therapy?
- How long should dual antiplatelet therapy be continued?
- How is bleeding risk assessed and managed?
- Can treatment with acetylsalicylic acid be stopped early?
- What are the indications for dual antiplatelet therapy in patients with atrial fibrillation?
- How should antiplatelet agents be switched?
- Conclusion
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

